You might also like
- NonRinse Conditioning-BisharaDocument5 pagesNonRinse Conditioning-Bisharaavanthika krishnarajNo ratings yet
- Bonding and Debonding From Metal To Ceramic: Research and Its Clinical ApplicationDocument13 pagesBonding and Debonding From Metal To Ceramic: Research and Its Clinical Applicationgriffone1No ratings yet
- Self-Etch Vs Etch-And - RinseDocument16 pagesSelf-Etch Vs Etch-And - RinseKarla AlanisNo ratings yet
- Bonding To Atypical Tooth SurfacesDocument4 pagesBonding To Atypical Tooth SurfacesRomit SenNo ratings yet
- TMP CE5 CDocument8 pagesTMP CE5 CFrontiersNo ratings yet
- Enamel Acid Etching - A ReviewDocument8 pagesEnamel Acid Etching - A ReviewSiddharth NairNo ratings yet
- Adhesive Systems in Restorative DentistryDocument6 pagesAdhesive Systems in Restorative DentistryStoian SimonaNo ratings yet
- The Current State of Adhesive DentistryDocument9 pagesThe Current State of Adhesive DentistrymishNo ratings yet
- Ultimate Ceramic Veneers: A Laboratory-Guided Preparation Technique For Minimally Invasive RestorationsDocument17 pagesUltimate Ceramic Veneers: A Laboratory-Guided Preparation Technique For Minimally Invasive RestorationsAlfred OrozcoNo ratings yet
- Microabrasion After 18 Years (Sundfeld)Document6 pagesMicroabrasion After 18 Years (Sundfeld)Bernny DaniloNo ratings yet
- Chapter 5 Fundamental Concepts of Enamel andDocument24 pagesChapter 5 Fundamental Concepts of Enamel andJerome Tolentino TotingNo ratings yet
- Batra 2013Document11 pagesBatra 2013Amee PatelNo ratings yet
- Influence of Operator Experience On in Vitro Bond Strength of Dentin AdhesivesDocument5 pagesInfluence of Operator Experience On in Vitro Bond Strength of Dentin AdhesivesdanielaNo ratings yet
- Re-Establishing Esthetics of Uorosis-Stained Teeth Using Enamel Microabrasion and Dental Bleaching TechniquesDocument10 pagesRe-Establishing Esthetics of Uorosis-Stained Teeth Using Enamel Microabrasion and Dental Bleaching TechniquesCeida Lopez CastillaNo ratings yet
- Influence of Ozone and Paracetic Acid Disinfection On Adhesion of Resilient Liners To Acrylic ResinDocument6 pagesInfluence of Ozone and Paracetic Acid Disinfection On Adhesion of Resilient Liners To Acrylic ResinHoshang AbdelrahmanNo ratings yet
- Australian Dental Journal: Current Aspects On Bonding Effectiveness and Stability in Adhesive DentistryDocument14 pagesAustralian Dental Journal: Current Aspects On Bonding Effectiveness and Stability in Adhesive DentistryGhita HAFFOUNo ratings yet
- Effect LutingDocument8 pagesEffect LutingCristina Androne MihăescuNo ratings yet
- Classification Review of Dental Adhesive Systems: From The IV Generation To The Universal TypeDocument17 pagesClassification Review of Dental Adhesive Systems: From The IV Generation To The Universal Typejuan diegoNo ratings yet
- Ultimate Ceramic Veneers: A Laboratory-Guided Preparation Technique For Minimally Invasive RestorationsDocument17 pagesUltimate Ceramic Veneers: A Laboratory-Guided Preparation Technique For Minimally Invasive RestorationsPablo BenitezNo ratings yet
- Adhesivos UniversalesDocument9 pagesAdhesivos Universalesmaria posadaNo ratings yet
- Yadav 2013Document6 pagesYadav 2013anas dkaliNo ratings yet
- Five-Year Clinical Evaluation of 300 Teeth Restored With Porcelain Laminate Veneers Using Total-Etch and A Modified Self-Etch Adhesive SystemDocument8 pagesFive-Year Clinical Evaluation of 300 Teeth Restored With Porcelain Laminate Veneers Using Total-Etch and A Modified Self-Etch Adhesive SystemEric Arnold dos Santos BritoNo ratings yet
- Effectiveness of Seven Types of Sealants Retention After One YearDocument6 pagesEffectiveness of Seven Types of Sealants Retention After One YearJoseph EneroNo ratings yet
- Operative Dentistry: Dental AdhesionDocument12 pagesOperative Dentistry: Dental AdhesionJohn CenaNo ratings yet
- 10 Frequent Handling Mistakes During Bonding 2017 Orthodontic Applications of BiomaterialsDocument7 pages10 Frequent Handling Mistakes During Bonding 2017 Orthodontic Applications of BiomaterialsFelipe ArceNo ratings yet
- Articulo Ensayo ClinicoDocument5 pagesArticulo Ensayo ClinicoAnyela CABRERA BASUALDONo ratings yet
- Self Etch or Total EtchDocument3 pagesSelf Etch or Total EtchKarlina KrishnaNo ratings yet
- Orthodontic Bonding Review of The LiteratureDocument10 pagesOrthodontic Bonding Review of The LiteratureLiliana Aguilar VillarrealNo ratings yet
- Cementation Protocols For Ceramic RestorationsDocument8 pagesCementation Protocols For Ceramic RestorationsValeria zNo ratings yet
- Enamel Acid Etching - A ReviewDocument8 pagesEnamel Acid Etching - A ReviewAmee PatelNo ratings yet
- Nagar Kar 2019Document11 pagesNagar Kar 2019Jessi RecaldeNo ratings yet
- Sharif - An Overview of Orthodontic Bonding FINALDocument23 pagesSharif - An Overview of Orthodontic Bonding FINALLimasunep JamirNo ratings yet
- 1998 Jod CL Perf-2Document20 pages1998 Jod CL Perf-2Hector Flores SotoNo ratings yet
- Adhesion of Multimode Adhesives To Enamel and Dentin 2017Document9 pagesAdhesion of Multimode Adhesives To Enamel and Dentin 2017Paul AlvarezNo ratings yet
- OVERLAYDocument24 pagesOVERLAYJose Luis Celis100% (3)
- Important Compositional Characteristics in The Clinical Use of Adhesive SystemsDocument9 pagesImportant Compositional Characteristics in The Clinical Use of Adhesive SystemsNaji Z. ArandiNo ratings yet
- Clinical Use of Glass Ionomer Cements A Literature ReviewDocument4 pagesClinical Use of Glass Ionomer Cements A Literature ReviewwzsatbcndNo ratings yet
- Jos 6 129Document7 pagesJos 6 129antonio dlNo ratings yet
- Effects of Direct and Indirect Bonding Techniques PDFDocument9 pagesEffects of Direct and Indirect Bonding Techniques PDFAlvaro ChacónNo ratings yet
- Degradacion de Interfase 2Document25 pagesDegradacion de Interfase 2Sofía TrianaNo ratings yet
- Microfiltracion en CarillasDocument6 pagesMicrofiltracion en CarillasCdjuan GnNo ratings yet
- Teori Pembersihan Gigi Tiruan - EngDocument5 pagesTeori Pembersihan Gigi Tiruan - EngZuhra An Nisa SamudraNo ratings yet
- Comparison of Microleakage of Three Adhesive Systems in Class V Composite Restorations Prepared With Er, Cr:YSGG LaserDocument6 pagesComparison of Microleakage of Three Adhesive Systems in Class V Composite Restorations Prepared With Er, Cr:YSGG LasernisaNo ratings yet
- Effect of Resin Coating and Chlorhexidine On Microleakage of Two Resin Cements After StorageDocument10 pagesEffect of Resin Coating and Chlorhexidine On Microleakage of Two Resin Cements After StorageHisham HameedNo ratings yet
- Joseph 1994Document7 pagesJoseph 1994Setthapong WisarnjarusornNo ratings yet
- Adhesion in Restorative DentistryDocument16 pagesAdhesion in Restorative DentistryIrene MartinezNo ratings yet
- Longevida Adhesivos-5Document25 pagesLongevida Adhesivos-5Camila Conejeros ArriagadaNo ratings yet
- Ultrastructure of The Dentin Adhesive Interface After Acidbase Challenge 2004Document8 pagesUltrastructure of The Dentin Adhesive Interface After Acidbase Challenge 2004Mohamed OudaNo ratings yet
- Ari 16Document5 pagesAri 16mariaNo ratings yet
- Evaluation of Different Enamel Conditioning Techniques For Orthodontic BondingDocument7 pagesEvaluation of Different Enamel Conditioning Techniques For Orthodontic Bondingosama-alaliNo ratings yet
- 36 Irie 2004 Immediate Performance of Self Etching Vs System Adhesives With Multiple Light Activate RestorativesDocument8 pages36 Irie 2004 Immediate Performance of Self Etching Vs System Adhesives With Multiple Light Activate RestorativesCherifNo ratings yet
- Frequently Asked Questions in Composite Restorative Dentistry PDFDocument7 pagesFrequently Asked Questions in Composite Restorative Dentistry PDFDavid ColonNo ratings yet
- New Adhesives and Bonding Techniques. Why and When?: Nicola ScottiDocument12 pagesNew Adhesives and Bonding Techniques. Why and When?: Nicola ScottiDr. Naji ArandiNo ratings yet
- Implementing Sandwich Technique With RMGI: (Resin-Modified Glass-Ionomer)Document8 pagesImplementing Sandwich Technique With RMGI: (Resin-Modified Glass-Ionomer)Firma Nurdinia DewiNo ratings yet
- Esthetic Dentistry and Ceramic Restoration, 1edDocument331 pagesEsthetic Dentistry and Ceramic Restoration, 1edMariana RaduNo ratings yet
- The "Index Technique" in Worn Dentition - A New and Conservative ApproachDocument32 pagesThe "Index Technique" in Worn Dentition - A New and Conservative ApproachFilipe Queiroz100% (2)
- Comparacion Micro CTDocument7 pagesComparacion Micro CTandrey eduardo quintero arevaloNo ratings yet
- Dentin Bonding Agents LectureDocument97 pagesDentin Bonding Agents Lectureaakriti100% (1)
- Ultimate Ceramic Veneer A Laboratory-Gui PDFDocument16 pagesUltimate Ceramic Veneer A Laboratory-Gui PDFHector Flores SotoNo ratings yet
- Jia and Mandibular AsymmetryDocument8 pagesJia and Mandibular AsymmetrynomanNo ratings yet
- Types of Occlusal Splint in Management of Temporomandibular Disorders TMD 2167 7921 1000176Document4 pagesTypes of Occlusal Splint in Management of Temporomandibular Disorders TMD 2167 7921 1000176INGRID DAYAN JIMENEZ VENEGASNo ratings yet
- Systematic Review by EmmaDocument11 pagesSystematic Review by EmmanomanNo ratings yet
- Different Types of Occlusal Splint Used in Management of Temporomandibular Joint Disorders-A ReviewDocument8 pagesDifferent Types of Occlusal Splint Used in Management of Temporomandibular Joint Disorders-A ReviewnomanNo ratings yet
- The Clinical Diagnosis of Temporomandibula. Disorders in The Orthodontic PatmntDocument10 pagesThe Clinical Diagnosis of Temporomandibula. Disorders in The Orthodontic PatmntnomanNo ratings yet
- Idiopathic Condylar Resorption: Diagnosis, Treatment Protocol, and OutcomesDocument11 pagesIdiopathic Condylar Resorption: Diagnosis, Treatment Protocol, and OutcomesCatherine NocuaNo ratings yet
- Radiographic Diagnosis of Root Resorption in Relation To OrthodonticsDocument7 pagesRadiographic Diagnosis of Root Resorption in Relation To OrthodonticsnomanNo ratings yet
- 28 143801 Parameters of CareDocument2 pages28 143801 Parameters of CarenomanNo ratings yet
- To Be Copied: About Periodontal (Gum) DiseaseDocument2 pagesTo Be Copied: About Periodontal (Gum) DiseasenomanNo ratings yet
- Practice: The Interdisciplinary Management of Hypodontia: OrthodonticsDocument6 pagesPractice: The Interdisciplinary Management of Hypodontia: OrthodonticsJawad TariqNo ratings yet
- 104 - 093615 - The Diabetes Times MiDocument2 pages104 - 093615 - The Diabetes Times MinomanNo ratings yet
- BSP BSPD Perio Guidelines For The Under 18sDocument1 pageBSP BSPD Perio Guidelines For The Under 18sNaomiAnneDomnicNo ratings yet
- 39 143748 Bpe2011-2Document2 pages39 143748 Bpe2011-2anees jamalNo ratings yet
- CephDocument1 pageCephnomanNo ratings yet
- Twinblocks Part 1 AJODODocument10 pagesTwinblocks Part 1 AJODOSara SaedNo ratings yet
- Skeletal and Dentoalveolar Effects ofDocument7 pagesSkeletal and Dentoalveolar Effects ofnomanNo ratings yet
- Ectopic Eruption of The First Permanent Molar: Predictive Factors For Irreversible OutcomeDocument9 pagesEctopic Eruption of The First Permanent Molar: Predictive Factors For Irreversible OutcomenomanNo ratings yet
- 2003.john H. Warford JR - Prediction of Maxillary Canine Impaction UsingDocument5 pages2003.john H. Warford JR - Prediction of Maxillary Canine Impaction UsingLuis HerreraNo ratings yet
- Association Between Root Resorption and Tooth Development: A Quantitative Clinical StudyDocument9 pagesAssociation Between Root Resorption and Tooth Development: A Quantitative Clinical StudynomanNo ratings yet
- Overcoming Compact Bone Resistance To Tooth Movement: Special ArticleDocument6 pagesOvercoming Compact Bone Resistance To Tooth Movement: Special ArticlenomanNo ratings yet
- Precautions and Recommendations For Orthodontic Settings During The COVID-19 Outbreak: A ReviewDocument7 pagesPrecautions and Recommendations For Orthodontic Settings During The COVID-19 Outbreak: A ReviewsmritiNo ratings yet
- Mechanics of Tooth Movement: or SmithDocument14 pagesMechanics of Tooth Movement: or SmithRamesh SakthyNo ratings yet
- Nano TechnologyDocument6 pagesNano Technologynoman100% (1)
- Miniscrews Failure Rate in Orthodontics - Systematic Review and Meta-AnalysisDocument12 pagesMiniscrews Failure Rate in Orthodontics - Systematic Review and Meta-AnalysisnomanNo ratings yet
- Mechanics of Tooth Movement: or SmithDocument14 pagesMechanics of Tooth Movement: or SmithRamesh SakthyNo ratings yet
- Maxillary First Molar With 7 Root Canals Diagnosed Using Cone-Beam Computed TomographyDocument5 pagesMaxillary First Molar With 7 Root Canals Diagnosed Using Cone-Beam Computed TomographynomanNo ratings yet
- Forensic Imaging: SciencedirectDocument6 pagesForensic Imaging: SciencedirectnomanNo ratings yet
- The Hyoid Triangle. Bibby y Preston PDFDocument6 pagesThe Hyoid Triangle. Bibby y Preston PDFAnahi AcostaNo ratings yet
- Miniscrews Failure Rate in Orthodontics - Systematic Review and Meta-AnalysisDocument12 pagesMiniscrews Failure Rate in Orthodontics - Systematic Review and Meta-AnalysisnomanNo ratings yet
- Cleft Lip and Palate Indices: A Review: Anju Agrawal, Rabindra Man Shrestha and Praveen MishraDocument9 pagesCleft Lip and Palate Indices: A Review: Anju Agrawal, Rabindra Man Shrestha and Praveen MishranomanNo ratings yet
- General Biology 1 Q1 Week 7 BiomoleculesDocument5 pagesGeneral Biology 1 Q1 Week 7 BiomoleculesJohn Brylle UrsuaNo ratings yet
- Seperation Techniques PDFDocument232 pagesSeperation Techniques PDFAmitranjan KarNo ratings yet
- Botany J-Adhikary Enzymology 4Document9 pagesBotany J-Adhikary Enzymology 4Dharmesh R.DNo ratings yet
- Acs JPCC 8b06841Document13 pagesAcs JPCC 8b06841Septian Perwira YudhaNo ratings yet
- Soap PreperationDocument13 pagesSoap PreperationKatrina MillerNo ratings yet
- Clean in Place Guide LinesDocument8 pagesClean in Place Guide LinesArunachalam NarayananNo ratings yet
- ChitosanDocument7 pagesChitosanYonatan AdiNo ratings yet
- Safety Data Sheet NALCO® 8140: Section 1. Product and Company IdentificationDocument9 pagesSafety Data Sheet NALCO® 8140: Section 1. Product and Company IdentificationU.s. Ezhil ArivudainambiNo ratings yet
- Paper 1Document7 pagesPaper 1Akash Kumar UpadhyayNo ratings yet
- Design Concentratiion-Class B FuelsDocument14 pagesDesign Concentratiion-Class B Fuelsmiguel angel garciaNo ratings yet
- Bio-Lubricant Production From Vegetable Oil and Animal Fat: International UniversityDocument48 pagesBio-Lubricant Production From Vegetable Oil and Animal Fat: International UniversityKiệtNguyễnNo ratings yet
- Electron Ionization Electron Ionization (EI, Formerly Known As Electron Impact) Is An Ionization MethodDocument12 pagesElectron Ionization Electron Ionization (EI, Formerly Known As Electron Impact) Is An Ionization MethodDiego RibeiroNo ratings yet
- Sow Combined Science Year 9 - 2+3 Programme - v2Document37 pagesSow Combined Science Year 9 - 2+3 Programme - v2Airul YantiNo ratings yet
- P Block (English)Document207 pagesP Block (English)Aditya YadavNo ratings yet
- Chemical Formula NamesDocument8 pagesChemical Formula NamesJeni PNo ratings yet
- Solid StatesDocument4 pagesSolid StatesAbhi RamNo ratings yet
- Eglin SteelDocument3 pagesEglin SteelShaun LeeNo ratings yet
- Glycine Leaching Kinetics of Chalcocite-92939546Document10 pagesGlycine Leaching Kinetics of Chalcocite-92939546Chad IrungNo ratings yet
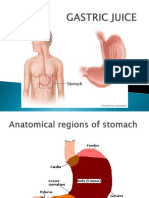
- Gastric JuiceDocument21 pagesGastric JuiceSohail AhamdNo ratings yet
- Preparing and Using Cobalt Chloride Indicator PapersDocument1 pagePreparing and Using Cobalt Chloride Indicator PapersJoko SusiloNo ratings yet
- Chemistry Lab Manual 2Document21 pagesChemistry Lab Manual 2Nischay SanjayNo ratings yet
- 04 Hydrogen PeroxideDocument10 pages04 Hydrogen Peroxidemacastillof100% (1)
- Wacker PolymeDocument6 pagesWacker PolymeForeverNo ratings yet
- Quiz 2 Micropara LecDocument5 pagesQuiz 2 Micropara LecAbby CruzNo ratings yet
- Manganese Deposits of Cuba: Bulletin 935-BDocument31 pagesManganese Deposits of Cuba: Bulletin 935-BMuhammad ZakyNo ratings yet
- 2000-2019 Nesa Chemistry Advanced Level-1Document269 pages2000-2019 Nesa Chemistry Advanced Level-1Jeff AlbaNo ratings yet
- Fr3 Synthesis of 1 Phenylazo 2 NaphtholDocument4 pagesFr3 Synthesis of 1 Phenylazo 2 NaphtholRon Andrei Soriano0% (1)
- Indigo Prodn. From Phenyl-Glycine Carboxylic Acid Salt - by Fusion in Mixed Potassium Hydroxide and Sodium Hydroxide Melt, Then OxidnDocument4 pagesIndigo Prodn. From Phenyl-Glycine Carboxylic Acid Salt - by Fusion in Mixed Potassium Hydroxide and Sodium Hydroxide Melt, Then OxidnCillian CreedonNo ratings yet
- Metallurgical Requirements of Copper Smelting Refractories in Refining'Document3 pagesMetallurgical Requirements of Copper Smelting Refractories in Refining'VictorNo ratings yet
- C Sol Ch-20 Organic+ChemistryDocument4 pagesC Sol Ch-20 Organic+Chemistrymysoftinfo.incNo ratings yet
- House Rules: How to Decorate for Every Home, Style, and BudgetFrom EverandHouse Rules: How to Decorate for Every Home, Style, and BudgetNo ratings yet
- Clean Mama's Guide to a Healthy Home: The Simple, Room-by-Room Plan for a Natural HomeFrom EverandClean Mama's Guide to a Healthy Home: The Simple, Room-by-Room Plan for a Natural HomeRating: 5 out of 5 stars5/5 (2)
- Eat That Frog!: 21 Great Ways to Stop Procrastinating and Get More Done in Less TimeFrom EverandEat That Frog!: 21 Great Ways to Stop Procrastinating and Get More Done in Less TimeRating: 4.5 out of 5 stars4.5/5 (3225)
- The Encyclopedia of Spices & Herbs: An Essential Guide to the Flavors of the WorldFrom EverandThe Encyclopedia of Spices & Herbs: An Essential Guide to the Flavors of the WorldRating: 3.5 out of 5 stars3.5/5 (5)
- Success at Home with ADHD.: Practical Organization Strategies to Make Your Life Easier.From EverandSuccess at Home with ADHD.: Practical Organization Strategies to Make Your Life Easier.Rating: 4 out of 5 stars4/5 (17)
- The Joy of Less: A Minimalist Guide to Declutter, Organize, and SimplifyFrom EverandThe Joy of Less: A Minimalist Guide to Declutter, Organize, and SimplifyRating: 4 out of 5 stars4/5 (277)
- How To Win Friends And Influence PeopleFrom EverandHow To Win Friends And Influence PeopleRating: 4.5 out of 5 stars4.5/5 (6512)
- Lightly: How to Live a Simple, Serene & Stress-free LifeFrom EverandLightly: How to Live a Simple, Serene & Stress-free LifeRating: 4 out of 5 stars4/5 (12)
- Root to Leaf: A Southern Chef Cooks Through the SeasonsFrom EverandRoot to Leaf: A Southern Chef Cooks Through the SeasonsRating: 4.5 out of 5 stars4.5/5 (3)
- 100 Micro Amigurumi: Crochet patterns and charts for tiny amigurumiFrom Everand100 Micro Amigurumi: Crochet patterns and charts for tiny amigurumiRating: 5 out of 5 stars5/5 (2)
- How to Keep House While Drowning: A Gentle Approach to Cleaning and OrganizingFrom EverandHow to Keep House While Drowning: A Gentle Approach to Cleaning and OrganizingRating: 4.5 out of 5 stars4.5/5 (844)
- The Gentle Art of Swedish Death Cleaning: How to Free Yourself and Your Family from a Lifetime of ClutterFrom EverandThe Gentle Art of Swedish Death Cleaning: How to Free Yourself and Your Family from a Lifetime of ClutterRating: 4 out of 5 stars4/5 (467)
- A Girl and Her Greens: Hearty Meals from the GardenFrom EverandA Girl and Her Greens: Hearty Meals from the GardenRating: 3.5 out of 5 stars3.5/5 (7)
- Crochet Impkins: Over a million possible combinations! Yes, really!From EverandCrochet Impkins: Over a million possible combinations! Yes, really!Rating: 4.5 out of 5 stars4.5/5 (10)
- Crochet with London Kaye: Projects and Ideas to Yarn Bomb Your LifeFrom EverandCrochet with London Kaye: Projects and Ideas to Yarn Bomb Your LifeRating: 5 out of 5 stars5/5 (1)
- Aristotle and Dante Discover the Secrets of the UniverseFrom EverandAristotle and Dante Discover the Secrets of the UniverseRating: 4.5 out of 5 stars4.5/5 (2341)
- Crochet Zodiac Dolls: Stitch the horoscope with astrological amigurumiFrom EverandCrochet Zodiac Dolls: Stitch the horoscope with astrological amigurumiRating: 4 out of 5 stars4/5 (3)
- The Martha Manual: How to Do (Almost) EverythingFrom EverandThe Martha Manual: How to Do (Almost) EverythingRating: 4 out of 5 stars4/5 (11)
- Mini Farming: Self-Sufficiency on 1/4 AcreFrom EverandMini Farming: Self-Sufficiency on 1/4 AcreRating: 4 out of 5 stars4/5 (76)
- The Fitness Mindset: Eat for energy, Train for tension, Manage your mindset, Reap the resultsFrom EverandThe Fitness Mindset: Eat for energy, Train for tension, Manage your mindset, Reap the resultsRating: 4.5 out of 5 stars4.5/5 (31)
- The Hidden Life of Trees: What They Feel, How They CommunicateFrom EverandThe Hidden Life of Trees: What They Feel, How They CommunicateRating: 4 out of 5 stars4/5 (1002)
- Minimalism: Minimalism for Beginners. How to Live Happy While Needing Less in This Modern Material WorldFrom EverandMinimalism: Minimalism for Beginners. How to Live Happy While Needing Less in This Modern Material WorldRating: 4.5 out of 5 stars4.5/5 (39)
- Wild Witchcraft: Folk Herbalism, Garden Magic, and Foraging for Spells, Rituals, and RemediesFrom EverandWild Witchcraft: Folk Herbalism, Garden Magic, and Foraging for Spells, Rituals, and RemediesRating: 5 out of 5 stars5/5 (32)
- The Cottage Fairy Companion: A Cottagecore Guide to Slow Living, Connecting to Nature, and Becoming Enchanted AgainFrom EverandThe Cottage Fairy Companion: A Cottagecore Guide to Slow Living, Connecting to Nature, and Becoming Enchanted AgainRating: 5 out of 5 stars5/5 (15)
- Dream Sewing Spaces: Design & Organization for Spaces Large & SmallFrom EverandDream Sewing Spaces: Design & Organization for Spaces Large & SmallRating: 4 out of 5 stars4/5 (24)