You might also like
- Behaviour Tracking Chart With Possible Function 1Document1 pageBehaviour Tracking Chart With Possible Function 1crnoorNo ratings yet
- Personality DisordersDocument63 pagesPersonality DisordersEcel AggasidNo ratings yet
- Neuropsychology Bordeline Personality RDocument5 pagesNeuropsychology Bordeline Personality RJennie VargasNo ratings yet
- Wellways Fact Sheet BPDDocument4 pagesWellways Fact Sheet BPDJonty ArputhemNo ratings yet
- PsychosisDocument2 pagesPsychosisGrace LNo ratings yet
- Over Coming The Darkness, Advancing Community Based Health CareDocument517 pagesOver Coming The Darkness, Advancing Community Based Health CareBasil FletcherNo ratings yet
- BPD in Young PeopleDocument8 pagesBPD in Young PeopleMaria Von ShaftNo ratings yet
- Romantic Love Vs Drug Addiction May InspireDocument12 pagesRomantic Love Vs Drug Addiction May InspireD Gonzalez GarciaNo ratings yet
- Borderline Personality Disorder - 0Document8 pagesBorderline Personality Disorder - 0Vanshla GuptaNo ratings yet
- Behaviour Support Plan Writing TipsDocument5 pagesBehaviour Support Plan Writing TipsWilly ManishNo ratings yet
- Orderline Ersonality Isorder: Patricia Lam, Ollivia Perea, Nancy Phan & Maribel Ocampo Period 4Document13 pagesOrderline Ersonality Isorder: Patricia Lam, Ollivia Perea, Nancy Phan & Maribel Ocampo Period 4api-277488150100% (1)
- How To Use Self-Compassion To Stop Self-BlamingDocument5 pagesHow To Use Self-Compassion To Stop Self-Blamingjacob100% (1)
- ManningHealing Hearts Conference 11.10.12-1 PDFDocument42 pagesManningHealing Hearts Conference 11.10.12-1 PDFSvetlana RadovanovicNo ratings yet
- Borderline Personality Disorder: Raising Questions, Finding AnswersDocument4 pagesBorderline Personality Disorder: Raising Questions, Finding AnswerslalichompyNo ratings yet
- Part 1: An Introduction To DBTDocument27 pagesPart 1: An Introduction To DBTsmileyfaces6534No ratings yet
- A Case Study About Severe Borderline Personality Disorder.: August 2020Document12 pagesA Case Study About Severe Borderline Personality Disorder.: August 2020Aimen MurtazaNo ratings yet
- CopingskillsDocument1 pageCopingskillsapi-504044748No ratings yet
- The Emotional Pain and Distress of Borderline Personality DisorderDocument9 pagesThe Emotional Pain and Distress of Borderline Personality Disorderme13No ratings yet
- Questions For Patients in The Precontemplation and ContemplatDocument10 pagesQuestions For Patients in The Precontemplation and ContemplatSteveEpsteinNo ratings yet
- Borderline Personality DisorderDocument9 pagesBorderline Personality DisorderSiva Nandhan0% (1)
- BPDDocument2 pagesBPDriffs_ahoyNo ratings yet
- Exploring The Relationship Between Non Suicidal Self-Injury and Borderline Personality Traits in Young AdultsDocument9 pagesExploring The Relationship Between Non Suicidal Self-Injury and Borderline Personality Traits in Young Adultsme13No ratings yet
- Attachment and Borderline Personality DisorderDocument18 pagesAttachment and Borderline Personality Disorderme13No ratings yet
- The Guidebook To HappinessDocument31 pagesThe Guidebook To HappinesskhawarayubNo ratings yet
- Choosing Sleep: An Acceptance and Commitment Therapy CourseDocument27 pagesChoosing Sleep: An Acceptance and Commitment Therapy CourseKitty G K'nkoNo ratings yet
- Cause and Effect of Broken RelationshipDocument18 pagesCause and Effect of Broken Relationshipshafi0% (1)
- 8 Dimensions Exercise Handout W-ResourcesDocument2 pages8 Dimensions Exercise Handout W-ResourcesMaricyaWilliamsNo ratings yet
- Motiv8 HandbookDocument52 pagesMotiv8 HandbookDEDIHNo ratings yet
- Contoh Challenging Negative ThoughtDocument1 pageContoh Challenging Negative Thoughtkezia ausieNo ratings yet
- MindfulnessDocument18 pagesMindfulnessJoshua RevanthNo ratings yet
- Borderline Personality Disorder Write Up 2Document8 pagesBorderline Personality Disorder Write Up 2Sreejita GhoshNo ratings yet
- Treatment of Borderline Personality Disorder Kenneth N Levy PDFDocument18 pagesTreatment of Borderline Personality Disorder Kenneth N Levy PDFdrguillermomedinaNo ratings yet
- DBT NotesDocument15 pagesDBT NotesYudhajit RoychowdhuryNo ratings yet
- CNL-624: Self-Care Assessment and Reflection: Week 2Document6 pagesCNL-624: Self-Care Assessment and Reflection: Week 2api-617533376No ratings yet
- Through Their Eyes WorkbookDocument48 pagesThrough Their Eyes WorkbookTosikur RahmanNo ratings yet
- Adapting CBT For Children With An Autism Spectrum Disorder (ASD)Document3 pagesAdapting CBT For Children With An Autism Spectrum Disorder (ASD)Ina HasimNo ratings yet
- Dysfunctional Beliefs Discriminate Personality DisordersDocument14 pagesDysfunctional Beliefs Discriminate Personality DisordersfelliantiNo ratings yet
- Self Compassion Handout Bereavement Group 2 2016Document6 pagesSelf Compassion Handout Bereavement Group 2 2016PrateekGandhiNo ratings yet
- Calm The FCK Down BookDocument247 pagesCalm The FCK Down BookZeid comline2020No ratings yet
- DBT For Borderline Personality DisorderDocument17 pagesDBT For Borderline Personality Disorderapi-595939801No ratings yet
- APA - DSM 5 Depression Bereavement Exclusion PDFDocument2 pagesAPA - DSM 5 Depression Bereavement Exclusion PDFDaniel NgNo ratings yet
- Sample Module MindfulnessDocument8 pagesSample Module MindfulnessIvanNo ratings yet
- 3 - Relaxation, Presence, Happiness - AcceptanceDocument182 pages3 - Relaxation, Presence, Happiness - AcceptanceAleksandar DjordjevicNo ratings yet
- Borderline & BipolarDocument9 pagesBorderline & BipolarGeorgiana Prisoschi100% (1)
- DBT Made Simple A Step by StepDocument210 pagesDBT Made Simple A Step by StepCarito AlarconNo ratings yet
- Info-What Is Distress IntoleranceDocument1 pageInfo-What Is Distress IntolerancelonstaNo ratings yet
- Ways To Manage Various EmotionDocument4 pagesWays To Manage Various EmotionHannah VisitacionNo ratings yet
- Relapse PreventionDocument1 pageRelapse PreventionAnonymous nYp4sSNo ratings yet
- Morty's Feelings Bingo PDFDocument3 pagesMorty's Feelings Bingo PDFNEW101No ratings yet
- The Storm in My Brain - Kids and Mood Disorders (Bipolar and Depression)Document20 pagesThe Storm in My Brain - Kids and Mood Disorders (Bipolar and Depression)Alina IoanaNo ratings yet
- Anger Management Techniques Howtodealwithandcontrolanger PatientDocument15 pagesAnger Management Techniques Howtodealwithandcontrolanger PatientXico LaranjaNo ratings yet
- Anger Inventory Colored PDFDocument7 pagesAnger Inventory Colored PDFMhidz FirmoNo ratings yet
- Survey of Personal Boundaries PDFDocument2 pagesSurvey of Personal Boundaries PDFmelodyfathiNo ratings yet
- What To Do If You're Feeling SuicidalDocument3 pagesWhat To Do If You're Feeling Suicidalapi-346509377No ratings yet
- Deficits of Cognitive Restructuring in Major Depressive DisorderDocument6 pagesDeficits of Cognitive Restructuring in Major Depressive DisorderIntan YuliNo ratings yet
- A Neurobiological Model of Borderline PersonalityDocument19 pagesA Neurobiological Model of Borderline Personalityme13No ratings yet
- HowtohelpDocument2 pagesHowtohelpapi-360754295100% (1)
- DSM 5 Intellectual Disability Fact SheetDocument2 pagesDSM 5 Intellectual Disability Fact SheetMelissa Ortega MaguiñaNo ratings yet
- Use of Electroconvulsive Therapy To Patient With Schizophrenia and Other Mental IllnessDocument1 pageUse of Electroconvulsive Therapy To Patient With Schizophrenia and Other Mental IllnessJordz PlaciNo ratings yet
- Nursing Degree - EZEKULIE MALLAREDocument1 pageNursing Degree - EZEKULIE MALLAREJordz PlaciNo ratings yet
- Otitis Media DialogueDocument1 pageOtitis Media DialogueJordz PlaciNo ratings yet
- Nursing Degree - EZEKULIE MALLAREDocument1 pageNursing Degree - EZEKULIE MALLAREJordz PlaciNo ratings yet
- Nursing Degree - EZEKULIE MALLAREDocument1 pageNursing Degree - EZEKULIE MALLAREJordz PlaciNo ratings yet
- Otitis Media DialogueDocument1 pageOtitis Media DialogueJordz PlaciNo ratings yet
- Nursing Degree - EZEKULIE MALLAREDocument1 pageNursing Degree - EZEKULIE MALLAREJordz PlaciNo ratings yet
- Recomm Schisto MajanDocument3 pagesRecomm Schisto MajanJordz PlaciNo ratings yet
- Nures ApaDocument1 pageNures ApaJordz PlaciNo ratings yet
- NURSING and SURGICAL MANAGEMENTDocument3 pagesNURSING and SURGICAL MANAGEMENTJordz PlaciNo ratings yet
- LABS Part 2 Jagna SchistosomiasisDocument3 pagesLABS Part 2 Jagna SchistosomiasisJordz PlaciNo ratings yet
- WEEK 14 Ear Ana Dxtic TestsDocument35 pagesWEEK 14 Ear Ana Dxtic TestsJordz PlaciNo ratings yet
- RECOMMENDATIONS Dengue FeverDocument1 pageRECOMMENDATIONS Dengue FeverJordz PlaciNo ratings yet
- Craniotomy Nursing Care PlanDocument5 pagesCraniotomy Nursing Care PlanJordz Placi100% (2)
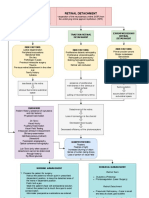
- Retinal Detachment: Traction Retinal Detachment Rhegmatogenous Detachment Exudative/Serous Retinal DetachmentDocument3 pagesRetinal Detachment: Traction Retinal Detachment Rhegmatogenous Detachment Exudative/Serous Retinal DetachmentJordz Placi100% (1)
- Communicable Disease Nursing Ca1 July 2018 5 PDFDocument461 pagesCommunicable Disease Nursing Ca1 July 2018 5 PDFJordz Placi100% (1)
- Muskulo Geria-1Document40 pagesMuskulo Geria-1Jordz PlaciNo ratings yet
- Gi NelecDocument52 pagesGi NelecJordz PlaciNo ratings yet
- LABS Part 2Document3 pagesLABS Part 2Jordz PlaciNo ratings yet
- Gi NelecDocument52 pagesGi NelecJordz PlaciNo ratings yet
- Anatomy and Physiology: Circulatory SystemDocument4 pagesAnatomy and Physiology: Circulatory SystemJordz PlaciNo ratings yet
- Muskulo Geria-1Document40 pagesMuskulo Geria-1Jordz PlaciNo ratings yet
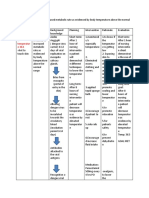
- Assessment Explanation of The Problem Goals and Objectives Interventions Rationale EvaluationDocument9 pagesAssessment Explanation of The Problem Goals and Objectives Interventions Rationale EvaluationJordz PlaciNo ratings yet
- Communicable Disease Nursing Ca1 July 2018 5Document461 pagesCommunicable Disease Nursing Ca1 July 2018 5Jordz PlaciNo ratings yet
- NCP Dengue Fever Hyperthermia and Acute PainDocument4 pagesNCP Dengue Fever Hyperthermia and Acute PainJordz PlaciNo ratings yet
- Fdar TorioDocument3 pagesFdar TorioJordz PlaciNo ratings yet
- Ncenl07 Activity 1Document1 pageNcenl07 Activity 1Jordz PlaciNo ratings yet
- Chapter 21 - Aids2Document31 pagesChapter 21 - Aids2Sanjeevan Aravindan (JEEV)No ratings yet
- Health and Safety Protocols: Dr. Michael Bautista Dr. Ethyl Salvador-CayetanoDocument35 pagesHealth and Safety Protocols: Dr. Michael Bautista Dr. Ethyl Salvador-CayetanoJordz PlaciNo ratings yet
- (884 KB) Eyeball Anatomy Sagittal View - EBM Consult HandoutDocument3 pages(884 KB) Eyeball Anatomy Sagittal View - EBM Consult HandoutJordz PlaciNo ratings yet
- Discussion Method As A Teaching MethodDocument3 pagesDiscussion Method As A Teaching MethodIna Spirit100% (1)
- Activity Completion Report: Activity Title Venue and Location Duration Date Participants Total Expense Fund SourceDocument3 pagesActivity Completion Report: Activity Title Venue and Location Duration Date Participants Total Expense Fund SourceCapoocan PantawidNo ratings yet
- Daily Lesson Plan: Deped Region 7 Poblacion, Talisay City, CebuDocument2 pagesDaily Lesson Plan: Deped Region 7 Poblacion, Talisay City, CebuMarjorie Nervez Sarino Bongato50% (2)
- Every Child Is SpecialDocument4 pagesEvery Child Is SpecialKàtrįńá Jøÿ ÅgùśtïńNo ratings yet
- Research Methodology: Lecture No: 11 (Goodness of Measures)Document30 pagesResearch Methodology: Lecture No: 11 (Goodness of Measures)Muhammad HaroonNo ratings yet
- Crystal Salazar ResumeDocument2 pagesCrystal Salazar Resumeapi-524269323No ratings yet
- 1 SGH PDFDocument5 pages1 SGH PDFoakley bartNo ratings yet
- Frontal Assessment Battery SVUH MedEl ToolDocument2 pagesFrontal Assessment Battery SVUH MedEl ToolHector Leonel Brienza100% (1)
- Hayes. Learning ACT An Acceptance and Commitment Therapy Skills Training Manual For TherapistsDocument466 pagesHayes. Learning ACT An Acceptance and Commitment Therapy Skills Training Manual For TherapistsNuni95% (20)
- M ChatDocument2 pagesM Chatballad3100% (2)
- Motivation TheoriesDocument15 pagesMotivation TheoriesMelNo ratings yet
- Blooms TaxonomyDocument2 pagesBlooms TaxonomySteve Raderman100% (1)
- Project Report Abhishant - PDF Final Version - PDF Done - PDF For PrintDocument57 pagesProject Report Abhishant - PDF Final Version - PDF Done - PDF For PrintAbhi SharmaNo ratings yet
- Gifted Education Curriculum - Gesta, KaeDocument17 pagesGifted Education Curriculum - Gesta, KaeKae Lourdes Gesta II100% (2)
- Social Responsibility Competency ProfilesDocument6 pagesSocial Responsibility Competency ProfilesJohnNo ratings yet
- Correlation Between Students Learning StyleDocument10 pagesCorrelation Between Students Learning StyleSholahhuddin AkkbarNo ratings yet
- I. Title: Project: Oplan Msfog Mentoring Student Skills in Four Fundamental Operations and GraphsDocument3 pagesI. Title: Project: Oplan Msfog Mentoring Student Skills in Four Fundamental Operations and GraphsLem Rada96% (56)
- Competency-Based Language Teaching, Standards and CefrDocument6 pagesCompetency-Based Language Teaching, Standards and CefrgunayNo ratings yet
- Go Tos: Core Values (TIU3)Document4 pagesGo Tos: Core Values (TIU3)api-536422576No ratings yet
- Exogenous Constructivism: Constructivism 2 Main Aspects of ConstructivismDocument4 pagesExogenous Constructivism: Constructivism 2 Main Aspects of ConstructivismMica FloresNo ratings yet
- Placement and InductionDocument14 pagesPlacement and InductionGangadharNo ratings yet
- Pedagogy McqsDocument5 pagesPedagogy McqsSanjeev ChaudharyNo ratings yet
- Individualized Professional Development Plan: GoalsDocument3 pagesIndividualized Professional Development Plan: Goalsapi-548616171No ratings yet
- c1 Multiple Choice - Mindfulness PDFDocument3 pagesc1 Multiple Choice - Mindfulness PDFMaria Martinez SanchezNo ratings yet
- Jennifer Droski: L.L.M.S.WDocument3 pagesJennifer Droski: L.L.M.S.Wapi-453860161No ratings yet
- DLL in Hope 3Document3 pagesDLL in Hope 3Donajei Rica100% (3)
- Emotion-Focused Coping StrategiesDocument2 pagesEmotion-Focused Coping StrategiesMURALI DGNo ratings yet
- Authentic Leadership 2Document32 pagesAuthentic Leadership 2fayçal chehabNo ratings yet
- Work Sampling System For Webpage 4 Year Old WebsiteDocument2 pagesWork Sampling System For Webpage 4 Year Old Websiteapi-225863655No ratings yet
- Performance Appraisal For Sales ManagerDocument6 pagesPerformance Appraisal For Sales ManagerNadim Nik80% (5)