You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5819)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Water Resources and Management in IraqDocument45 pagesWater Resources and Management in IraqRundNo ratings yet
- Microbiology Sessions Project IfmsaDocument8 pagesMicrobiology Sessions Project IfmsaRundNo ratings yet
- First Draft DVT ProphylaxisDocument6 pagesFirst Draft DVT ProphylaxisRundNo ratings yet
- 1) Peripheral BloodDocument21 pages1) Peripheral BloodRundNo ratings yet
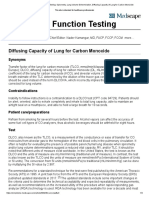
- Pulmonary Function Testing - Spirometry, Lung Volume Determination, Diffusing Capacity of Lung For Carbon MonoxideDocument4 pagesPulmonary Function Testing - Spirometry, Lung Volume Determination, Diffusing Capacity of Lung For Carbon MonoxideRundNo ratings yet
- Rund Aljarrah Dana RidaDocument54 pagesRund Aljarrah Dana RidaRundNo ratings yet
- Pain Management TherapeuticsDocument10 pagesPain Management TherapeuticsRundNo ratings yet
- Fat EmbolismDocument7 pagesFat EmbolismRundNo ratings yet
- Pediatric SurgeryDocument8 pagesPediatric SurgeryRundNo ratings yet
- 3 - Lipids I, II and III PDFDocument60 pages3 - Lipids I, II and III PDFRundNo ratings yet
- Head and Neck SurgeryDocument92 pagesHead and Neck SurgeryAlbert GheorgheNo ratings yet
- Atlas of PET-CT Imaging in Oncology - A Case-Based Guide To Image Interpretation (PDFDrive)Document479 pagesAtlas of PET-CT Imaging in Oncology - A Case-Based Guide To Image Interpretation (PDFDrive)WilverCarbonelLuyo100% (2)
- Bethesda For Thyroid Cytology Part ListDocument6 pagesBethesda For Thyroid Cytology Part ListTanveerNo ratings yet
- Thyroid CaseDocument53 pagesThyroid CaseKenisha HutsonNo ratings yet
- Surgery 1.04 Surgical Diseases of The Thyroid GlandDocument15 pagesSurgery 1.04 Surgical Diseases of The Thyroid GlandjayaeroneNo ratings yet
- Decision Study SorafenibDocument10 pagesDecision Study SorafenibmiguelalmenarezNo ratings yet
- A Nomogram For Lateral Lymph Nodes That Have MetasDocument12 pagesA Nomogram For Lateral Lymph Nodes That Have MetasAbo-ahmed ElmasryNo ratings yet
- Dr. Dr. Tjokorda Gde, SP - PD KEMD-Thyroid NoduleDocument51 pagesDr. Dr. Tjokorda Gde, SP - PD KEMD-Thyroid NodulevinahandoyoNo ratings yet
- Thyroid Tumors: Grades of GoiterDocument2 pagesThyroid Tumors: Grades of GoiterRaisah Bint AbdullahNo ratings yet
- Dokumen - Pub - Werner Amp Ingbars The Thyroid A Fundamental and Clinical Text 11nbsped 2020009060 9781975112967 1975112962 9781975112974 1975112970Document2,428 pagesDokumen - Pub - Werner Amp Ingbars The Thyroid A Fundamental and Clinical Text 11nbsped 2020009060 9781975112967 1975112962 9781975112974 1975112970Verónica Rojas Hernández100% (1)
- SK2 Pertemuan 2Document61 pagesSK2 Pertemuan 2andistinoorfitryNo ratings yet
- Thyroid Cancer Early Detection, Diagnosis, and StagingDocument24 pagesThyroid Cancer Early Detection, Diagnosis, and StagingRum Afida RasfaNo ratings yet
- Medical Record Summary Template (Disability)Document17 pagesMedical Record Summary Template (Disability)Alipit Jr. D. ArmanNo ratings yet
- Pathology BinderDocument406 pagesPathology BinderFaisol KabirNo ratings yet
- Dr. Kunta Setiaji (ThyroidNodule)Document17 pagesDr. Kunta Setiaji (ThyroidNodule)Hasty WahyuniNo ratings yet
- Bethesda Thyroid 2017Document6 pagesBethesda Thyroid 2017Ladipo Temitope AyodejiNo ratings yet
- Thyroid CancerDocument10 pagesThyroid Canceraishaiqbal6789No ratings yet
- TP Thyroid Nodules 1Document59 pagesTP Thyroid Nodules 1Meaw Thitirat SupasilNo ratings yet
- Us de Tiroides y Ganglios LinfDocument17 pagesUs de Tiroides y Ganglios Linfpruebaprueba321765No ratings yet
- Breast+endocrine Surg-EMQ-18Document18 pagesBreast+endocrine Surg-EMQ-18assssadfNo ratings yet
- Reader's Digest USA 06.2021 TDocument128 pagesReader's Digest USA 06.2021 TvnmasterNo ratings yet
- Incidence of Recurrent Laryngeal Nerve Palsy Following Thyroid SurgeryDocument25 pagesIncidence of Recurrent Laryngeal Nerve Palsy Following Thyroid SurgeryAshokNo ratings yet
- Lenvatinib Compared with Sorafenib as a First-Line Treatment for Radioactive Iodine-Refractory, Progressive, Differentiated Thyroid Carcinoma Real-World Outcomes in a Multicenter Retrospective Cohort StudyDocument9 pagesLenvatinib Compared with Sorafenib as a First-Line Treatment for Radioactive Iodine-Refractory, Progressive, Differentiated Thyroid Carcinoma Real-World Outcomes in a Multicenter Retrospective Cohort Studyana carolina hidalgo valeraNo ratings yet
- Surgery of The Thyroid and Parathyroid Glands, OertliDocument352 pagesSurgery of The Thyroid and Parathyroid Glands, Oertliandrruts6318100% (1)
- Ebook Scott Browns Essential Otorhinolaryngology Head Neck Surgery 1St Edition R James A England Online PDF All ChapterDocument65 pagesEbook Scott Browns Essential Otorhinolaryngology Head Neck Surgery 1St Edition R James A England Online PDF All Chapterlawrence.wood865100% (5)
- Solitary Thyroid Nodule: Current Management: Continuing Medical EducationDocument6 pagesSolitary Thyroid Nodule: Current Management: Continuing Medical EducationSathiyamoorthy KarunakaranNo ratings yet
- MRCP EndocrineDocument94 pagesMRCP EndocrineMarwan M.100% (3)
- Subtotal and Total Thyroidectomy: AuthorDocument10 pagesSubtotal and Total Thyroidectomy: AuthorAgustina TambingNo ratings yet
- E.N.T Guide For Medical Students: Neck Examination: Dr. Giovanni Henry ENT Resident 2016Document79 pagesE.N.T Guide For Medical Students: Neck Examination: Dr. Giovanni Henry ENT Resident 2016John M. HemsworthNo ratings yet
- Malignant Thyroid and Parathyroid DisordersDocument48 pagesMalignant Thyroid and Parathyroid DisordersPavan chowdaryNo ratings yet