You might also like
- 1 s2.0 S0169260711003075 Main PDFDocument29 pages1 s2.0 S0169260711003075 Main PDFT.AnithaNo ratings yet
- Best Practice & Research Clinical Anaesthesiology: François Lellouche, MD, PHD, Doctor, Laurent Brochard, MD, ProfessorDocument13 pagesBest Practice & Research Clinical Anaesthesiology: François Lellouche, MD, PHD, Doctor, Laurent Brochard, MD, Professorkittykm chuiNo ratings yet
- Rev A - RespiratoryDocument10 pagesRev A - Respiratorymuhammad irsyad khresna ajiNo ratings yet
- Extubación TemDocument7 pagesExtubación TemMelina AlcaineNo ratings yet
- 7 - Archimedis Trial Validated Model Diabetes - FullDocument9 pages7 - Archimedis Trial Validated Model Diabetes - FullrakeshNo ratings yet
- Asv en NiñosDocument7 pagesAsv en Niñosjuan suarezNo ratings yet
- The Vortex Approach: Management of the Unanticipated Difficult AirwayFrom EverandThe Vortex Approach: Management of the Unanticipated Difficult AirwayRating: 5 out of 5 stars5/5 (1)
- JTD 13 12 6976Document18 pagesJTD 13 12 6976khadeja mowaffakNo ratings yet
- CURE Software PublishedDocument14 pagesCURE Software PublishedMario GuedesNo ratings yet
- Erekat 2019Document16 pagesErekat 2019ayed latifaNo ratings yet
- Asthma Diagnosis SystemDocument10 pagesAsthma Diagnosis SystemAbanum ChuksNo ratings yet
- Newer Modes of Ventilation5Document12 pagesNewer Modes of Ventilation5Saradha PellatiNo ratings yet
- Expert Systems With Applications: Jesmin Nahar, Tasadduq Imam, Kevin S. Tickle, Yi-Ping Phoebe ChenDocument9 pagesExpert Systems With Applications: Jesmin Nahar, Tasadduq Imam, Kevin S. Tickle, Yi-Ping Phoebe ChenRohan SahuNo ratings yet
- Air Distribution Strategy Impact On Operating Room Infection ControlDocument7 pagesAir Distribution Strategy Impact On Operating Room Infection ControlGokhanUNLUNo ratings yet
- Acute Respiratory Distress Syndrome (ARDS) Developed Clinical Pathway: Suggested ProtocolDocument6 pagesAcute Respiratory Distress Syndrome (ARDS) Developed Clinical Pathway: Suggested ProtocolRia sasmitaNo ratings yet
- A Classification and Regression Tree Algorithm For Heart Disease Modeling and PredictionDocument9 pagesA Classification and Regression Tree Algorithm For Heart Disease Modeling and PredictionRavindra MSNo ratings yet
- Censoring in Theory and Practice: Statistical Perspectives and ControversiesDocument16 pagesCensoring in Theory and Practice: Statistical Perspectives and ControversiesSuhail AshrafNo ratings yet
- Characterization of Parameters and Strategies Used by Physical Therapists in Difficult Mechanical Ventilation WeaningDocument6 pagesCharacterization of Parameters and Strategies Used by Physical Therapists in Difficult Mechanical Ventilation WeaningAurora BarreraNo ratings yet
- Multicéntrico Lellouche Et AllDocument7 pagesMulticéntrico Lellouche Et AllterapiafisicapilaresNo ratings yet
- Expert Systems With Applications: Qing Yan, Hongmei Yan, Fei Han, Xinchuan Wei, Tao ZhuDocument5 pagesExpert Systems With Applications: Qing Yan, Hongmei Yan, Fei Han, Xinchuan Wei, Tao ZhuNguyễn Quang HuyNo ratings yet
- Ards PronoDocument10 pagesArds PronoARELHI ROSARIO GARCIA MONROYNo ratings yet
- Swart 2016Document7 pagesSwart 2016TommysNo ratings yet
- Dosimetric Verification of Radiotherapy Treatment Planning Systems: Results of IAEA Pilot StudyDocument10 pagesDosimetric Verification of Radiotherapy Treatment Planning Systems: Results of IAEA Pilot StudyOscar Javier GarciaNo ratings yet
- Protocolos Weaining 2011Document14 pagesProtocolos Weaining 2011perla islasNo ratings yet
- 2017-Core Outcome Sets For Research and Clinical PracticeDocument8 pages2017-Core Outcome Sets For Research and Clinical PracticeAlessandra Aparecida PalacioNo ratings yet
- An Evaluation of A Simple Model For Predicting Surgery - 2021 - Informatics inDocument10 pagesAn Evaluation of A Simple Model For Predicting Surgery - 2021 - Informatics inilc67123No ratings yet
- Resuming Elective Surgery After COVID-19Document13 pagesResuming Elective Surgery After COVID-19mochkurniawanNo ratings yet
- Ventilator Weaning Protocols: Influencing Outcomes and Promoting SuccessDocument32 pagesVentilator Weaning Protocols: Influencing Outcomes and Promoting SuccessarinNo ratings yet
- Hipercapnia PermisivaDocument18 pagesHipercapnia PermisivaARIADNA FABIOLA TRUJILLO RODRÍGUEZNo ratings yet
- A Decision Tree Approach To Airway Management.5Document6 pagesA Decision Tree Approach To Airway Management.5Dominik Chirito PastorNo ratings yet
- Enhanced Recovery After Spine Surgery: A Systematic Review: Neurosurgical FOCUS April 2019Document9 pagesEnhanced Recovery After Spine Surgery: A Systematic Review: Neurosurgical FOCUS April 2019Manuela Martín-Bejarano GarcíaNo ratings yet
- Estratégias de Ventilação em PacientesDocument10 pagesEstratégias de Ventilação em PacientesAllisson GomesNo ratings yet
- Effects of Aggressive and Conservative Strategies For Mechanical Ventilation LiberationDocument9 pagesEffects of Aggressive and Conservative Strategies For Mechanical Ventilation LiberationGurmeet SinghNo ratings yet
- RespiratoryIsolation EMJ2011Document5 pagesRespiratoryIsolation EMJ2011luribe662No ratings yet
- 15-Abbasi KashiyarndiDocument15 pages15-Abbasi KashiyarndiWy TeayNo ratings yet
- Practice Guidelines For Preoperative FastingDocument18 pagesPractice Guidelines For Preoperative FastingTaufik RachmanNo ratings yet
- Design and Material Optimization VentilatorDocument8 pagesDesign and Material Optimization VentilatorHadhi Hassan KhanNo ratings yet
- Sandeep Sir ComputerDocument6 pagesSandeep Sir Computeraditya bNo ratings yet
- Symptoms of DiabetesDocument6 pagesSymptoms of DiabetespriyankaNo ratings yet
- Clinical Reasoning in Neurological Physiotherapy: A Framework For The Management of Patients With Movement DisordersDocument12 pagesClinical Reasoning in Neurological Physiotherapy: A Framework For The Management of Patients With Movement DisordersPredrag NikolicNo ratings yet
- MP 12430Document42 pagesMP 12430Mourya AnkurNo ratings yet
- DocDocument26 pagesDocprojectnewmail.2023No ratings yet
- Independent Dose Calculations Concepts and ModelsDocument104 pagesIndependent Dose Calculations Concepts and ModelsMuhammad Nauman UsmaniNo ratings yet
- Pautas Basadas en La Evidencia para El DesteteDocument23 pagesPautas Basadas en La Evidencia para El DesteteJuan Pa BramantiNo ratings yet
- Nurse Education Today: Thomas Buckley, Christopher GordonDocument6 pagesNurse Education Today: Thomas Buckley, Christopher GordonagssugaNo ratings yet
- Information Technology System Applicable in Nursing PracticeDocument9 pagesInformation Technology System Applicable in Nursing PracticeZyrene Rivera100% (3)
- 1 s2.0 S0165178119306833 MainDocument7 pages1 s2.0 S0165178119306833 MainHindi ako goodsNo ratings yet
- CladsDocument7 pagesCladsParvathy R NairNo ratings yet
- Predicción Longitudinal de La Aptitud Cardiorrespiratoria A Través de Dispositivos Portátiles en Entornos de Vida LibreDocument11 pagesPredicción Longitudinal de La Aptitud Cardiorrespiratoria A Través de Dispositivos Portátiles en Entornos de Vida Libremariojosehurtado3955No ratings yet
- LeeYih SIM 2010Document17 pagesLeeYih SIM 2010Mohamed MuradNo ratings yet
- #PENTING Demeurechy2018Document19 pages#PENTING Demeurechy2018Octapaedi SoetomoNo ratings yet
- 2008 Evolution of Mechanical Ventilation in Response ToDocument8 pages2008 Evolution of Mechanical Ventilation in Response Tonanang criztaNo ratings yet
- 2014 Tinga PHMEuropeDocument11 pages2014 Tinga PHMEuropejudarangocaNo ratings yet
- Whatistherolepfphysioin PICUDocument7 pagesWhatistherolepfphysioin PICUsundar_kumar0No ratings yet
- 1 s2.0 S2468294221000605 MainDocument7 pages1 s2.0 S2468294221000605 MainVishal BasuNo ratings yet
- Estrategias VentilatoriasDocument8 pagesEstrategias VentilatoriasJose ManuelNo ratings yet
- Critical Care ApplicationDocument36 pagesCritical Care ApplicationMonique ReyesNo ratings yet
- 1543-2165 (2006) 130 (1263 Appasn) 2 0 Co 2Document6 pages1543-2165 (2006) 130 (1263 Appasn) 2 0 Co 2jhidalgomdNo ratings yet
- Thrall 2014Document5 pagesThrall 2014Rudi IlhamsyahNo ratings yet
- Miller Et Al. (In Press) - Experimental and Quasi-Experimental Designs in Implementation ResearchDocument7 pagesMiller Et Al. (In Press) - Experimental and Quasi-Experimental Designs in Implementation ResearchThiagoNo ratings yet
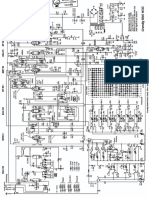
- Elisee - 150 Service ManualDocument176 pagesElisee - 150 Service ManualDawoodNo ratings yet
- Romse Design Switch Mode Power Supply RmoseDocument29 pagesRomse Design Switch Mode Power Supply RmoseDawoodNo ratings yet
- أجهزة التحاليل الطبية واستخداماتهاDocument22 pagesأجهزة التحاليل الطبية واستخداماتهاDawoodNo ratings yet
- Equ24-02 Chem Intergra400plus Op-SOPDocument12 pagesEqu24-02 Chem Intergra400plus Op-SOPDawoodNo ratings yet
- PDF Scanner 19-05-22 5.41.11Document6 pagesPDF Scanner 19-05-22 5.41.11DawoodNo ratings yet
- 18 5 2022Document18 pages18 5 2022DawoodNo ratings yet
- Grundig 5040w-3dDocument7 pagesGrundig 5040w-3dDawoodNo ratings yet
- IHDS 2021-2022 Trimester 3 BrochureDocument37 pagesIHDS 2021-2022 Trimester 3 BrochureDawoodNo ratings yet
- Frequency of Parts Replacement On All Analyzers-1Document3 pagesFrequency of Parts Replacement On All Analyzers-1DawoodNo ratings yet
- PDF Scanner 18-05-22 6.11.16Document4 pagesPDF Scanner 18-05-22 6.11.16DawoodNo ratings yet
- Mythic 60: Service ManualDocument255 pagesMythic 60: Service ManualDawoodNo ratings yet
- Mythic 60: User's ManualDocument122 pagesMythic 60: User's ManualDawoodNo ratings yet
- Volume-Targeted Modes of Modern Neonatal Ventilators: How Stable Is The Delivered Tidal Volume?Document10 pagesVolume-Targeted Modes of Modern Neonatal Ventilators: How Stable Is The Delivered Tidal Volume?DawoodNo ratings yet
- Capnografo Capnocheck PlusDocument2 pagesCapnografo Capnocheck Pluspaola100% (1)
- AAST PSG Guideline FinalDocument21 pagesAAST PSG Guideline FinalNana CastilloNo ratings yet
- Inspiration - 7i - Ventilator EventDocument6 pagesInspiration - 7i - Ventilator EventLicitaciones InbiosNo ratings yet
- NZ Crisis Handbook - DiagnosingDocument16 pagesNZ Crisis Handbook - DiagnosingSean SmythNo ratings yet
- Emergency Care Algorithms 2022Document88 pagesEmergency Care Algorithms 2022Gustavo Paredes0% (1)
- Capnography in ICUDocument49 pagesCapnography in ICUherbertglennyNo ratings yet
- Slides Nursing Pulse Oximetry Capnography PDFDocument32 pagesSlides Nursing Pulse Oximetry Capnography PDFPablo Maria Peralta LorcaNo ratings yet
- ELEC4810: Introduction To Biosensors and Bioinstrumentation: Lecture Notes - Set #10Document17 pagesELEC4810: Introduction To Biosensors and Bioinstrumentation: Lecture Notes - Set #10Kwan ChanNo ratings yet
- User Manual: Vitalogik 4000 / 6000 Series®Document576 pagesUser Manual: Vitalogik 4000 / 6000 Series®SERGIO PEREZNo ratings yet
- Case Report - Ectopia CordisDocument10 pagesCase Report - Ectopia CordisAnne Reichel MinasNo ratings yet
- Masimo Emma Capnograph User ManualDocument34 pagesMasimo Emma Capnograph User ManualChristian MuñozNo ratings yet
- SLE6000 English InteractiveDocument8 pagesSLE6000 English InteractiveWaseem MurtazaNo ratings yet
- Paramedic NREMTDocument88 pagesParamedic NREMTJadie Barringer III100% (2)
- ALS AlgorithmDocument22 pagesALS AlgorithmBookwormNo ratings yet
- ECRI Monitor Multiparametro 2012Document15 pagesECRI Monitor Multiparametro 2012Direccion TecnicaNo ratings yet
- Fleximag - 110xxxx-Ne-22-01 Instruction and Service ManualDocument135 pagesFleximag - 110xxxx-Ne-22-01 Instruction and Service ManualWalter Perdomo50% (2)
- Ventilador Mekics PDFDocument4 pagesVentilador Mekics PDFBalam CaballeroNo ratings yet
- 271 High Frequency Jet VentilationDocument10 pages271 High Frequency Jet VentilationachyutsharmaNo ratings yet
- Assessment of Knowledge About Vital Signs Among Paramedical StudentsDocument7 pagesAssessment of Knowledge About Vital Signs Among Paramedical StudentsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Extubation - Making Safer PDFDocument6 pagesExtubation - Making Safer PDFUlises Herrera SotoNo ratings yet
- M880 User ManualDocument103 pagesM880 User ManualMateuszNo ratings yet
- Cardiac SurgeryDocument25 pagesCardiac SurgeryMohamed HamdyNo ratings yet
- Enls V 4 0 Protocol Avs FinalDocument14 pagesEnls V 4 0 Protocol Avs Finalsucipto suciptoNo ratings yet
- Zeus Ie Sw2n Ifu 9054908 enDocument460 pagesZeus Ie Sw2n Ifu 9054908 enRazwan ErtepNo ratings yet
- 2021 ACLS Study GuideDocument20 pages2021 ACLS Study GuideShane Brown83% (12)
- CapnografiaDocument19 pagesCapnografiaJunior BarbozaNo ratings yet
- AHA ACLS Megacode ScenariosDocument6 pagesAHA ACLS Megacode ScenariosVitor Hugo G Correia86% (7)
- 54730546Document164 pages54730546Paul Gomez GarcíaNo ratings yet
- Elisa 300 - 800Document40 pagesElisa 300 - 800junaid ahmadNo ratings yet
- Mechanical Ventilator: Design and Implementation: Professor Yasser Mostafa KadahDocument19 pagesMechanical Ventilator: Design and Implementation: Professor Yasser Mostafa Kadahmorton1472No ratings yet