You might also like
- NURSING ADMINISTRATION: Passbooks Study GuideFrom EverandNURSING ADMINISTRATION: Passbooks Study GuideNo ratings yet
- Utilization Review Coordinator: Passbooks Study GuideFrom EverandUtilization Review Coordinator: Passbooks Study GuideNo ratings yet
- Health Record Technician I: Passbooks Study GuideFrom EverandHealth Record Technician I: Passbooks Study GuideNo ratings yet
- Supervising Registered Nurse: Passbooks Study GuideFrom EverandSupervising Registered Nurse: Passbooks Study GuideNo ratings yet
- NURSING ADMINISTRATION, ADVANCED: Passbooks Study GuideFrom EverandNURSING ADMINISTRATION, ADVANCED: Passbooks Study GuideNo ratings yet
- Healthcare Environmental Services A Complete Guide - 2020 EditionFrom EverandHealthcare Environmental Services A Complete Guide - 2020 EditionNo ratings yet
- Textbook of Urgent Care Management: Chapter 24, Revenue Cycle Management and PartnershipFrom EverandTextbook of Urgent Care Management: Chapter 24, Revenue Cycle Management and PartnershipNo ratings yet
- Textbook of Urgent Care Management: Chapter 34, Engaging Accountable Care Organizations in Urgent Care CentersFrom EverandTextbook of Urgent Care Management: Chapter 34, Engaging Accountable Care Organizations in Urgent Care CentersNo ratings yet
- The New Era of Regulatory Enforcement: A Comprehensive Guide for Raising the Bar to Manage RiskFrom EverandThe New Era of Regulatory Enforcement: A Comprehensive Guide for Raising the Bar to Manage RiskNo ratings yet
- Hospitalist Program Toolkit: A Comprehensive Guide to Implementation of Successful Hospitalist ProgramsFrom EverandHospitalist Program Toolkit: A Comprehensive Guide to Implementation of Successful Hospitalist ProgramsNo ratings yet
- Clerical Positions (Entry Level): Passbooks Study GuideFrom EverandClerical Positions (Entry Level): Passbooks Study GuideNo ratings yet
- The Healthcare Law and Ethics: Principles & PracticesFrom EverandThe Healthcare Law and Ethics: Principles & PracticesNo ratings yet
- Your Healthcare Job Hunt: How Your Digital Presence Can Make or Break Your CareerFrom EverandYour Healthcare Job Hunt: How Your Digital Presence Can Make or Break Your CareerNo ratings yet
- Textbook of Urgent Care Management: Chapter 32, Implementation of a Moderate-Complexity Clinical LaboratoryFrom EverandTextbook of Urgent Care Management: Chapter 32, Implementation of a Moderate-Complexity Clinical LaboratoryNo ratings yet
- Certified Professional in Medical Services Management: Passbooks Study GuideFrom EverandCertified Professional in Medical Services Management: Passbooks Study GuideNo ratings yet
- Employment Consultant (Testing): Passbooks Study GuideFrom EverandEmployment Consultant (Testing): Passbooks Study GuideNo ratings yet
- A few minutes to improve Risk documentation Accuracy even when you know nothing about Medicare Risk AdjustmentFrom EverandA few minutes to improve Risk documentation Accuracy even when you know nothing about Medicare Risk AdjustmentNo ratings yet
- Health policy Administration The Ultimate Step-By-Step GuideFrom EverandHealth policy Administration The Ultimate Step-By-Step GuideNo ratings yet
- Disability Insurance Program Representative: Passbooks Study GuideFrom EverandDisability Insurance Program Representative: Passbooks Study GuideNo ratings yet
- Textbook of Urgent Care Management: Chapter 38, Audits by Managed-Care Organizations and Regulatory AgenciesFrom EverandTextbook of Urgent Care Management: Chapter 38, Audits by Managed-Care Organizations and Regulatory AgenciesNo ratings yet
- Health Program Manager: Passbooks Study GuideFrom EverandHealth Program Manager: Passbooks Study GuideNo ratings yet
- Health Information Technology A Complete Guide - 2020 EditionFrom EverandHealth Information Technology A Complete Guide - 2020 EditionNo ratings yet
- Hospital Administration Consultant: Passbooks Study GuideFrom EverandHospital Administration Consultant: Passbooks Study GuideNo ratings yet
- Textbook of Urgent Care Management: Chapter 33, EMTALA in Urgent Care MedicineFrom EverandTextbook of Urgent Care Management: Chapter 33, EMTALA in Urgent Care MedicineNo ratings yet
- Health Management Information System A Complete Guide - 2020 EditionFrom EverandHealth Management Information System A Complete Guide - 2020 EditionNo ratings yet
- Textbook of Urgent Care Management: Chapter 12, Pro Forma Financial StatementsFrom EverandTextbook of Urgent Care Management: Chapter 12, Pro Forma Financial StatementsNo ratings yet
- Medicaid Claims Examiner: Passbooks Study GuideFrom EverandMedicaid Claims Examiner: Passbooks Study GuideNo ratings yet
- ARRT EXAMINATION IN CARDIOVASCULAR-INTERVENTIONAL TECHNOLOGY (CIT): Passbooks Study GuideFrom EverandARRT EXAMINATION IN CARDIOVASCULAR-INTERVENTIONAL TECHNOLOGY (CIT): Passbooks Study GuideNo ratings yet
- Public Health Assistant: Passbooks Study GuideFrom EverandPublic Health Assistant: Passbooks Study GuideNo ratings yet
- Office Assistant II (Calculations): Passbooks Study GuideFrom EverandOffice Assistant II (Calculations): Passbooks Study GuideNo ratings yet
- NURSING THE CHILDBEARING FAMILY: Passbooks Study GuideFrom EverandNURSING THE CHILDBEARING FAMILY: Passbooks Study GuideNo ratings yet
- BEHAVIORAL SCIENCES FOR NURSES: Passbooks Study GuideFrom EverandBEHAVIORAL SCIENCES FOR NURSES: Passbooks Study GuideRating: 1 out of 5 stars1/5 (1)
- Take As Directed: Your Prescription for Safe Health Care in CanadaFrom EverandTake As Directed: Your Prescription for Safe Health Care in CanadaRating: 3.5 out of 5 stars3.5/5 (14)
- Office Assistant II (Customer Service): Passbooks Study GuideFrom EverandOffice Assistant II (Customer Service): Passbooks Study GuideNo ratings yet
- Medical Record Administrator: Passbooks Study GuideFrom EverandMedical Record Administrator: Passbooks Study GuideNo ratings yet
- Medical equipment management Complete Self-Assessment GuideFrom EverandMedical equipment management Complete Self-Assessment GuideNo ratings yet
- Electronic Health Records: An Audit and Internal Control GuideFrom EverandElectronic Health Records: An Audit and Internal Control GuideNo ratings yet
- Risk Management Handbook for Health Care Organizations, 3 Volume SetFrom EverandRisk Management Handbook for Health Care Organizations, 3 Volume SetNo ratings yet
- IEHP Medi-Cal Members Rights and Responsibilities PDFDocument11 pagesIEHP Medi-Cal Members Rights and Responsibilities PDFminipower50No ratings yet
- ACHC - Standards - Community RetailDocument71 pagesACHC - Standards - Community RetailServesh Tiwari100% (2)
- Feb 2022 Compliance ReportDocument62 pagesFeb 2022 Compliance ReportThe TexanNo ratings yet
- Ahima Data Quality Management ModelDocument11 pagesAhima Data Quality Management Modelselinasimpson2301No ratings yet
- Chapter DHS 83: Community Based Residential FacilitiesDocument26 pagesChapter DHS 83: Community Based Residential FacilitiesAmberNo ratings yet
- Extension Rural Fellows Q4 NewsletterDocument1 pageExtension Rural Fellows Q4 NewsletterNTV NewsNo ratings yet
- Dave Ptak Employment AgreementDocument4 pagesDave Ptak Employment AgreementNTV NewsNo ratings yet
- Letter To Candidate Herbster Re Use of MarksDocument2 pagesLetter To Candidate Herbster Re Use of MarksNTV NewsNo ratings yet
- Grand Island Northwest Letter To ParentsDocument2 pagesGrand Island Northwest Letter To ParentsNTV NewsNo ratings yet
- Letter From Speaker Hilgers On Special SessionDocument2 pagesLetter From Speaker Hilgers On Special SessionNTV NewsNo ratings yet
- Dave Ptak Resignation LetterDocument1 pageDave Ptak Resignation LetterNTV NewsNo ratings yet
- Herbster v. Slama ComplaintDocument9 pagesHerbster v. Slama ComplaintNTV NewsNo ratings yet
- Fiji ComplaintDocument30 pagesFiji ComplaintNTV NewsNo ratings yet
- Nebraska Extension Ag FlyersDocument2 pagesNebraska Extension Ag FlyersNTV NewsNo ratings yet
- Spilker LPD LawsuitDocument34 pagesSpilker LPD LawsuitNTV NewsNo ratings yet
- GIPS Safe Return To School 21-22 FINALDocument11 pagesGIPS Safe Return To School 21-22 FINALNTV NewsNo ratings yet
- Nebraska Extension 2022 Winter ProgramDocument2 pagesNebraska Extension 2022 Winter ProgramNTV NewsNo ratings yet
- Letter To Candidate Herbster Re Use of MarksDocument2 pagesLetter To Candidate Herbster Re Use of MarksNTV NewsNo ratings yet
- Letter To Candidate Pillen Re Use of University MarksDocument2 pagesLetter To Candidate Pillen Re Use of University MarksNTV NewsNo ratings yet
- Operations and Vendor Analysis Report Prepared by Jeremy JensenDocument11 pagesOperations and Vendor Analysis Report Prepared by Jeremy JensenNTV News100% (1)
- Petition Against GIPSDocument5 pagesPetition Against GIPSNTV NewsNo ratings yet
- NRCSA Considerations For Re-OpeningDocument31 pagesNRCSA Considerations For Re-OpeningNTV NewsNo ratings yet
- 2020.01.22 - ComplaintDocument79 pages2020.01.22 - ComplaintNTV NewsNo ratings yet
- UNK Summer Graduate ListDocument4 pagesUNK Summer Graduate ListNTV NewsNo ratings yet
- NE Attorney General Complaint Against Mead Ethanol PlantDocument113 pagesNE Attorney General Complaint Against Mead Ethanol PlantNTV NewsNo ratings yet
- Grandparents Day Reg. Form 2019Document1 pageGrandparents Day Reg. Form 2019NTV NewsNo ratings yet
- Robocall LetterDocument6 pagesRobocall LetterNTV NewsNo ratings yet
- Radon Test Results - NTV NewsDocument2 pagesRadon Test Results - NTV NewsNTV NewsNo ratings yet
- Joseph Williams AffidavitDocument3 pagesJoseph Williams AffidavitNTV NewsNo ratings yet
- John Kakkuzhiyil New DatesDocument3 pagesJohn Kakkuzhiyil New DatesNTV NewsNo ratings yet
- Seward County Sample BallotDocument1 pageSeward County Sample BallotNTV NewsNo ratings yet
- NEB RVP Written Comments 4.29.19Document4 pagesNEB RVP Written Comments 4.29.19NTV NewsNo ratings yet
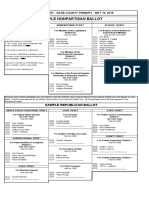
- Gage County Sample BallotDocument3 pagesGage County Sample BallotNTV NewsNo ratings yet
- Lancaster County Sample BallotDocument3 pagesLancaster County Sample BallotNTV NewsNo ratings yet
- Routine Immunization Schedule ToolDocument2 pagesRoutine Immunization Schedule ToolJack MillerNo ratings yet
- Boalan Es Health Condition 2023 FinalDocument2 pagesBoalan Es Health Condition 2023 FinalMely DelacruzNo ratings yet
- Antifungal DrugsDocument12 pagesAntifungal Drugsshibsankar rakshitNo ratings yet
- BDS FINAL YEAR PERIODONTICS CHAPTERSDocument7 pagesBDS FINAL YEAR PERIODONTICS CHAPTERSakash_81087No ratings yet
- DNA Flow Technology - 2016Document2 pagesDNA Flow Technology - 2016Uswatun hasanah harifuddinNo ratings yet
- Bacterial Infection On Upper Respiratory Tract Hemofillus Moraxella Fusobacterium Ed 1Document29 pagesBacterial Infection On Upper Respiratory Tract Hemofillus Moraxella Fusobacterium Ed 1Cintya Risti MawarniNo ratings yet
- Arboviruses in ChinaDocument21 pagesArboviruses in ChinaChris LicínioNo ratings yet
- Viral Infection AHEADDocument24 pagesViral Infection AHEADShiena Mae PelagioNo ratings yet
- Chikungunya Virus Disease: Ii. Clinical InformationDocument2 pagesChikungunya Virus Disease: Ii. Clinical Informationkbl27No ratings yet
- Eosinophils in The GI TractDocument15 pagesEosinophils in The GI TractdkbritobNo ratings yet
- Montelukast in Hospitalized Patients Diagnosed With COVID 19-1Document8 pagesMontelukast in Hospitalized Patients Diagnosed With COVID 19-1Golam JILANI Mahbubay AlamNo ratings yet
- Infeksi NosokomialDocument29 pagesInfeksi NosokomialAlunaficha Melody KiraniaNo ratings yet
- Hepatitis B in Pregnancy: Global Importance and Need for ControlDocument42 pagesHepatitis B in Pregnancy: Global Importance and Need for ControlAbraham ChiuNo ratings yet
- Eur J Immunol - 2020 - Hanitsch - Treatment and Management of Primary Antibody Deficiency German InterdisciplinaryDocument15 pagesEur J Immunol - 2020 - Hanitsch - Treatment and Management of Primary Antibody Deficiency German InterdisciplinaryRSU Trijaya medical centerNo ratings yet
- Final Presentation (Stock Pitch) - ModernaDocument8 pagesFinal Presentation (Stock Pitch) - ModernaAarushiNo ratings yet
- Monoclonal AntibodiesDocument13 pagesMonoclonal AntibodiesEllen Mynelle MabulacNo ratings yet
- List of PubMed Central Journals Open AccessDocument6 pagesList of PubMed Central Journals Open AccessAhmad Sayeed KhanNo ratings yet
- A Positive Serum Basophil Histamine Release AssayDocument4 pagesA Positive Serum Basophil Histamine Release AssayBrîndușa PetruțescuNo ratings yet
- Penicillin G (Intravenous and Short-Acting Intramuscular) - Drug Information - UpToDateDocument29 pagesPenicillin G (Intravenous and Short-Acting Intramuscular) - Drug Information - UpToDateMikaela lNo ratings yet
- Communicable Disease Nursing: Hosts, Microbes and ImmunityDocument421 pagesCommunicable Disease Nursing: Hosts, Microbes and ImmunityJoric Magusara91% (11)
- Verified Market Research - Global Pseudomonas Aeruginosa Infection Treatment MarketDocument2 pagesVerified Market Research - Global Pseudomonas Aeruginosa Infection Treatment MarketTejas D HusukaleNo ratings yet
- Obat Antijamur: Wening Sari, DR., M.KesDocument18 pagesObat Antijamur: Wening Sari, DR., M.KesdebbyelviraNo ratings yet
- Bajwa, 2018 - Atopic Dermatitis in CatsDocument3 pagesBajwa, 2018 - Atopic Dermatitis in CatsFabricio CamargoNo ratings yet
- PROTOZOA DARAH (MALARIADocument88 pagesPROTOZOA DARAH (MALARIAGladis Aprilla RizkiNo ratings yet
- Day 1 PNUDocument250 pagesDay 1 PNUM LNo ratings yet
- The Journal of Dermatology - 2022 - Sakamoto - T Cell Rich Perivascular Inflammation in A Case of Cutaneous VariantDocument2 pagesThe Journal of Dermatology - 2022 - Sakamoto - T Cell Rich Perivascular Inflammation in A Case of Cutaneous VariantKi IsoNo ratings yet
- Case 1 Pedia Henoch Schonlein PurpuraDocument45 pagesCase 1 Pedia Henoch Schonlein PurpuraJefferson Gumiran100% (1)
- Churg StraussDocument15 pagesChurg StraussMiguel AguileraNo ratings yet
- T Cell Flyer PDFDocument26 pagesT Cell Flyer PDFJohnny AtmanNo ratings yet
- Pupil Personal Data FormDocument12 pagesPupil Personal Data FormKyleZack Rivera100% (1)