You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5811)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Personal Statement - University of EssexDocument2 pagesPersonal Statement - University of EssexAsare WilliamsNo ratings yet
- Maslowski2001 - School Culture and School PerformanceDocument220 pagesMaslowski2001 - School Culture and School PerformanceAlice ChenNo ratings yet
- How ComeDocument24 pagesHow ComeGreenNo ratings yet
- Caring Science Education: Measuring Nurses' Caring BehaviorsDocument13 pagesCaring Science Education: Measuring Nurses' Caring BehaviorsKresensia Anne GetriniNo ratings yet
- Apas 2022 African Religion-1Document200 pagesApas 2022 African Religion-1Ibrahim Lawal AhmedNo ratings yet
- Process Tracing and ComparisonDocument17 pagesProcess Tracing and ComparisonSalmanNo ratings yet
- ParadigmsDocument6 pagesParadigmsReshma GeorgiNo ratings yet
- 2 Hpef 7053Document5 pages2 Hpef 7053Jefri HussinNo ratings yet
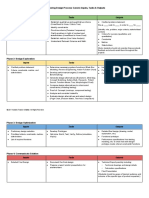
- Engineering Design Process: Generic Inputs, Tasks & Outputs Phase 1: Problem DefinitionDocument2 pagesEngineering Design Process: Generic Inputs, Tasks & Outputs Phase 1: Problem DefinitionAhmad Rifky AzisNo ratings yet
- Sserunjogi Nicholus. Peoples Knowledge About Fire InsuranceDocument42 pagesSserunjogi Nicholus. Peoples Knowledge About Fire InsuranceSSERUNJOGI NICHOLUSNo ratings yet
- Test With AnswersDocument3 pagesTest With AnswersKarla Bernadette HonradoNo ratings yet
- CG ResearchDocument16 pagesCG ResearchArman VillagraciaNo ratings yet
- Unisdrmeframeworkver1.0Document26 pagesUnisdrmeframeworkver1.0Joeban R. Paza100% (1)
- Critique Paper GuideDocument2 pagesCritique Paper GuideFerreras Dexter Arandela100% (1)
- Introduksyon Sa Pag Aaral NG WikaDocument11 pagesIntroduksyon Sa Pag Aaral NG WikaNellyNo ratings yet
- Ugyen-ODL-Quantitative Techniques in Management - AssignmentA-Question 1Document6 pagesUgyen-ODL-Quantitative Techniques in Management - AssignmentA-Question 1Ugyen LingpaNo ratings yet
- Blended Learning FrameworkDocument9 pagesBlended Learning FrameworkDion Aris Simanjuntak (dionjuntak)No ratings yet
- Qualitative Research Proposal Finalised VersionDocument20 pagesQualitative Research Proposal Finalised VersionMohd AzwanNo ratings yet
- Jquilca,+1 +the+use+of+massive+online+games+in+game-Based+learning+activitiesDocument24 pagesJquilca,+1 +the+use+of+massive+online+games+in+game-Based+learning+activitiesBombe ZombeNo ratings yet
- The Effects of Online Game A Study On Online Game Addiction Among UNISEL S Shah Alam Campus StudentsDocument85 pagesThe Effects of Online Game A Study On Online Game Addiction Among UNISEL S Shah Alam Campus StudentsVanna Louise DuhaylungsodNo ratings yet
- RM&IPR Notes - Unit 1Document24 pagesRM&IPR Notes - Unit 1Sai PrasadNo ratings yet
- Final Draft Research Paper Ritika KhatiDocument41 pagesFinal Draft Research Paper Ritika Khatibishnu paudelNo ratings yet
- I. Objectives: A. Content Standards: B. Performance Standards: C. Learning CompetenciesDocument4 pagesI. Objectives: A. Content Standards: B. Performance Standards: C. Learning CompetenciesTJ SabadoNo ratings yet
- Dissertation With Only Secondary DataDocument8 pagesDissertation With Only Secondary DataCheapPaperWritingServiceSingapore100% (1)
- Assessing ChangeDocument65 pagesAssessing ChangeNCVONo ratings yet
- Lived Experiences of Flood in Riverine CommunitiesDocument33 pagesLived Experiences of Flood in Riverine CommunitiesHAIDEE VASQUEZNo ratings yet
- 1639 GCS210462 NguyenQuangHuyASM1 BriefDocument19 pages1639 GCS210462 NguyenQuangHuyASM1 BriefLão Rùa OfficialNo ratings yet
- Kinerja Pelayanan Dinas Kependudukan Dan Pencatatan Sipil Kepada MasyarakatDocument9 pagesKinerja Pelayanan Dinas Kependudukan Dan Pencatatan Sipil Kepada MasyarakatJirou KazugamiNo ratings yet
- PolicingDocument44 pagesPolicingbcapstone100% (1)
- Research QuestionDocument7 pagesResearch Questionতৌহিদুল ইসলামNo ratings yet