You might also like
- Iron therapy - With Special Emphasis on Intravenous AdministrationFrom EverandIron therapy - With Special Emphasis on Intravenous AdministrationNo ratings yet
- Bonnie and Clyde: Vitamin C and Iron Are Partners in Crime in Iron Deficiency Anaemia and Its Potential Role in The ElderlyDocument3 pagesBonnie and Clyde: Vitamin C and Iron Are Partners in Crime in Iron Deficiency Anaemia and Its Potential Role in The ElderlyDina Ikrama PutriNo ratings yet
- The Role of Copper As A Modifier of Lipid Metabolism: January 2013Document23 pagesThe Role of Copper As A Modifier of Lipid Metabolism: January 2013Leni LismayantiNo ratings yet
- Hepcidin Knockout Mice Fed With Iron Rich DietDocument9 pagesHepcidin Knockout Mice Fed With Iron Rich DietEduardo Henrique de Sousa SalvinoNo ratings yet
- Iron Review 2014 ResMedScDocument12 pagesIron Review 2014 ResMedScgayatri sabaradNo ratings yet
- Intravenous Irons: From Basic Science To Clinical Practice: PharmaceuticalsDocument20 pagesIntravenous Irons: From Basic Science To Clinical Practice: Pharmaceuticalsisabel pangNo ratings yet
- A Novel Approach For Iron DeficiencyDocument15 pagesA Novel Approach For Iron DeficiencyMahyar MehrNo ratings yet
- Walters, Esfandi, Tsopmo - 2018 - Potential of Food Hydrolyzed Proteins and Peptides To Chelate Iron or Calcium and Enhance Their Absorp-AnnotatedDocument17 pagesWalters, Esfandi, Tsopmo - 2018 - Potential of Food Hydrolyzed Proteins and Peptides To Chelate Iron or Calcium and Enhance Their Absorp-AnnotatedDiễm SươngNo ratings yet
- Jurnal Anemia BesiDocument14 pagesJurnal Anemia BesiSonya MaysalvaNo ratings yet
- Nutrients 10 01647 PDFDocument11 pagesNutrients 10 01647 PDFNaeem AnjumNo ratings yet
- Peptide-Mineral Complexes Understanding TheirDocument17 pagesPeptide-Mineral Complexes Understanding TheirDiễm SươngNo ratings yet
- Deferasirox-An Oral Agent For Chronic Iron Overload: New Drug DevelopmentsDocument8 pagesDeferasirox-An Oral Agent For Chronic Iron Overload: New Drug DevelopmentsTriska Maharani Manoppo100% (1)
- Iron SucroseDocument14 pagesIron SucroseTejaswi J DamerlaNo ratings yet
- Iron Biology, Immunology, Aging, and Obesity: Four Fields Connected by The Small Peptide Hormone HepcidinDocument16 pagesIron Biology, Immunology, Aging, and Obesity: Four Fields Connected by The Small Peptide Hormone HepcidinSagita DarmasariNo ratings yet
- Balance de HierroDocument13 pagesBalance de HierroWalter Huacani HuamaniNo ratings yet
- IDA and ChildDocument15 pagesIDA and ChildSarah KemalasariNo ratings yet
- Diagnosis and Management of Iron Deficiency Anemia in The 21st CenturyDocument8 pagesDiagnosis and Management of Iron Deficiency Anemia in The 21st CenturyireneNo ratings yet
- TranslateDocument68 pagesTranslateNando WatungNo ratings yet
- Role of Iron in Human BodyDocument6 pagesRole of Iron in Human BodyAliza KhanNo ratings yet
- 8 PDFDocument8 pages8 PDFSofia FurtadoNo ratings yet
- Iron's Importance for Human HealthDocument11 pagesIron's Importance for Human HealthSegun TalabiNo ratings yet
- Electrons Redox Scavenging Free Radicals (1) (2) : CopperDocument9 pagesElectrons Redox Scavenging Free Radicals (1) (2) : CopperTowhid HasanNo ratings yet
- 11 Vol. 12 Issue 5 May 2021 IJPSR RA 14622Document13 pages11 Vol. 12 Issue 5 May 2021 IJPSR RA 14622VinayNo ratings yet
- Heavy Metal in The Intensive Care Unit: A Review of Current Literature On Trace Element Supplementation in Critically Ill PatientsDocument12 pagesHeavy Metal in The Intensive Care Unit: A Review of Current Literature On Trace Element Supplementation in Critically Ill PatientsSaaluddin ArsyadNo ratings yet
- Article 1659164610Document14 pagesArticle 1659164610B49 Nabila Araishabeby YudyatirtaNo ratings yet
- Management of Iron de Ficiency: Shuoyan Ning and Michelle P. ZellerDocument8 pagesManagement of Iron de Ficiency: Shuoyan Ning and Michelle P. ZellerGeorgina Aguilar GallardoNo ratings yet
- Liposomal IronDocument6 pagesLiposomal IronPiyush KhetrapalNo ratings yet
- Div Styletext-Align Justify Copper - An Essential Micronutrient For Calves and Adult Cattle DivDocument10 pagesDiv Styletext-Align Justify Copper - An Essential Micronutrient For Calves and Adult Cattle DivNesibe TaşdemirNo ratings yet
- Peerj 10 13592Document19 pagesPeerj 10 13592yvettejongenNo ratings yet
- Copper Deficiency Anemia: Review ArticleDocument8 pagesCopper Deficiency Anemia: Review ArticleIlham RamadhanNo ratings yet
- Mechanisms of Iron Loading and Toxicity: Gregory J. AndersonDocument4 pagesMechanisms of Iron Loading and Toxicity: Gregory J. Andersonikhsan07No ratings yet
- 2021 Iron Replacement Therapy in Heart Failure A Literature ReviewDocument11 pages2021 Iron Replacement Therapy in Heart Failure A Literature ReviewSiswanto H. AzwarNo ratings yet
- Anemia in IndiaDocument13 pagesAnemia in IndiaAle ZevallosNo ratings yet
- Iron in FoodDocument22 pagesIron in FoodMarshal GrahamNo ratings yet
- Efficacy of A Novel Food Supplement (Ferfer®) Containing Microencapsulated Iron in Liposomal Form in Female Iron Deficiency AnemiaDocument7 pagesEfficacy of A Novel Food Supplement (Ferfer®) Containing Microencapsulated Iron in Liposomal Form in Female Iron Deficiency AnemiaAnnisa magfiraNo ratings yet
- Hepcidin's Role in Iron Distribution and Anemia of Chronic Kidney DiseaseDocument7 pagesHepcidin's Role in Iron Distribution and Anemia of Chronic Kidney DiseasegigibesiNo ratings yet
- 03 Iron Transport Proteins Gateways of Cellular and SystemicDocument9 pages03 Iron Transport Proteins Gateways of Cellular and SystemicMatheus SouzaNo ratings yet
- IronDocument22 pagesIronJoiceLanaNo ratings yet
- Iron Absorption and Strategies to Control Iron Deficiency AnaemiaDocument7 pagesIron Absorption and Strategies to Control Iron Deficiency Anaemiaகௌசிக் வெNo ratings yet
- Resumen Artículo InglésDocument2 pagesResumen Artículo InglésDaniela Orozco MartinezNo ratings yet
- Níveis de FerroDocument13 pagesNíveis de FerroCarla FernandaNo ratings yet
- Review Article: Iron-Deficiency Anemia: Indonesia's StrivingDocument14 pagesReview Article: Iron-Deficiency Anemia: Indonesia's StrivingmeldaoktaviaNo ratings yet
- Risk Factor VERY IMPODocument7 pagesRisk Factor VERY IMPOayham luNo ratings yet
- Am J Clin Nutr 1998 Whittaker 442S 6SDocument5 pagesAm J Clin Nutr 1998 Whittaker 442S 6SRegina ErikaNo ratings yet
- An exclusionary approach to recover Iron deficiency by POLYROLDocument6 pagesAn exclusionary approach to recover Iron deficiency by POLYROLKorry Meliana PangaribuanNo ratings yet
- Mantadakis-2015-Pediatric Blood CancerDocument7 pagesMantadakis-2015-Pediatric Blood CancerakshayajainaNo ratings yet
- Jurnal Maya 1Document16 pagesJurnal Maya 1Azwad AnHty AsHty SlamanyaNo ratings yet
- 1 - Iron Content, Bioavailability & Factors Affecting Iron Status of IndiansDocument12 pages1 - Iron Content, Bioavailability & Factors Affecting Iron Status of IndiansDivyesh AmarsedaNo ratings yet
- Characterizing pH-Dependent Release Kinetics of Iron MicrocapsulesDocument12 pagesCharacterizing pH-Dependent Release Kinetics of Iron MicrocapsulesLimber Castro ChinoNo ratings yet
- Intravenous Iron Use in The Care of Patients With Kidney DiseaseDocument3 pagesIntravenous Iron Use in The Care of Patients With Kidney DiseaseAntika CahyatiNo ratings yet
- BSR 37 bsr20170195Document7 pagesBSR 37 bsr20170195Carp TheodorNo ratings yet
- HHS Public Access: Developmental Physiology of Iron Absorption, Homeostasis and Metabolism in The Healthy Term InfantDocument13 pagesHHS Public Access: Developmental Physiology of Iron Absorption, Homeostasis and Metabolism in The Healthy Term InfantubafisioNo ratings yet
- EXCERPTED FROM: Vitamin and Mineral Safety 3Document11 pagesEXCERPTED FROM: Vitamin and Mineral Safety 3NitinPrachiJainNo ratings yet
- TRACE MineralsDocument18 pagesTRACE MineralsKipchirchir AbednegoNo ratings yet
- Iron Metabolism and Its DisordersDocument10 pagesIron Metabolism and Its DisordersMario AbdiwijoyoNo ratings yet
- 4147610translate PDFDocument10 pages4147610translate PDFNando WatungNo ratings yet
- Metabolisme IronDocument15 pagesMetabolisme IronERNI FORWATYNo ratings yet
- Caro Tenuto 2019Document8 pagesCaro Tenuto 2019Melahat UnalNo ratings yet
- Diagnosis and Management of Iron Deficiency Anemia in The 21st CenturyDocument8 pagesDiagnosis and Management of Iron Deficiency Anemia in The 21st CenturyNur AlamNo ratings yet
- Plant Ferritin-A Source of Iron To Prevent Its DeficiencyDocument18 pagesPlant Ferritin-A Source of Iron To Prevent Its DeficiencyLara Ayu LestariNo ratings yet
- BJD 17896Document8 pagesBJD 17896JeromeNo ratings yet
- Journal of Nutritional Science: Review Article Appropriate and Inappropriate Vitamin Supplementation in ChildrenDocument8 pagesJournal of Nutritional Science: Review Article Appropriate and Inappropriate Vitamin Supplementation in ChildrenNazihan Safitri AlkatiriNo ratings yet
- Anak Chairuddin9Document44 pagesAnak Chairuddin9Nazihan Safitri AlkatiriNo ratings yet
- Mihai 2018Document17 pagesMihai 2018Nazihan AlkatiriNo ratings yet
- Baru 5Document4 pagesBaru 5Nazihan Safitri AlkatiriNo ratings yet
- Baru 6Document6 pagesBaru 6Nazihan Safitri AlkatiriNo ratings yet
- Baru 1Document6 pagesBaru 1Nazihan Safitri AlkatiriNo ratings yet
- Baru 3Document8 pagesBaru 3Nazihan Safitri AlkatiriNo ratings yet
- Ijohns - 2018070416075309Document12 pagesIjohns - 2018070416075309Mega PuspitaNo ratings yet
- Hamilton Anxiety Rating Scale (HAM-A)Document2 pagesHamilton Anxiety Rating Scale (HAM-A)Elsa Ameliana ManurungNo ratings yet
- BJD 17896Document8 pagesBJD 17896JeromeNo ratings yet
- Baru 5Document4 pagesBaru 5Nazihan Safitri AlkatiriNo ratings yet
- New 2Document9 pagesNew 2Nazihan Safitri AlkatiriNo ratings yet
- Baru 2Document8 pagesBaru 2Nazihan Safitri AlkatiriNo ratings yet
- Staphylococcus Aureus in Dermatology Outpatients With Special Emphasis On Community-Associated Methicillin-Resistant StrainsDocument10 pagesStaphylococcus Aureus in Dermatology Outpatients With Special Emphasis On Community-Associated Methicillin-Resistant StrainsNazihan Safitri AlkatiriNo ratings yet
- Simpson Angus ScaleDocument6 pagesSimpson Angus ScaleManish KumarNo ratings yet
- Switching and Stopping Antidepressants: Nicholas KeksDocument8 pagesSwitching and Stopping Antidepressants: Nicholas KeksRodrigoNo ratings yet
- Management - of - Patients - With - Disk - Displacement - WithDocument8 pagesManagement - of - Patients - With - Disk - Displacement - WithNazihan Safitri AlkatiriNo ratings yet
- Management - of - Patients - With - Disk - Displacement - WithDocument8 pagesManagement - of - Patients - With - Disk - Displacement - WithNazihan Safitri AlkatiriNo ratings yet
- New 1Document5 pagesNew 1Nazihan Safitri AlkatiriNo ratings yet
- Pathogenesis Coagulopathy COVID-19Document33 pagesPathogenesis Coagulopathy COVID-19benny christantoNo ratings yet
- Coas Anak: Scanned by CamscannerDocument1 pageCoas Anak: Scanned by CamscannerNazihan Safitri AlkatiriNo ratings yet
- Journal of Nutritional Science: Review Article Appropriate and Inappropriate Vitamin Supplementation in ChildrenDocument8 pagesJournal of Nutritional Science: Review Article Appropriate and Inappropriate Vitamin Supplementation in ChildrenNazihan Safitri AlkatiriNo ratings yet
- Olewinski 2016Document15 pagesOlewinski 2016Nazihan Safitri AlkatiriNo ratings yet
- Nutrients 09 00190Document18 pagesNutrients 09 00190Yosephine SantosoNo ratings yet
- Management - of - Patients - With - Disk - Displacement - WithDocument8 pagesManagement - of - Patients - With - Disk - Displacement - WithNazihan Safitri AlkatiriNo ratings yet
- Hamilton Anxiety Rating Scale (HAM-A)Document2 pagesHamilton Anxiety Rating Scale (HAM-A)Elsa Ameliana ManurungNo ratings yet
- CP Growth ChartDocument30 pagesCP Growth ChartJijie Azeera100% (1)
- Nutrients 09 00190Document18 pagesNutrients 09 00190Yosephine SantosoNo ratings yet
- Review: Dopaminergic Neurons and Brain Reward Pathways From Neurogenesis To Circuit AssemblyDocument11 pagesReview: Dopaminergic Neurons and Brain Reward Pathways From Neurogenesis To Circuit AssemblyNazihan Safitri AlkatiriNo ratings yet
- ResMed Case Study AnalysisDocument12 pagesResMed Case Study Analysis徐芊芊No ratings yet
- Lesson 1 Context CluesDocument33 pagesLesson 1 Context CluesRomnick BistayanNo ratings yet
- EasyGreen ManualDocument33 pagesEasyGreen ManualpitoupitouNo ratings yet
- Fabric Trademark and Brand Name IndexDocument15 pagesFabric Trademark and Brand Name Indexsukrat20No ratings yet
- Si Eft Mandate FormDocument1 pageSi Eft Mandate FormdSolarianNo ratings yet
- School RulesDocument2 pagesSchool RulesAI HUEYNo ratings yet
- Jumpin' Beans Cafe Near SchoolDocument4 pagesJumpin' Beans Cafe Near SchoolJhon Axl Heart RaferNo ratings yet
- Sponsor A Child With E-Tuition 2022Document19 pagesSponsor A Child With E-Tuition 2022nuur xiemaNo ratings yet
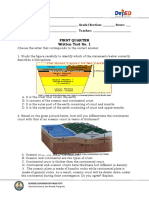
- Written Work 1 Q1 Science 10Document6 pagesWritten Work 1 Q1 Science 10JOEL MONTERDENo ratings yet
- Coleção Bernoulli Ensino Médio 2020 - 100% BNCC by Bernoulli Sistema de Ensino - IssuuDocument1 pageColeção Bernoulli Ensino Médio 2020 - 100% BNCC by Bernoulli Sistema de Ensino - IssuuVitor OliveiraNo ratings yet
- Villariba - Document Analysis - Jose RizalDocument2 pagesVillariba - Document Analysis - Jose RizalkrishaNo ratings yet
- In The Matter of The Adoption of Elizabeth MiraDocument2 pagesIn The Matter of The Adoption of Elizabeth MiradelayinggratificationNo ratings yet
- Warren BuffetDocument11 pagesWarren BuffetSopakirite Kuruye-AleleNo ratings yet
- Teresita Dio Versus STDocument2 pagesTeresita Dio Versus STmwaike100% (1)
- Parking Garage Design GuidelinesDocument17 pagesParking Garage Design GuidelinesCarlos Benjamin BCNo ratings yet
- Wiring Diagram Obp 1 v2Document5 pagesWiring Diagram Obp 1 v2Jorge Luis Vera AlmeidaNo ratings yet
- Postpaid Bill AugDocument2 pagesPostpaid Bill Augsiva vNo ratings yet
- Development Plan-Part IV, 2022-2023Document3 pagesDevelopment Plan-Part IV, 2022-2023Divina bentayao100% (5)
- Diagrama RSAG7.820.7977Document14 pagesDiagrama RSAG7.820.7977Manuel Medina100% (4)
- OUM Human Anatomy Final Exam QuestionsDocument5 pagesOUM Human Anatomy Final Exam QuestionsAnandNo ratings yet
- Types of Motivation in Language LearningDocument8 pagesTypes of Motivation in Language LearningAlya IrmasyahNo ratings yet
- Lesson 5 Classifications of CommunicationDocument48 pagesLesson 5 Classifications of CommunicationRovenick SinggaNo ratings yet
- SYLLABUS FYUP-PoliticalScience PDFDocument105 pagesSYLLABUS FYUP-PoliticalScience PDFIshta VohraNo ratings yet
- Surveying 2 Practical 3Document15 pagesSurveying 2 Practical 3Huzefa AliNo ratings yet
- Major Discoveries in Science HistoryDocument7 pagesMajor Discoveries in Science HistoryRoland AbelaNo ratings yet
- 09 Egyptian Architecture PDFDocument107 pages09 Egyptian Architecture PDFIra PecsonNo ratings yet
- Contrastive Study of English and Romanian Legal TerminologyDocument39 pagesContrastive Study of English and Romanian Legal TerminologyVictorNo ratings yet
- UITM Faculty of Business Entrepreneurship Rubric Social Media PortfolioDocument9 pagesUITM Faculty of Business Entrepreneurship Rubric Social Media PortfolioShamsyul AriffinNo ratings yet
- MSc Thesis on VAW in PhilippinesDocument100 pagesMSc Thesis on VAW in Philippineselma cutamoraNo ratings yet
- A Powerful Graphic Liquid Crystal Display: Column #47, March 1999 by Lon GlaznerDocument16 pagesA Powerful Graphic Liquid Crystal Display: Column #47, March 1999 by Lon GlaznerVijay P PulavarthiNo ratings yet