You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Jin Gui Yao Lue PDFDocument64 pagesJin Gui Yao Lue PDFSergio Jesús Huapaya Gálvez75% (4)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- MCU 2019 Human Diseases 5th EditionDocument626 pagesMCU 2019 Human Diseases 5th EditionMoon Edits100% (1)
- Pediatric Intensive Care Nursing Knowledge & Skills ChecklistDocument5 pagesPediatric Intensive Care Nursing Knowledge & Skills Checklistnorthweststaffing50% (2)
- BSIT 601 Activity 1 Moral DilemmasDocument2 pagesBSIT 601 Activity 1 Moral DilemmasJ-Lyn Seyer100% (5)
- Hawes 2003Document12 pagesHawes 2003Karibeños San JavierNo ratings yet
- Anti Bullying For Children PDF VersionDocument2 pagesAnti Bullying For Children PDF VersionMhelshy VillanuevaNo ratings yet
- BreakfastDocument1 pageBreakfastMhelshy VillanuevaNo ratings yet
- Peppercorn Mesisskkknnn6Document33 pagesPeppercorn Mesisskkknnn6Mhelshy VillanuevaNo ratings yet
- KS4 Physical Education: The Circulatory SystemDocument36 pagesKS4 Physical Education: The Circulatory SystemAjay Pal NattNo ratings yet
- BreakfastDocument1 pageBreakfastMhelshy VillanuevaNo ratings yet
- B.3.aamelita D. Balliao - Lupang Hinirang - Group 3Document1 pageB.3.aamelita D. Balliao - Lupang Hinirang - Group 3Mhelshy VillanuevaNo ratings yet
- B.2.a.cindy G. Awe - Concrete Poetry - Group 3Document1 pageB.2.a.cindy G. Awe - Concrete Poetry - Group 3Mhelshy VillanuevaNo ratings yet
- Managing Acute Meningitis: HistoryDocument37 pagesManaging Acute Meningitis: HistoryMhelshy VillanuevaNo ratings yet
- Etiologies and Management of Acute Bacterial MeningitisDocument41 pagesEtiologies and Management of Acute Bacterial MeningitisMhelshy VillanuevaNo ratings yet
- Peppercorn MesisskkknnnDocument40 pagesPeppercorn MesisskkknnnMhelshy VillanuevaNo ratings yet
- Peppercorn MesissDocument42 pagesPeppercorn MesissMhelshy VillanuevaNo ratings yet
- Peppercorn MesisskkknnnDocument40 pagesPeppercorn MesisskkknnnMhelshy VillanuevaNo ratings yet
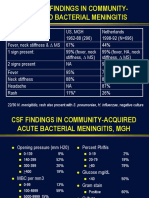
- CSF Findings in Community-Acquired Acute Bacterial Meningitis, MGHDocument34 pagesCSF Findings in Community-Acquired Acute Bacterial Meningitis, MGHMhelshy VillanuevaNo ratings yet
- Clinical Findings in Community-Acquired Bacterial MeningitisDocument35 pagesClinical Findings in Community-Acquired Bacterial MeningitisMhelshy VillanuevaNo ratings yet
- Peppercorn MeDocument45 pagesPeppercorn MeMhelshy VillanuevaNo ratings yet
- Managing Acute Meningitis: History, Clinical Findings, Treatment GuidelinesDocument38 pagesManaging Acute Meningitis: History, Clinical Findings, Treatment GuidelinesMhelshy VillanuevaNo ratings yet
- Peppercorn MesDocument44 pagesPeppercorn MesMhelshy VillanuevaNo ratings yet
- Case Example: Presents For Evaluation When He Starts To Notice Faint Rash On Trunk, Back and Arms No Known Sick ContactsDocument46 pagesCase Example: Presents For Evaluation When He Starts To Notice Faint Rash On Trunk, Back and Arms No Known Sick ContactsMhelshy VillanuevaNo ratings yet
- Diagnosis and Management of Acute Bacterial MeningitisDocument47 pagesDiagnosis and Management of Acute Bacterial MeningitisMhelshy VillanuevaNo ratings yet
- What's Causing His MeningitisDocument43 pagesWhat's Causing His MeningitisMhelshy VillanuevaNo ratings yet
- Diagnosis and Management of Acute Bacterial MeningitisDocument47 pagesDiagnosis and Management of Acute Bacterial MeningitisMhelshy VillanuevaNo ratings yet
- Diagnosis and Management of Acute Bacterial MeningitisDocument47 pagesDiagnosis and Management of Acute Bacterial MeningitisMhelshy VillanuevaNo ratings yet
- Diagnosis and Management of Acute Bacterial MeningitisDocument47 pagesDiagnosis and Management of Acute Bacterial MeningitisMhelshy VillanuevaNo ratings yet
- History of ChemistryDocument4 pagesHistory of ChemistryMhelshy VillanuevaNo ratings yet
- History of ChemistryDocument4 pagesHistory of ChemistryMhelshy VillanuevaNo ratings yet
- Midwifery Program CatalogueDocument20 pagesMidwifery Program CatalogueMhelshy Villanueva100% (1)
- Diagnosis and Management of Acute Bacterial MeningitisDocument47 pagesDiagnosis and Management of Acute Bacterial MeningitisMhelshy VillanuevaNo ratings yet
- History of Iglesia Ni Cristo: Is Christ God?Document2 pagesHistory of Iglesia Ni Cristo: Is Christ God?Mhelshy VillanuevaNo ratings yet
- Bayangan-Milo Nuptial Narciso & NoemiDocument2 pagesBayangan-Milo Nuptial Narciso & NoemiMhelshy VillanuevaNo ratings yet
- NCPDocument3 pagesNCPranee diane0% (1)
- Our History, and Theirs - Alrich Rovananda BrataDocument5 pagesOur History, and Theirs - Alrich Rovananda BrataAlrich BrataNo ratings yet
- Acute Appendicitis Complications and TreatmentDocument28 pagesAcute Appendicitis Complications and Treatmentsimi yNo ratings yet
- Pneumothorax, Tension and TraumaticDocument24 pagesPneumothorax, Tension and TraumaticSatria WibawaNo ratings yet
- EBOOK Infection Control and Management of Hazardous Materials For The Dental Team Download Full Chapter PDF KindleDocument62 pagesEBOOK Infection Control and Management of Hazardous Materials For The Dental Team Download Full Chapter PDF Kindlemichael.carathers448100% (36)
- Dr. Maimoona AliDocument34 pagesDr. Maimoona AliAli HafeezNo ratings yet
- Small PoxDocument7 pagesSmall PoxsunnyxmNo ratings yet
- Ayurvedic Herbs (PDFDrive)Document84 pagesAyurvedic Herbs (PDFDrive)siesmannNo ratings yet
- Physiotherapy Practice McqsDocument9 pagesPhysiotherapy Practice McqsSyeda Sakina AsgharNo ratings yet
- Concept Map 1Document3 pagesConcept Map 1Rubie Ann TillorNo ratings yet
- Hospital PneumoniaDocument12 pagesHospital PneumoniaKartika RezkyNo ratings yet
- Of Physical Medicine & Rehabilitation, Marmara University, Istanbul TURKEY Mediterranean Forum of Physical Medicine and RehabilitationDocument46 pagesOf Physical Medicine & Rehabilitation, Marmara University, Istanbul TURKEY Mediterranean Forum of Physical Medicine and RehabilitationneareastspineNo ratings yet
- Naturex Gingest PDFDocument5 pagesNaturex Gingest PDFyuricpNo ratings yet
- Nosocomial InfectionDocument30 pagesNosocomial InfectionZephas HillsNo ratings yet
- Cranial Nerve Worksheet AnswersDocument2 pagesCranial Nerve Worksheet AnswersWilner SiarotNo ratings yet
- Managing Pain After AppendectomyDocument2 pagesManaging Pain After AppendectomyChatoh SanaoNo ratings yet
- CNS PathologyDocument10 pagesCNS Pathologysarguss1483% (6)
- Chapter 6 NeoplasiaDocument24 pagesChapter 6 Neoplasiahenna patelNo ratings yet
- 6th Science Source of Food Notes PDFDocument2 pages6th Science Source of Food Notes PDFPankaj ARORANo ratings yet
- Face Masks Are Not Effective?Document5 pagesFace Masks Are Not Effective?Adam FernandezNo ratings yet
- ThyroidDocument84 pagesThyroidMeLissa Pearl GuillermoNo ratings yet
- Anxiety Disorder - DSM 5Document57 pagesAnxiety Disorder - DSM 5Rizky Indah Soraya100% (1)
- Clinical Teaching Ecg InterpretationDocument25 pagesClinical Teaching Ecg InterpretationAnusha VergheseNo ratings yet
- CLL Case PresentationDocument17 pagesCLL Case PresentationAhmed EshraNo ratings yet
- Chapter 14. Patient Clinical EvaluationDocument13 pagesChapter 14. Patient Clinical Evaluationedwinp21No ratings yet