You might also like
- 3 Step NutritionDocument12 pages3 Step NutritionIonut Chicinas100% (1)
- Vanity TricepsDocument16 pagesVanity TricepsIonut Chicinas100% (1)
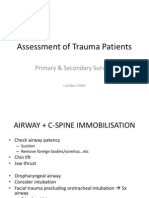
- Primary SurveyDocument19 pagesPrimary SurveyCaroline ChauNo ratings yet
- Standard Precaution: Prof. Dr. Ida Parwati, PHDDocument23 pagesStandard Precaution: Prof. Dr. Ida Parwati, PHDPutri Senna Rahayu100% (2)
- Chapter 06. Medical and Surgical AsepsisDocument19 pagesChapter 06. Medical and Surgical AsepsisChino Isiah CañeteNo ratings yet
- Isolation TechniqueDocument19 pagesIsolation Techniquejenn21283% (6)
- Systemic Manifestations of Skin DisordersDocument41 pagesSystemic Manifestations of Skin DisordersMeighalah ArumugamNo ratings yet
- Isolation PrecautionsDocument13 pagesIsolation Precautionsmalyn1218No ratings yet
- INFECTION CONTROL by Sandra WilsonDocument24 pagesINFECTION CONTROL by Sandra WilsonsandraNo ratings yet
- Infection Prevention and Control PPE (Personal Protecting Equipment)Document37 pagesInfection Prevention and Control PPE (Personal Protecting Equipment)Ahmad Sobih100% (1)
- Fluid, Electrolyte, and Acid-Base Disorders Robert B Schonberger 2018Document18 pagesFluid, Electrolyte, and Acid-Base Disorders Robert B Schonberger 2018Akhmad Fadhiel Noor100% (1)
- 6 Ways To Keep Getting StrongerDocument10 pages6 Ways To Keep Getting StrongerIonut Chicinas100% (1)
- Ms Infection ControlDocument68 pagesMs Infection ControlMa.angela Vaneza MendozaNo ratings yet
- MODULE 7 Infection ControlDocument43 pagesMODULE 7 Infection ControlBitoy AlarconNo ratings yet
- The Infection Control Manual: Standard PrecautionsDocument5 pagesThe Infection Control Manual: Standard Precautionszenagit123456No ratings yet
- Prepration of The Isolation UnitDocument43 pagesPrepration of The Isolation UnitGayatri MudliyarNo ratings yet
- Infection Control Practices in WorkplaceDocument28 pagesInfection Control Practices in WorkplaceJames Patrick Dizon100% (1)
- UTIDocument57 pagesUTIGireesh NagaruruNo ratings yet
- 5.infection Control & Standard PrecautionsDocument33 pages5.infection Control & Standard PrecautionsGilbert JohnNo ratings yet
- Barrier NursingDocument5 pagesBarrier NursingShiny Preethi100% (1)
- 2chain of DiseaseDocument43 pages2chain of Diseaseyuuki konno100% (1)
- Isolation PrecautionsDocument58 pagesIsolation PrecautionsDrShereen Fawzy HafezNo ratings yet
- Kis and MegDocument31 pagesKis and MegkisNo ratings yet
- Universal PrecautionsDocument4 pagesUniversal PrecautionsRasheena Alaja JainalNo ratings yet
- Clinical Ward CatedralDocument4 pagesClinical Ward Catedralje-ann catedralNo ratings yet
- Personal Protective Equipment (PPE) - Equipment That Creates A Barrier Between InfectiousDocument4 pagesPersonal Protective Equipment (PPE) - Equipment That Creates A Barrier Between InfectiousJp Rizal IPCCNo ratings yet
- Infection ControlDocument14 pagesInfection ControlShiba AbdullahNo ratings yet
- HostDocument21 pagesHostJoanna DagohoyNo ratings yet
- Medical and Surgical AsepsisDocument40 pagesMedical and Surgical AsepsisFrancr ToledanoNo ratings yet
- Standard PrecautionDocument51 pagesStandard PrecautionLovelights ZamoraNo ratings yet
- 3promoting Asepsis and Preventing InfectionDocument20 pages3promoting Asepsis and Preventing InfectionKaren Joy MagbanuaNo ratings yet
- Management of Infectious DiseaseDocument17 pagesManagement of Infectious DiseaseLeni CarununganNo ratings yet
- Infection Prevention and Control: Novita Kurnia SariDocument8 pagesInfection Prevention and Control: Novita Kurnia SariHesti FathanNo ratings yet
- Unit-6 Concept of IsolationDocument46 pagesUnit-6 Concept of Isolationabdulsaboor30No ratings yet
- General Infection Control MeasuresDocument40 pagesGeneral Infection Control MeasuresZllison Mae Teodoro MangabatNo ratings yet
- Standard PrecautionsDocument20 pagesStandard PrecautionspomiakhterNo ratings yet
- Chapter 6, Isolation VDocument46 pagesChapter 6, Isolation Vfarooqahmadmughal456No ratings yet
- Infection Control PracticesDocument5 pagesInfection Control PracticesMaryNo ratings yet
- Overview of Patient Isolation PrecautionsDocument2 pagesOverview of Patient Isolation PrecautionsCrystal AyalaNo ratings yet
- Lec 4 Precautions - A Lec 6Document19 pagesLec 4 Precautions - A Lec 6mqbljbr529No ratings yet
- TransmissionDocument7 pagesTransmissionJennifer TarrazonaNo ratings yet
- Hap Lo5Document8 pagesHap Lo5cjNo ratings yet
- Standard Precaution HandoutDocument3 pagesStandard Precaution Handoutaringkinking100% (1)
- Suraj Clinical Management of COVID 19Document23 pagesSuraj Clinical Management of COVID 19H.M RathodNo ratings yet
- Public Health Information Sheet: General Infection Control MeasuresDocument4 pagesPublic Health Information Sheet: General Infection Control MeasuresAjay Pal NattNo ratings yet
- INFECTION CONTROL 2nd YearDocument12 pagesINFECTION CONTROL 2nd YearAmy LalringhluaniNo ratings yet
- 2 Infection Prevention and ControlDocument5 pages2 Infection Prevention and ControlLiane BartolomeNo ratings yet
- HandwashingDocument36 pagesHandwashingidelleequibalNo ratings yet
- Standard Precaution: Presented By: G. Lynne Chancy, MSN, Arnp, Acagnp-B Adjunct Professor of Nursing MAY 2016Document23 pagesStandard Precaution: Presented By: G. Lynne Chancy, MSN, Arnp, Acagnp-B Adjunct Professor of Nursing MAY 2016Alain Chery0% (1)
- OUTFOXCDCStandardPrecautions PDFDocument2 pagesOUTFOXCDCStandardPrecautions PDFmorris_tyoNo ratings yet
- Aplikasi K3 Dalam Keperawatan: Ns. Endah Suprihatin, M.Kep., SP - MatDocument44 pagesAplikasi K3 Dalam Keperawatan: Ns. Endah Suprihatin, M.Kep., SP - MatDinda tri agustinNo ratings yet
- LECLAB3 MP Controlling Microbial Growth RemovedDocument31 pagesLECLAB3 MP Controlling Microbial Growth RemovedPriya ManobalNo ratings yet
- Universal Precautions Transmission Based PrecautionsDocument61 pagesUniversal Precautions Transmission Based PrecautionsShalamNo ratings yet
- Universal Precautions (UP)Document26 pagesUniversal Precautions (UP)Avigael Gabriel AvilesNo ratings yet
- Topic B Topic Title: Surgical and Medical Asepsis Topic ObjectivesDocument16 pagesTopic B Topic Title: Surgical and Medical Asepsis Topic ObjectivesZyrene RiveraNo ratings yet
- Nursing Foundation: Unit Xi Infection Control in Clinicl SettingDocument45 pagesNursing Foundation: Unit Xi Infection Control in Clinicl Settingbemina jaNo ratings yet
- Chapter 6Document41 pagesChapter 6Challe MontemayorNo ratings yet
- Standard PrecautionsDocument4 pagesStandard PrecautionsEthel May AlabastroNo ratings yet
- Standard Precautions 1Document34 pagesStandard Precautions 1Savita HanamsagarNo ratings yet
- Dr. Nadia Aziz C.A.B.C.M Baghdad Medical CollegeDocument39 pagesDr. Nadia Aziz C.A.B.C.M Baghdad Medical CollegeMazinNo ratings yet
- Isolationwardinhospital 180913070258Document34 pagesIsolationwardinhospital 180913070258Lorna MiroNo ratings yet
- PMLS2 2Document45 pagesPMLS2 2john dale duranoNo ratings yet
- Standard Precautions in Health CareDocument4 pagesStandard Precautions in Health CareCityhealthoffice SantiagoNo ratings yet
- CURSUL 2 Bis - Aplicatiile Practice Ale Precautiunilor StandardDocument34 pagesCURSUL 2 Bis - Aplicatiile Practice Ale Precautiunilor Standardsorin LucaNo ratings yet
- Survival Skills: How to Survive Anything and Anywhere in the World (A Comprehensive Guide to Preparing for and Overcoming Challenges of Earthquakes)From EverandSurvival Skills: How to Survive Anything and Anywhere in the World (A Comprehensive Guide to Preparing for and Overcoming Challenges of Earthquakes)No ratings yet
- 7 Exercitii Masa MuscularaDocument1 page7 Exercitii Masa MuscularaIonut ChicinasNo ratings yet
- Surgical Management in LeprosyDocument33 pagesSurgical Management in Leprosynsv.epicNo ratings yet
- Scenarios For HIV Test Counselling Role Plays: Scenario 1Document4 pagesScenarios For HIV Test Counselling Role Plays: Scenario 1ayan khwajaNo ratings yet
- 01 General Pharmacology History IntroductionDocument10 pages01 General Pharmacology History Introductionpmily100% (1)
- تجميعات مزاولة و بورد و توظيف تحديث 8-2016Document86 pagesتجميعات مزاولة و بورد و توظيف تحديث 8-2016Mahitab M. Alkhoudary80% (5)
- Ref 27 Mortalitas Pada Malnutrisi DG AMLDocument9 pagesRef 27 Mortalitas Pada Malnutrisi DG AMLmuarifNo ratings yet
- Neocon 2017Document71 pagesNeocon 2017Jasleen KaurNo ratings yet
- Anesthesia: Sanda-Maria CopotoiuDocument94 pagesAnesthesia: Sanda-Maria CopotoiuAdriana VillarrealNo ratings yet
- Research Letter: Lili Chan, Nicholas Fuca, Etti Zeldis, Kirk N. Campbell, and Aisha ShaikhDocument3 pagesResearch Letter: Lili Chan, Nicholas Fuca, Etti Zeldis, Kirk N. Campbell, and Aisha ShaikhBala MuraliNo ratings yet
- Chapter 4: Implementing The Pharmacists' Patient Care ProcessDocument15 pagesChapter 4: Implementing The Pharmacists' Patient Care ProcessLouise TheunisNo ratings yet
- 2022 - Economics of AI in Healthcare Diagonosis Vs TreatmentDocument38 pages2022 - Economics of AI in Healthcare Diagonosis Vs TreatmentAlok Kumar SinghNo ratings yet
- Table of Benefits - 140104782Document7 pagesTable of Benefits - 140104782Jeff Sy BrionesNo ratings yet
- DM General Surgery CurriculumDocument45 pagesDM General Surgery CurriculumGiovanni HenryNo ratings yet
- Children's Community Nursing: Promoting Effective Teamworking For Children and Their FamiliesDocument26 pagesChildren's Community Nursing: Promoting Effective Teamworking For Children and Their FamiliesRaiHanah HasanNo ratings yet
- Mental Health Awareness SpeechDocument2 pagesMental Health Awareness SpeechJayvelle Andrea Lauzon VillanuevaNo ratings yet
- Nursing Care of A Family During A Surgical Intervention For Birth.....Document10 pagesNursing Care of A Family During A Surgical Intervention For Birth.....Keshia HadjinorNo ratings yet
- 2014 Past Attendee ListDocument16 pages2014 Past Attendee ListBhupendra SinghNo ratings yet
- Beacon Control Norm & Path (LP10-014)Document2 pagesBeacon Control Norm & Path (LP10-014)psychejaneNo ratings yet
- Symptoms and Signs: Compartment SyndromeDocument4 pagesSymptoms and Signs: Compartment SyndromeajeikoNo ratings yet
- Novilyn C. Pataray Bsn-Ii Retinophathy: St. Paul College of Ilocos SurDocument1 pageNovilyn C. Pataray Bsn-Ii Retinophathy: St. Paul College of Ilocos SurCharina AubreyNo ratings yet
- Treatment of Hyperprolactinemia A.7Document4 pagesTreatment of Hyperprolactinemia A.7Leyni fanny guerrero limaNo ratings yet
- Drug StudyDocument17 pagesDrug StudyJhucyl Mae GalvezNo ratings yet
- Basic First AidDocument3 pagesBasic First AidAlexandra VelascoNo ratings yet
- Factors Influencing Responses To DrugsDocument3 pagesFactors Influencing Responses To Drugselle belloNo ratings yet
- Neoplasia: Basic PathologyDocument12 pagesNeoplasia: Basic Pathologyandroid tricksNo ratings yet
- Medicina 58 01115 v2Document21 pagesMedicina 58 01115 v2silmanuryanzila2705No ratings yet
- RS OnlineDocument28 pagesRS OnlineAnugrah Prasetyo AjiNo ratings yet