You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5796)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Evolution of A GoblinDocument2,042 pagesThe Evolution of A GoblinNabeel HasanNo ratings yet
- KetotifenDocument7 pagesKetotifenZauzaa NabilaNo ratings yet
- Dizziness, Unsteadiness, Visual Disturbances, and Sensorimotor Control in Traumatic Neck PainDocument14 pagesDizziness, Unsteadiness, Visual Disturbances, and Sensorimotor Control in Traumatic Neck PainMarco NgNo ratings yet
- Nacc Catalog - WebDocument54 pagesNacc Catalog - WebChirac OanaNo ratings yet
- MedicalDocument1 pageMedicalJohny HansomeNo ratings yet
- Mata KorneaDocument37 pagesMata KorneaRushdaNo ratings yet
- UDYAMDocument1 pageUDYAMSaurabh ShrivastavaNo ratings yet
- Common Ocular EmergenciesDocument33 pagesCommon Ocular EmergenciesMaimoona AimanNo ratings yet
- Text Neck Syndrome: Disentangling A New EpidemicDocument5 pagesText Neck Syndrome: Disentangling A New EpidemicLaura GarciaNo ratings yet
- Neuro OphthalmologyDocument23 pagesNeuro Ophthalmologysk100% (1)
- 10.total CholesterolDocument2 pages10.total Cholesteroltuan vănNo ratings yet
- Laboratory Rules and RegulationsDocument22 pagesLaboratory Rules and RegulationsSuiee GenrieeNo ratings yet
- Ophtho BookDocument181 pagesOphtho BookSymss MathewNo ratings yet
- Eye RobicsDocument28 pagesEye RobicsIsmi Raudha0% (1)
- Kasus2Blefarokonjungtivitis BlokSSS Tingkat1Document146 pagesKasus2Blefarokonjungtivitis BlokSSS Tingkat1DhikaNo ratings yet
- Neural Control and CoordinationDocument6 pagesNeural Control and CoordinationRonaldNo ratings yet
- Comparison of ZETA Fast (PTS) (Optopol Technology) PaperDocument7 pagesComparison of ZETA Fast (PTS) (Optopol Technology) PaperChee Yuan LokNo ratings yet
- Special Senses ReportingDocument17 pagesSpecial Senses ReportingVanessa LopezNo ratings yet
- Seaclean Plus 210 LTR SDSDocument9 pagesSeaclean Plus 210 LTR SDSviNo ratings yet
- The Comparison Between The People With Blurred Vision and The People With Clear Vision Using Attentional Blink ParadigmDocument19 pagesThe Comparison Between The People With Blurred Vision and The People With Clear Vision Using Attentional Blink ParadigmCymer Justine BaltazarNo ratings yet
- HDS ZycobondDocument10 pagesHDS ZycobondCatalina AstudilloNo ratings yet
- Clinical Profile of Patients of Episcleritis - A Hospital Based Study, JhansiDocument6 pagesClinical Profile of Patients of Episcleritis - A Hospital Based Study, JhansiIJAR JOURNALNo ratings yet
- Sspc-Tu 11 PDFDocument8 pagesSspc-Tu 11 PDFCarlos Villacriz100% (1)
- Eye Eye Assessment Assessment and Care and CareDocument126 pagesEye Eye Assessment Assessment and Care and CareBern NerquitNo ratings yet
- Pharmacology of The EyeDocument8 pagesPharmacology of The EyeRahul IyerNo ratings yet
- NSCV c1 July2018Document82 pagesNSCV c1 July2018taddeoNo ratings yet
- Albinism 12.24.22Document7 pagesAlbinism 12.24.22Fe Rt CionNo ratings yet
- MSDS Thinner Cat Dog00Document3 pagesMSDS Thinner Cat Dog00Sigitwinarto3No ratings yet
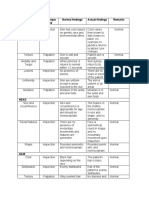
- Area Assessed Technique Used Normal Findings Actual Findings Remarks SkinDocument6 pagesArea Assessed Technique Used Normal Findings Actual Findings Remarks SkinLadybelle GototosNo ratings yet
- Arvind Eye Care - FinalDocument22 pagesArvind Eye Care - Final2005sumeet100% (2)