You might also like
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5814)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Mineral Deficiencies: Mineral Deficiency by SymptomDocument18 pagesMineral Deficiencies: Mineral Deficiency by Symptommika.100% (3)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
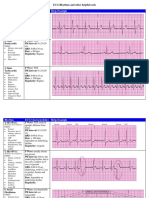
- Rhythm ECG Characteristics Strip Example: ECG Rhythms and Other Helpful ToolsDocument6 pagesRhythm ECG Characteristics Strip Example: ECG Rhythms and Other Helpful ToolsJohnildy MatiasNo ratings yet
- ECG Mastery Improving Your ECG Interpretation SkillsDocument23 pagesECG Mastery Improving Your ECG Interpretation SkillsHitesh Deora100% (2)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- ACLS PharmacologyDocument6 pagesACLS PharmacologyEunice Angela Fulgueras83% (6)
- ECG Study GuideDocument7 pagesECG Study GuideannaNo ratings yet
- Mini Test QUIZDocument9 pagesMini Test QUIZAbdul RohimNo ratings yet
- Antiarrhythmic DrugsDocument3 pagesAntiarrhythmic DrugsdoktorcoopNo ratings yet
- Aclsrhythmtest11 PDFDocument7 pagesAclsrhythmtest11 PDFmonir610% (1)
- 100 Most Important DrugsDocument13 pages100 Most Important Drugsngopya djiki67% (3)
- Medical Surgical QandADocument63 pagesMedical Surgical QandAAlona Lumidao100% (8)
- Acls Manual PDFDocument30 pagesAcls Manual PDFCyner Cruz100% (2)
- Cardiomyopathy Case StudyDocument11 pagesCardiomyopathy Case StudyJen Faye Orpilla100% (1)
- Obtaining and Interpreting EcgDocument8 pagesObtaining and Interpreting EcgAndra Elena PricopNo ratings yet
- DYSRHYTHMIASDocument9 pagesDYSRHYTHMIASgudobenNo ratings yet
- Atrioventricular Conduction AbnormalitiesDocument11 pagesAtrioventricular Conduction AbnormalitiesRaul OrtegaNo ratings yet
- Arrhythmia OF THE HEARTDocument4 pagesArrhythmia OF THE HEARTSellappan MuthusamyNo ratings yet
- SVT PresentationDocument39 pagesSVT PresentationReinsy NoviNo ratings yet
- A Review of The Cardiovascular System and ECG Performance, Troubleshooting, and InterpretationDocument47 pagesA Review of The Cardiovascular System and ECG Performance, Troubleshooting, and InterpretationRetroPilotNo ratings yet
- Junctional: TachycardiaDocument11 pagesJunctional: TachycardiachaiNo ratings yet
- Clinical Drug BaseDocument263 pagesClinical Drug BaseJackie MoonNo ratings yet
- SVT CaseDocument11 pagesSVT CaseZakiy AzzuhdiNo ratings yet
- K7 - Supraventricular Tachycardia (SVT)Document44 pagesK7 - Supraventricular Tachycardia (SVT)Zikri Putra Lan LubisNo ratings yet
- EKG Taki-Bradi AritmiaDocument47 pagesEKG Taki-Bradi Aritmiamithaa octoviagnesNo ratings yet
- Supra Ventricular TachycardiaDocument10 pagesSupra Ventricular TachycardiaJohn RobinsonNo ratings yet
- ALSDocument33 pagesALSsyahrizon thomasNo ratings yet
- Ecg ProcedureDocument5 pagesEcg ProcedureLungu AdrianNo ratings yet
- PDF Interpreting Ecgs A Practical Approach 3Rd Edition Shade Ebook Full ChapterDocument53 pagesPDF Interpreting Ecgs A Practical Approach 3Rd Edition Shade Ebook Full Chaptertanya.barnes610100% (2)
- How To Read An EKG Strip LectureDocument221 pagesHow To Read An EKG Strip LectureDemuel Dee L. BertoNo ratings yet
- Teaching Cardiac Arrhythmias A Focus On PathophysiDocument10 pagesTeaching Cardiac Arrhythmias A Focus On PathophysiJoao FonsecaNo ratings yet
- Quiz Section: Level 1Document4 pagesQuiz Section: Level 1AinunZamiraNo ratings yet