You might also like
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Nursing Education Assignment (UNIT PLAN) 1Document4 pagesNursing Education Assignment (UNIT PLAN) 1charanjit kaurNo ratings yet
- Assignment (Course Plan) 2Document3 pagesAssignment (Course Plan) 2charanjit kaurNo ratings yet
- S.G.R.D College of Nursing: AssignmentDocument3 pagesS.G.R.D College of Nursing: Assignmentcharanjit kaurNo ratings yet
- Case-Presentation-on-Pem AdvanceDocument21 pagesCase-Presentation-on-Pem Advancecharanjit kaur100% (1)
- Medical Surgical Lesson Plan 1Document7 pagesMedical Surgical Lesson Plan 1charanjit kaur100% (2)
- 2ND-Model DETAILDocument1 page2ND-Model DETAILcharanjit kaurNo ratings yet
- Demographic Data of The PatientDocument19 pagesDemographic Data of The Patientcharanjit kaurNo ratings yet
- M.S Drug StudyDocument9 pagesM.S Drug Studycharanjit kaurNo ratings yet
- Medical Surgical Seminar 2Document87 pagesMedical Surgical Seminar 2charanjit kaurNo ratings yet
- CovaAppForRecruitmentsTests PDFDocument1 pageCovaAppForRecruitmentsTests PDFcharanjit kaurNo ratings yet
- Medical Surgical Assignment 5Document2 pagesMedical Surgical Assignment 5charanjit kaurNo ratings yet
- 2ND-Model 2Document1 page2ND-Model 2charanjit kaurNo ratings yet
- Problem Statement 1 (Autosaved) Real DimpyDocument8 pagesProblem Statement 1 (Autosaved) Real Dimpycharanjit kaurNo ratings yet
- Pediatric Nutritional AssessmentDocument51 pagesPediatric Nutritional Assessmentcharanjit kaur100% (1)
- Resume of RajaDocument2 pagesResume of Rajacharanjit kaurNo ratings yet
- Lesson Plan of Education (MS (Document9 pagesLesson Plan of Education (MS (charanjit kaurNo ratings yet
- Advance Assignmnet 4Document4 pagesAdvance Assignmnet 4charanjit kaurNo ratings yet
- Health Talk On AnemiaDocument12 pagesHealth Talk On Anemiacharanjit kaurNo ratings yet
- Assignment On IMNCIDocument3 pagesAssignment On IMNCIcharanjit kaurNo ratings yet
- Second Year B.SC Nursing Master PlanDocument3 pagesSecond Year B.SC Nursing Master Plancharanjit kaur100% (1)
- Verka Milk PlantDocument8 pagesVerka Milk Plantcharanjit kaurNo ratings yet
- 2.3. Mental Health Nursing: Course DescriptionDocument5 pages2.3. Mental Health Nursing: Course Descriptioncharanjit kaurNo ratings yet
- A QUASI SynopsisDocument9 pagesA QUASI Synopsischaranjit kaurNo ratings yet
- Presentation Nursing EducationDocument22 pagesPresentation Nursing Educationcharanjit kaurNo ratings yet
- Master Plan For First Year. B.Sc. Nursing 2011-2012 X Batch: Lisie College of Nursing, Lisie Hospital, ErnakulamDocument1 pageMaster Plan For First Year. B.Sc. Nursing 2011-2012 X Batch: Lisie College of Nursing, Lisie Hospital, Ernakulamcharanjit kaurNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Badminton Coaching 2016Document32 pagesBadminton Coaching 2016dennis sabornidoNo ratings yet
- 5 6147640574871601280Document365 pages5 6147640574871601280albert david100% (39)
- Chest PBLDocument2 pagesChest PBLRamish IrfanNo ratings yet
- Lecture F2F - Seriously Injured ChildDocument22 pagesLecture F2F - Seriously Injured ChildcolinjNo ratings yet
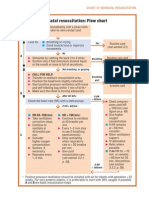
- Neonatal Resuscitation Program Flow ChartDocument3 pagesNeonatal Resuscitation Program Flow ChartChin Nam80% (5)
- Zang-Fu Syndrome Differentiation - UERMDocument113 pagesZang-Fu Syndrome Differentiation - UERMNathaniel P. Peralta0% (1)
- Unilateral Agenesis of The Lung: A Rare EntityDocument4 pagesUnilateral Agenesis of The Lung: A Rare EntityOzzy YunandarNo ratings yet
- New Born ExaminationDocument10 pagesNew Born ExaminationEn GeorgeNo ratings yet
- History Taking in Pulmonary MedicineDocument14 pagesHistory Taking in Pulmonary MedicinestudymedicNo ratings yet
- EXAM 3 20210405 C11 NUR310G.C Health Assessment PDFDocument37 pagesEXAM 3 20210405 C11 NUR310G.C Health Assessment PDFCeciliaNo ratings yet
- Benumof - Thoracic AnesthesiaDocument705 pagesBenumof - Thoracic AnesthesiaCosmin Calancia100% (5)
- TCE - Barbaric!Document57 pagesTCE - Barbaric!Phil100% (1)
- General Medicine MCQDocument11 pagesGeneral Medicine MCQsami1218100% (3)
- Pathophysiology of PneumothoraxDocument2 pagesPathophysiology of Pneumothoraxoxidalaj84% (19)
- Lesson Plan in ScienceDocument3 pagesLesson Plan in SciencePRINCESS ANGELLA SITUBALNo ratings yet
- Pemeriksaan Foto Thorax Pada Anak-AnakDocument29 pagesPemeriksaan Foto Thorax Pada Anak-AnakRenaldy PamungkasNo ratings yet
- Case Book For The Medical Students Guide To The Plain Chest FilmDocument180 pagesCase Book For The Medical Students Guide To The Plain Chest FilmMuler MeleseNo ratings yet
- Upper Back ExercisesDocument2 pagesUpper Back ExercisesMarco NgNo ratings yet
- Dr. Basil Notes - Nac Osce VipDocument255 pagesDr. Basil Notes - Nac Osce Vipamroamasha100% (18)
- Massage Guide For CoughDocument10 pagesMassage Guide For Coughice@sgNo ratings yet
- Module 6 Case Study 1 1Document3 pagesModule 6 Case Study 1 1api-675533626No ratings yet
- Thoracocentasis: INTRODUCTION:-Thoracentasis Also Known As The Thoracocentasis or Plural Tap Is AnDocument7 pagesThoracocentasis: INTRODUCTION:-Thoracentasis Also Known As The Thoracocentasis or Plural Tap Is AnaparnaNo ratings yet
- Assessment of The Trauma Patient PDFDocument25 pagesAssessment of The Trauma Patient PDFcotovairinax100% (1)
- DR Writing 001 OET Practice Letter by PASS OETDocument3 pagesDR Writing 001 OET Practice Letter by PASS OETmuthu18933% (6)
- Cases Study For Formula in Jin Gui Yao LueDocument97 pagesCases Study For Formula in Jin Gui Yao LueSergio Jesús Huapaya Gálvez100% (2)
- Emergency traumaEMQ34Document34 pagesEmergency traumaEMQ34assssadfNo ratings yet
- 8.DAY-8 ZOO - Breathing and Exchange of Gases - 25-05-2020Document11 pages8.DAY-8 ZOO - Breathing and Exchange of Gases - 25-05-2020Ramakrishna ReddyNo ratings yet
- Baba RamdevDocument8 pagesBaba RamdevMogul MagnateNo ratings yet
- Manual de La Vía Aerea en Emergencia-Walls-5ta Edicion 2018Document726 pagesManual de La Vía Aerea en Emergencia-Walls-5ta Edicion 2018María Augusta Robayo Uvilluz100% (1)
- Testing "Saintly" Authenticity: Investigations On Two Catacomb SaintsDocument8 pagesTesting "Saintly" Authenticity: Investigations On Two Catacomb SaintsRed OdisseyNo ratings yet