You might also like
- Textbook of Urgent Care Management: Chapter 41, Measuring and Improving Patient SatisfactionFrom EverandTextbook of Urgent Care Management: Chapter 41, Measuring and Improving Patient SatisfactionNo ratings yet
- Quality Improvement Project Proposal WorksheetDocument12 pagesQuality Improvement Project Proposal Worksheetapi-448506260No ratings yet
- Textbook of Urgent Care Management: Chapter 11, Urgent Care AccreditationFrom EverandTextbook of Urgent Care Management: Chapter 11, Urgent Care AccreditationNo ratings yet
- Qi Project Assignment Paper 1Document6 pagesQi Project Assignment Paper 1api-354027298No ratings yet
- Qms Project #1Document16 pagesQms Project #1GirumNo ratings yet
- DR Hanan Abbbas Assistant Professor of Family MedicineDocument27 pagesDR Hanan Abbbas Assistant Professor of Family Medicinehanan abbasNo ratings yet
- Hcin 541 ArtifactDocument11 pagesHcin 541 Artifactapi-612297093No ratings yet
- CQI by CommitteeDocument6 pagesCQI by CommitteeJhOy XiNo ratings yet
- Improving Quality of Care at Sunlight HospitalDocument7 pagesImproving Quality of Care at Sunlight HospitalTooba SiddiquiNo ratings yet
- CW AppraisalDocument34 pagesCW AppraisalWasim Paget3No ratings yet
- QA ASSURANCE HEALTHCAREDocument24 pagesQA ASSURANCE HEALTHCARERenita ChrisNo ratings yet
- Experience MappingDocument8 pagesExperience MappingGelbConsultingNo ratings yet
- Applying Lean Techniques to Improve Patient SchedulingDocument7 pagesApplying Lean Techniques to Improve Patient SchedulingjessicaNo ratings yet
- 1 SPDocument10 pages1 SPhamidi PunggawaNo ratings yet
- PNACF510Document56 pagesPNACF510Jerusalem ShiferawNo ratings yet
- RubishDocument9 pagesRubishkennedy othoroNo ratings yet
- Self EvaluationDocument4 pagesSelf EvaluationSonu Singh100% (2)
- Implementing The New Quality Assurance Framework: By: Christine Joy Alonday Bsn4Document8 pagesImplementing The New Quality Assurance Framework: By: Christine Joy Alonday Bsn4yasiraNo ratings yet
- He U.S. Hospital System Suffers From ShortfallsDocument8 pagesHe U.S. Hospital System Suffers From Shortfallsjoy gorreNo ratings yet
- Take Home ExamsDocument4 pagesTake Home Examshcny46wsjjNo ratings yet
- 2.quality Assurance in NursingDocument7 pages2.quality Assurance in NursingNancy SamuelNo ratings yet
- Key Concepts, Chapter 15, Evaluating: Critically About How Best To Evaluate The Patient's Progress Toward Valued HealthDocument4 pagesKey Concepts, Chapter 15, Evaluating: Critically About How Best To Evaluate The Patient's Progress Toward Valued HealthmsbunnileeNo ratings yet
- Describe at Least Two Purposes of ControllingDocument5 pagesDescribe at Least Two Purposes of Controllinglouie roderosNo ratings yet
- Module 5 Nursing ProcessDocument34 pagesModule 5 Nursing Processscrewdriver100% (5)
- Quality Management Programs ReviewDocument5 pagesQuality Management Programs ReviewAllan SaquinNo ratings yet
- Eyring, H. (2020)Document45 pagesEyring, H. (2020)J. RanNo ratings yet
- Reducing Waste and Improving Health Care Processes Through The Application of LeanDocument10 pagesReducing Waste and Improving Health Care Processes Through The Application of LeanLakhsmie Herawati YuwantinaNo ratings yet
- Quality Improvement ProcessDocument10 pagesQuality Improvement Processapi-284596154No ratings yet
- Project ReportDocument41 pagesProject ReportAnoop PunathilNo ratings yet
- Optima Healthcare Insurance Peer Review GuideDocument10 pagesOptima Healthcare Insurance Peer Review GuidewaleedNo ratings yet
- New Quality Improvement Plan For Reducing Patient Assessment Errors at Health FiDocument8 pagesNew Quality Improvement Plan For Reducing Patient Assessment Errors at Health Firexhudson100No ratings yet
- QMS-Concept Note (MERF)Document4 pagesQMS-Concept Note (MERF)mba07-807No ratings yet
- What Do Employer's Want For Their Employees?: Standardization With IndividualizationDocument4 pagesWhat Do Employer's Want For Their Employees?: Standardization With Individualizationapi-304631562No ratings yet
- What Do Employer's Want For Their Employees?: Standardization With IndividualizationDocument4 pagesWhat Do Employer's Want For Their Employees?: Standardization With Individualizationapi-304631562No ratings yet
- Learning Activities - Docx FinaleDocument8 pagesLearning Activities - Docx FinaleKrisia CastucianoNo ratings yet
- INTRODUCTIONDocument8 pagesINTRODUCTIONબોલતો ગુજરાતીNo ratings yet
- Clinical AuditDocument2 pagesClinical AuditTan Choong ShenNo ratings yet
- BNS Honours Nursing Quality ImprovementDocument14 pagesBNS Honours Nursing Quality ImprovementyeapgyNo ratings yet
- Quality and Safety Synthesis PaperDocument6 pagesQuality and Safety Synthesis Paperapi-252807964No ratings yet
- Nursing Process Unit-4Document27 pagesNursing Process Unit-4Rashid HussainNo ratings yet
- 2D5 Care Coordination 2014Document36 pages2D5 Care Coordination 2014Tammy Yount Di Poppante100% (1)
- Advances-Meyer 41 PDFDocument13 pagesAdvances-Meyer 41 PDFNenny Puji LestariNo ratings yet
- Licensure, Accreditation, and CertificationDocument62 pagesLicensure, Accreditation, and CertificationSohib KawaiNo ratings yet
- HealthcareDocument11 pagesHealthcarejulinthaNo ratings yet
- Quality Assurance ProcessDocument3 pagesQuality Assurance ProcessJane ChinonsoNo ratings yet
- Continuous Improvement Approach Can Optimize Manufacturing OperationsDocument15 pagesContinuous Improvement Approach Can Optimize Manufacturing OperationsMane DaralNo ratings yet
- Quality-Improvement PlanDocument11 pagesQuality-Improvement Planyhm70071No ratings yet
- Running Head: Quality Improvement Project 1Document9 pagesRunning Head: Quality Improvement Project 1api-379379776No ratings yet
- 04 eLMS Quiz 1Document4 pages04 eLMS Quiz 1Jeanette Pavo TrinidadNo ratings yet
- Nursing AuditDocument22 pagesNursing AuditBinal Joshi100% (3)
- Quality Assurance in Perioperative NursingDocument39 pagesQuality Assurance in Perioperative NursingbummyNo ratings yet
- Facts About The Hand-Off Communications ProjectDocument2 pagesFacts About The Hand-Off Communications ProjectMukhlish MudaNo ratings yet
- Quality AssuranceDocument18 pagesQuality Assurancehemihema100% (1)
- TQM in Physical TherapyDocument15 pagesTQM in Physical TherapyDina Lutfy SharafNo ratings yet
- Seminar 2 Discussion QuestionDocument7 pagesSeminar 2 Discussion Questionapi-643881078No ratings yet
- Improve Healthcare QualityDocument12 pagesImprove Healthcare Qualitykasthu75No ratings yet
- Defining Staffing:: Workforce ManagementDocument33 pagesDefining Staffing:: Workforce ManagementMari FeNo ratings yet
- The Top 6 Examples of Quality Improvement in HealthcareDocument7 pagesThe Top 6 Examples of Quality Improvement in HealthcareDennis Junior ChorumaNo ratings yet
- Tutorial Edited EditedDocument8 pagesTutorial Edited EditedBenson MabokoNo ratings yet
- Running Head: Evaluating Organizational Change 1Document11 pagesRunning Head: Evaluating Organizational Change 1klm klmNo ratings yet
- Kjenkins ServicelearningpostactivityDocument4 pagesKjenkins Servicelearningpostactivityapi-448506260No ratings yet
- Resume For E-PortfolioDocument3 pagesResume For E-Portfolioapi-448506260No ratings yet
- Kjenkins StrengthbasedleadershippaperDocument10 pagesKjenkins Strengthbasedleadershippaperapi-448506260No ratings yet
- Kjenkins ServicelearningpreactivityDocument5 pagesKjenkins Servicelearningpreactivityapi-448506260No ratings yet
- Kjenkins QidigitalposterDocument1 pageKjenkins Qidigitalposterapi-448506260No ratings yet
- KJ FinalselfcareblogDocument2 pagesKJ Finalselfcareblogapi-448506260No ratings yet
- Zero Based Budget Proposal: Improving The Obstetrical Office Triage and Scheduling Systems By: Kelley Jenkins, RNDocument16 pagesZero Based Budget Proposal: Improving The Obstetrical Office Triage and Scheduling Systems By: Kelley Jenkins, RNapi-448506260No ratings yet
- Kjenkins AdvocacymethodsmemoDocument2 pagesKjenkins Advocacymethodsmemoapi-448506260No ratings yet
- Kjenkins StrengthbasedleadershippaperDocument10 pagesKjenkins Strengthbasedleadershippaperapi-448506260No ratings yet
- Kjenkins Integrative Literature ReviewDocument26 pagesKjenkins Integrative Literature Reviewapi-448506260No ratings yet
- Root Cause AnalysisDocument6 pagesRoot Cause Analysisapi-448506260No ratings yet
- Kjenkins RnskillschecklistDocument6 pagesKjenkins Rnskillschecklistapi-448506260No ratings yet
- Jenkins PersonalphilosophyDocument6 pagesJenkins Personalphilosophyapi-448506260No ratings yet
- pedCAT BrochureDocument12 pagespedCAT BrochureVinti Singh100% (1)
- Pediatric Fundamental Critical Care SupportDocument811 pagesPediatric Fundamental Critical Care SupportSofi De Leon85% (20)
- Cranial Nerves-Anatomy and Clinical Comments Wilson-PauwelsDocument189 pagesCranial Nerves-Anatomy and Clinical Comments Wilson-PauwelsAlina Elena Tudorache100% (6)
- Placenta Previa AbruptioDocument44 pagesPlacenta Previa AbruptiorizkickyNo ratings yet
- GTDMC New Brochure, NewfinalDocument2 pagesGTDMC New Brochure, Newfinalmike tanNo ratings yet
- Application For Permit To Construct A Health FacilityDocument3 pagesApplication For Permit To Construct A Health FacilityquesterNo ratings yet
- Maternal and Child HealthDocument28 pagesMaternal and Child Health지창욱No ratings yet
- Catalog Surgical, Critical Care Dan Support Radiologi PT Megah Alkesindo 2021 5Document39 pagesCatalog Surgical, Critical Care Dan Support Radiologi PT Megah Alkesindo 2021 5gehu goc4rNo ratings yet
- Musculoskeletal Imaging 2015Document79 pagesMusculoskeletal Imaging 2015Faiq Syukri Bin SaparudinNo ratings yet
- Floppy BabyDocument13 pagesFloppy BabyJorge JhgNo ratings yet
- Prevalence of IDA among Pregnant Women in NablusDocument72 pagesPrevalence of IDA among Pregnant Women in NablusEArl CopinaNo ratings yet
- Clinical Case StudiesDocument4 pagesClinical Case StudiesThao Ngo50% (2)
- Its Over DebbieDocument1 pageIts Over DebbietakischanNo ratings yet
- HESI Test 1 PreparationDocument3 pagesHESI Test 1 Preparationestudiant9No ratings yet
- Displacement of The Uterus: DR Sahar Anwar RizkDocument32 pagesDisplacement of The Uterus: DR Sahar Anwar RizkWida Ratna SariNo ratings yet
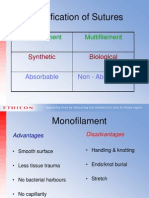
- Classification of Sutures: Monofilament MultifilamentDocument17 pagesClassification of Sutures: Monofilament Multifilamentlina_m354No ratings yet
- Ulnar Nerve EntrapmentDocument2 pagesUlnar Nerve EntrapmentboocanuuNo ratings yet
- Nas Poster FinalDocument1 pageNas Poster Finalapi-545031607No ratings yet
- Chilaiditi Syndrome - A Benign Air Under DiaphragmDocument1 pageChilaiditi Syndrome - A Benign Air Under DiaphragmBaran PalanimuthuNo ratings yet
- Process of Rapifd PrototypingDocument3 pagesProcess of Rapifd Prototypingpooja rohondiaNo ratings yet
- SHKM College AdvtDocument2 pagesSHKM College Advtnareshjangra397No ratings yet
- Covidien Product Catalogue StaplingLaparoscopy Soft Tissue RepairDocument80 pagesCovidien Product Catalogue StaplingLaparoscopy Soft Tissue RepairYiannis GkogkornasNo ratings yet
- CV: Mohd Rahime Bin Ab WahabDocument4 pagesCV: Mohd Rahime Bin Ab WahabGlobal medik indonesiaNo ratings yet
- Skin Graft Vs DC 8DRDocument2 pagesSkin Graft Vs DC 8DRibraheemNo ratings yet
- Overview of The Health System in KenyaDocument14 pagesOverview of The Health System in KenyaJohnas WanderaNo ratings yet
- Common Medical Abbreviations ListDocument3 pagesCommon Medical Abbreviations ListZyra DIOKNO0% (1)
- MDD Harm-Std-2013-01-Ojc-022Document23 pagesMDD Harm-Std-2013-01-Ojc-022Nur HayatiNo ratings yet
- MCN PartographDocument2 pagesMCN PartographAlec Anon100% (1)
- Maternal Sepsis Update - Curr Opin Anesthesiol - 2021Document6 pagesMaternal Sepsis Update - Curr Opin Anesthesiol - 2021Alex Degracia100% (1)
- Pregnancy and Alkaline WaterDocument4 pagesPregnancy and Alkaline Waterapi-320035594No ratings yet
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (14)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 3.5 out of 5 stars3.5/5 (2)
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (4)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 3.5 out of 5 stars3.5/5 (33)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (327)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 5 out of 5 stars5/5 (5)
- Summary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisFrom EverandSummary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisRating: 5 out of 5 stars5/5 (3)
- The Tennis Partner: A Doctor's Story of Friendship and LossFrom EverandThe Tennis Partner: A Doctor's Story of Friendship and LossRating: 4.5 out of 5 stars4.5/5 (4)