You might also like
- Cues: Subjective/ Objective Background of The Disease Nursing Diagnosis Goal/ Objectives Intervention Rationale EvaluationDocument3 pagesCues: Subjective/ Objective Background of The Disease Nursing Diagnosis Goal/ Objectives Intervention Rationale EvaluationMaria Margaret Macasaet0% (1)
- Nursing Care Plan For HypertensionDocument4 pagesNursing Care Plan For HypertensionKathleen Dimacali100% (2)
- NCP For CHFDocument11 pagesNCP For CHFqingwen100% (5)
- Decreased Cardiac Output Related To Decreased Myocardial Contractility Secondary To CardiomyopathyDocument2 pagesDecreased Cardiac Output Related To Decreased Myocardial Contractility Secondary To Cardiomyopathywen_pil75% (8)
- NCP Acute Pain (HTN Crisis)Document3 pagesNCP Acute Pain (HTN Crisis)Jenny AjocNo ratings yet
- Nursing Care Plan For Palliative Care Nursing NotesDocument2 pagesNursing Care Plan For Palliative Care Nursing NotesblaireNo ratings yet
- Substance AbuseDocument87 pagesSubstance AbuseJayselle ArvieNo ratings yet
- Arterial Spectral Doppler WaveformDocument21 pagesArterial Spectral Doppler WaveformL0v3B00k5100% (6)
- NCP For RS-HF (Cor PulmonaleDocument5 pagesNCP For RS-HF (Cor PulmonaleMika Saldaña100% (1)
- Dela Ysla NCPDocument4 pagesDela Ysla NCPShaira SariaNo ratings yet
- Pulmonary HypertensionDocument10 pagesPulmonary HypertensionqingwenNo ratings yet
- Anemia NCPDocument5 pagesAnemia NCPMel Christian Baldoz100% (2)
- NCPDocument4 pagesNCPElbert Vierneza100% (2)
- NCP Activity Intolerance (HTN Crisis)Document3 pagesNCP Activity Intolerance (HTN Crisis)Jenny AjocNo ratings yet
- 1-!nursing Diagnosis:: Myocardial Infarction As Evidenced by Reports of Chest Pain With Radiation in Bilateral ArmDocument3 pages1-!nursing Diagnosis:: Myocardial Infarction As Evidenced by Reports of Chest Pain With Radiation in Bilateral Armون توNo ratings yet
- Case Study NCPDocument6 pagesCase Study NCPEarl Joseph DezaNo ratings yet
- Nursing Care Plan Assessment Nursing Diagnosis Inference Planning Intervention Rationale Evaluation Short Term Goal: IndependentDocument4 pagesNursing Care Plan Assessment Nursing Diagnosis Inference Planning Intervention Rationale Evaluation Short Term Goal: IndependentasdasdasdNo ratings yet
- Decreased Cardiac OutputDocument5 pagesDecreased Cardiac Outputshuang81No ratings yet
- Nursing Care Plan Patient's Name: L. Fajardo Age: 19 Y.O AddressDocument3 pagesNursing Care Plan Patient's Name: L. Fajardo Age: 19 Y.O AddressLeticia ElricNo ratings yet
- NCP MR TMGDocument3 pagesNCP MR TMGeric macabiogNo ratings yet
- NCP AnemiaDocument2 pagesNCP AnemiaEzekiel Seth UmangayNo ratings yet
- Nursing Care Plan Assessment Diagnosis Planning Intervention Rationale EvaluationDocument10 pagesNursing Care Plan Assessment Diagnosis Planning Intervention Rationale EvaluationPantaleon PacisNo ratings yet
- Family Nursing Care PlanDocument7 pagesFamily Nursing Care PlanRebecca Caga SarmientoNo ratings yet
- 6TH NCPDocument4 pages6TH NCPjoidaNo ratings yet
- Nursing Care Plan For Doppler Scan and Stress TestingDocument10 pagesNursing Care Plan For Doppler Scan and Stress TestingAmy Rose AbuevaNo ratings yet
- Estoya, Gen Paulo C. - Anemia NCP - NCM 112 LecDocument5 pagesEstoya, Gen Paulo C. - Anemia NCP - NCM 112 LecGen Paulo EstoyaNo ratings yet
- Nursing Care Plan Acute Lymphoblastic LeukemiaDocument2 pagesNursing Care Plan Acute Lymphoblastic LeukemiabluennaNo ratings yet
- Case Report 3: Ectopic Pregnancy (Surgical) : Laboratory/Diagnostic FindingsDocument12 pagesCase Report 3: Ectopic Pregnancy (Surgical) : Laboratory/Diagnostic FindingsKM DelantarNo ratings yet
- Decreased Cardiac Output Related To Decreased Myocardial Contractility Secondary To CardiomyopathyDocument2 pagesDecreased Cardiac Output Related To Decreased Myocardial Contractility Secondary To CardiomyopathySoniaMarieBalanayNo ratings yet
- Nursing Care PlanDocument1 pageNursing Care PlanThea Lacaba AbosamaNo ratings yet
- Seminar - Heart FailuerDocument19 pagesSeminar - Heart Failuermustafalotfy01No ratings yet
- Kelompok 1 - Kelas B - Nursing English II-1Document6 pagesKelompok 1 - Kelas B - Nursing English II-1Nazimatul FitriyahNo ratings yet
- Viray, Messiah Jezreel: NCP #3 For RHDDocument3 pagesViray, Messiah Jezreel: NCP #3 For RHDJezzy VeeNo ratings yet
- Priority Problem For Severe Hypertension: Nursing Care PlanDocument3 pagesPriority Problem For Severe Hypertension: Nursing Care PlanDeanne MunarNo ratings yet
- Body-Weakness-Ncp X Drug StudyDocument3 pagesBody-Weakness-Ncp X Drug Studyhayascent hilarioNo ratings yet
- Ineffective Cerebral Tissue Perfusion Related To Interruption of Blood Flow Secondary To Hemorrhage As Evidenced by GCS of 7Document2 pagesIneffective Cerebral Tissue Perfusion Related To Interruption of Blood Flow Secondary To Hemorrhage As Evidenced by GCS of 7dana100% (4)
- DSPDocument3 pagesDSPCake ManNo ratings yet
- HypertensionDocument3 pagesHypertensionkarl de guzmanNo ratings yet
- NCP For CKDDocument4 pagesNCP For CKDMinhwa KimNo ratings yet
- NCP HomeworkDocument6 pagesNCP HomeworkAndrea Albester GarinoNo ratings yet
- Activity Intolerance NCPDocument2 pagesActivity Intolerance NCPChristopher VictoriaNo ratings yet
- Cardio Activityinto NCPDocument3 pagesCardio Activityinto NCPIcel Jean QuimboNo ratings yet
- NCP 3Document2 pagesNCP 3ABIL ABU BAKARNo ratings yet
- Activity Intolerance YAp ER NCPDocument2 pagesActivity Intolerance YAp ER NCPmecz26100% (2)
- NCP 1Document4 pagesNCP 1Jezrale FameNo ratings yet
- Medication and Nursing Care PlanDocument4 pagesMedication and Nursing Care PlanRubina MasihNo ratings yet
- IMPAIRED PHYSICAL MOBILITY RT Neuromuscular Involvement (Right Sided Paresthesia Aeb Inability To Purposefully Move Body Parts.Document2 pagesIMPAIRED PHYSICAL MOBILITY RT Neuromuscular Involvement (Right Sided Paresthesia Aeb Inability To Purposefully Move Body Parts.Senyorita KHaye67% (3)
- Abad, Izhiel C.: Assessment Diagnosis Planning Intervention Rationale EvaluationDocument3 pagesAbad, Izhiel C.: Assessment Diagnosis Planning Intervention Rationale EvaluationIzhiel AbadNo ratings yet
- Activity Intolerance NCPDocument2 pagesActivity Intolerance NCPAdriano Odysseus Jon O.No ratings yet
- Nursing Care Plan Cues Nursing Diagnosis Objective Intervention Rationale Evaluation SubjectiveDocument2 pagesNursing Care Plan Cues Nursing Diagnosis Objective Intervention Rationale Evaluation SubjectiveFreisanChenMandumotanNo ratings yet
- Revised NCP 1-3Document6 pagesRevised NCP 1-3MarcieNo ratings yet
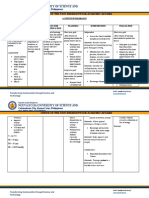
- Nueva Ecija University of Science and TechnologyDocument7 pagesNueva Ecija University of Science and TechnologyKym RonquilloNo ratings yet
- NCP Mugar Leptospirosis TLJPHDocument2 pagesNCP Mugar Leptospirosis TLJPHFRANZI ALYANNA MUGARNo ratings yet
- Nueva Ecija University of Science And: O V A ADocument2 pagesNueva Ecija University of Science And: O V A AVanessa VillanuevaNo ratings yet
- Assessment Subjective: "Apat Na Araw Na SiyangDocument2 pagesAssessment Subjective: "Apat Na Araw Na Siyangmarlon_taycoNo ratings yet
- Anemia N C P BY BHERU LALDocument1 pageAnemia N C P BY BHERU LALBheru Lal100% (1)
- Clinical Autonomic and Mitochondrial Disorders: Diagnosis, Prevention, and Treatment for Mind-Body WellnessFrom EverandClinical Autonomic and Mitochondrial Disorders: Diagnosis, Prevention, and Treatment for Mind-Body WellnessNo ratings yet
- A Simple Guide to Post-stroke Recovery, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Post-stroke Recovery, Diagnosis, Treatment and Related ConditionsNo ratings yet
- Guillain Barre Syndrome A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandGuillain Barre Syndrome A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- Polarity Therapy: How Re-Polarizing Your Body Can Heal YouFrom EverandPolarity Therapy: How Re-Polarizing Your Body Can Heal YouRating: 1 out of 5 stars1/5 (1)
- Ob ExamDocument8 pagesOb ExamJayselle ArvieNo ratings yet
- Ramilo-Act 123Document4 pagesRamilo-Act 123Jayselle ArvieNo ratings yet
- Case Study APFDocument64 pagesCase Study APFJayselle ArvieNo ratings yet
- Cerebral Infection and Cerebral InflammationDocument38 pagesCerebral Infection and Cerebral InflammationJayselle ArvieNo ratings yet
- TABIJEreflection 07Document1 pageTABIJEreflection 07Jayselle ArvieNo ratings yet
- Tabije, Arvie Jayselle P. Ncenh06Document2 pagesTabije, Arvie Jayselle P. Ncenh06Jayselle ArvieNo ratings yet
- Gerontological NursingDocument21 pagesGerontological NursingJayselle ArvieNo ratings yet
- Eating DisorderDocument57 pagesEating DisorderJayselle ArvieNo ratings yet
- Glaucoma and CataractDocument30 pagesGlaucoma and CataractJayselle ArvieNo ratings yet
- MoodDocument54 pagesMoodJayselle ArvieNo ratings yet
- 2621 Personality DisordersDocument37 pages2621 Personality DisordersJayselle ArvieNo ratings yet
- TIMI Score For NSTEMI, STEMI and Unstable AnginaDocument8 pagesTIMI Score For NSTEMI, STEMI and Unstable AnginaBenny TrisaktyariNo ratings yet
- Vertebrate Circulatory System #1Document36 pagesVertebrate Circulatory System #1Josephine Ivy JumalaNo ratings yet
- 2019 ESC/EAS Guidelines For The Management of Dyslipidaemias: Lipid Modification To Reduce Cardiovascular Risk: Supplementary DataDocument18 pages2019 ESC/EAS Guidelines For The Management of Dyslipidaemias: Lipid Modification To Reduce Cardiovascular Risk: Supplementary DataElena CosminaNo ratings yet
- Mediastinum - Lymph Node MapDocument10 pagesMediastinum - Lymph Node MapAmal-TyINo ratings yet
- Symptoms of StrokeDocument3 pagesSymptoms of StrokeMichael Pert GonzagaNo ratings yet
- Coronary ArteriesDocument28 pagesCoronary ArteriesFirst LuckNo ratings yet
- Anaesth Intensive Care 2012 LittonDocument18 pagesAnaesth Intensive Care 2012 Littonduong tien truongNo ratings yet
- Surgery - MCQ - 3rd - BHMS - (Old, New, 2015)Document57 pagesSurgery - MCQ - 3rd - BHMS - (Old, New, 2015)Anil kadamNo ratings yet
- Cardio and Hema - DR PueyoDocument161 pagesCardio and Hema - DR Pueyoapi-3735995100% (2)
- Myocardial Infarction: Ericka Jane S. Barrios, R.NDocument55 pagesMyocardial Infarction: Ericka Jane S. Barrios, R.NdantefuerteNo ratings yet
- Gabbe's Obstetrics Chapter 3 gm5.0Document30 pagesGabbe's Obstetrics Chapter 3 gm5.0AnnieNo ratings yet
- Wound Management: Using Levine's Conservation Model To Guide PracticeDocument6 pagesWound Management: Using Levine's Conservation Model To Guide PracticeGedeAriyanaKusumaNo ratings yet
- Cardiac Function Tests Anatomy of The HeartDocument8 pagesCardiac Function Tests Anatomy of The HeartJosiah BimabamNo ratings yet
- CVS and RSDocument132 pagesCVS and RSclareawambuiNo ratings yet
- Coronary Artery Disease Literature ReviewDocument4 pagesCoronary Artery Disease Literature Reviewaflsvwoeu100% (1)
- Carrel (LAncet 2023)Document16 pagesCarrel (LAncet 2023)Batoul100% (1)
- Management of ChylothoraxDocument11 pagesManagement of ChylothoraxLapjag BedahNo ratings yet
- Summary and ConclusionDocument4 pagesSummary and Conclusionhamodi222No ratings yet
- HypertensionDocument12 pagesHypertensionDr. PARMINDER NAINNo ratings yet
- Organs of The Immune SystemDocument19 pagesOrgans of The Immune SystemprabuNo ratings yet
- Flotrac BrochureDocument6 pagesFlotrac BrochureAnestesia 2017 UDECNo ratings yet
- Refreshing Shock: Pembimbing: Dr. Fauzi Abdillah Susman, SP - An, MSC Disusun Oleh: Achmad Reza SyamsuladeDocument14 pagesRefreshing Shock: Pembimbing: Dr. Fauzi Abdillah Susman, SP - An, MSC Disusun Oleh: Achmad Reza SyamsuladeSam.No ratings yet
- Cardiac Tamponade 2Document23 pagesCardiac Tamponade 2Jethro Floyd QuintoNo ratings yet
- OSCE Checklist Blood Pressure MeasurementDocument2 pagesOSCE Checklist Blood Pressure MeasurementRohullah QasimiNo ratings yet
- A. Pathway: (Lutfi, 2007 Smeltzer, 2000: 360)Document1 pageA. Pathway: (Lutfi, 2007 Smeltzer, 2000: 360)Yosef HidayatNo ratings yet
- Yanlin Ma Feb 3 PDFDocument2 pagesYanlin Ma Feb 3 PDFMitziNo ratings yet
- Pathology - Lab: Pathology of The Blood VesselsDocument5 pagesPathology - Lab: Pathology of The Blood VesselsRazel PerezNo ratings yet
- Blood Supply of BrainDocument33 pagesBlood Supply of BrainHaji BhuttoNo ratings yet
- Byscard DHTN Product PresentationDocument51 pagesByscard DHTN Product PresentationDr.abdul GhaffarNo ratings yet