You might also like
- Supraventricular TachyarrythmiasDocument172 pagesSupraventricular TachyarrythmiasAbnet WondimuNo ratings yet
- ECG Interpretation (WSAVA 2007, Boswood)Document5 pagesECG Interpretation (WSAVA 2007, Boswood)Kevin ChoyNo ratings yet
- Rate and RhythmDocument10 pagesRate and RhythmSamanta Luiza de AraujoNo ratings yet
- PrintDocument21 pagesPrintSamsudin YahyaNo ratings yet
- Atrial Flutter EmedicineDocument8 pagesAtrial Flutter EmedicineErnis Wahyu OktianaNo ratings yet
- How To Read An ECGDocument21 pagesHow To Read An ECGSlychenkoNo ratings yet
- Supraventricular Tachycardia - Life in The Fast Lane ECG LibraryDocument29 pagesSupraventricular Tachycardia - Life in The Fast Lane ECG LibraryYehuda Agus SantosoNo ratings yet
- Atrial RhythmDocument12 pagesAtrial RhythmCarlo Domingo LadieroNo ratings yet
- ECG InterpretationDocument1 pageECG InterpretationCecil-An DalanonNo ratings yet
- Practice Essentials: Essential Updates: Distinguishing Between Left-And Right-Sided Atrial TachycardiaDocument28 pagesPractice Essentials: Essential Updates: Distinguishing Between Left-And Right-Sided Atrial TachycardiaRully SyahrizalNo ratings yet
- Supraventricular TachycardiDocument8 pagesSupraventricular TachycardiHairunisa 0049No ratings yet
- Abnomalites of ECGDocument81 pagesAbnomalites of ECGgrreddy8364320No ratings yet
- 10 1016@j Cveq 2018 12 004Document18 pages10 1016@j Cveq 2018 12 004Agro PetNo ratings yet
- How To Read An ECGDocument15 pagesHow To Read An ECGSarah RonquilloNo ratings yet
- Supraventricular TachycardiaDocument9 pagesSupraventricular TachycardiaclubsanatateNo ratings yet
- ECG InterpretationDocument11 pagesECG InterpretationAndrea AndradaNo ratings yet
- Unit 7 ArrhythmiaDocument32 pagesUnit 7 ArrhythmiaJack TomarNo ratings yet
- Atrioventricular Nodal Reentry Tachycardia (AVNRT)Document24 pagesAtrioventricular Nodal Reentry Tachycardia (AVNRT)Radya Agna100% (1)
- How To Read An ECGDocument15 pagesHow To Read An ECGcharlyn206No ratings yet
- ECG - Complete Heart BlockDocument2 pagesECG - Complete Heart BlockCsilla DobrescuNo ratings yet
- Bradydysrhythmias and Atrioventricular Conduction BlocksDocument9 pagesBradydysrhythmias and Atrioventricular Conduction BlocksMariPaty LorenzoNo ratings yet
- Click Here To View: 6. Multifocal Atrial Tachycardia (MAT) and RhythmDocument1 pageClick Here To View: 6. Multifocal Atrial Tachycardia (MAT) and RhythmLwin Maung Maung ThikeNo ratings yet
- ECG EKG InterpretationDocument11 pagesECG EKG InterpretationGunma AkagiNo ratings yet
- A Most Important Question: Click Here To ViewDocument1 pageA Most Important Question: Click Here To ViewLwin Maung Maung ThikeNo ratings yet
- Atrial Flutter: The Lancet Carotid Sinus MassageDocument3 pagesAtrial Flutter: The Lancet Carotid Sinus Massageyosi rizalNo ratings yet
- ACLS Appendix 3Document32 pagesACLS Appendix 3tostc100% (1)
- Supraventricular Tachycardia: Arun Umesh Mahtani,, Devi Gopinath NairDocument17 pagesSupraventricular Tachycardia: Arun Umesh Mahtani,, Devi Gopinath Nairwindar baquero100% (1)
- Ecg Criteria SVT Vs VT: DR - Vinoth Kumar PostgraduateDocument48 pagesEcg Criteria SVT Vs VT: DR - Vinoth Kumar Postgraduatelichumo murryNo ratings yet
- Junctional Rhythms and Tachycardias: Click Here To ViewDocument1 pageJunctional Rhythms and Tachycardias: Click Here To ViewLwin Maung Maung ThikeNo ratings yet
- Chapter 5: Analyzing A Rhythm StripDocument7 pagesChapter 5: Analyzing A Rhythm StriptellyNo ratings yet
- How To Read An ECG: Confirm DetailsDocument15 pagesHow To Read An ECG: Confirm DetailsRinothja RajaratnamNo ratings yet
- Neo Pedia Guidelines Arrhythmia PDFDocument16 pagesNeo Pedia Guidelines Arrhythmia PDFkhludNo ratings yet
- Definition ECGDocument8 pagesDefinition ECGMelody BoadoNo ratings yet
- Wide Qrs Tachy 2Document6 pagesWide Qrs Tachy 2Mohit TandonNo ratings yet
- Common Arrhythmias - The Importance of ECG InterpretationDocument9 pagesCommon Arrhythmias - The Importance of ECG InterpretationDANIELA PARRA GARCIANo ratings yet
- How To Read An ECGDocument24 pagesHow To Read An ECGredroseeeeeeNo ratings yet
- Narrow QRS Complex Tachycardias: Clinical Manifestations, Diagnosis, and EvaluatDocument24 pagesNarrow QRS Complex Tachycardias: Clinical Manifestations, Diagnosis, and EvaluataspxxNo ratings yet
- Dissertation EkgDocument6 pagesDissertation EkgBuyACollegePaperOnlineMilwaukee100% (1)
- EKG InterpretationDocument63 pagesEKG InterpretationMiriam Cindy MathullaNo ratings yet
- Ecg PreparationDocument15 pagesEcg PreparationErika Danalle ArceoNo ratings yet
- Aritmii EngDocument90 pagesAritmii EngAnna HaritonencoNo ratings yet
- Accelerated Idioventricular RhythmDocument5 pagesAccelerated Idioventricular RhythmMed AmineNo ratings yet
- A. Flutter, AFDocument80 pagesA. Flutter, AFclaimstudent3515No ratings yet
- Tachycardia Approach and ManagementDocument41 pagesTachycardia Approach and ManagementChadi Alraies100% (5)
- Common Types of Supraventricular Tachycardia - Diagnosis and Management - AAFPDocument9 pagesCommon Types of Supraventricular Tachycardia - Diagnosis and Management - AAFPMohamad MostafaNo ratings yet
- Normal Sinus RhythmDocument97 pagesNormal Sinus RhythmNatasha LiberisNo ratings yet
- Basics of EKG InterpretationDocument132 pagesBasics of EKG InterpretationArif Imam HidayatNo ratings yet
- ECG StudyDocument32 pagesECG StudyDan Daniel XuNo ratings yet
- Supraventricular TachyarrythmiasDocument24 pagesSupraventricular TachyarrythmiasEINSTEIN2DNo ratings yet
- Electrocardiograph Y: Dr. Fatimah Eliana, SPPD, Kemd, FinasimDocument118 pagesElectrocardiograph Y: Dr. Fatimah Eliana, SPPD, Kemd, FinasimTommy WidjayaNo ratings yet
- 11 AvrtDocument32 pages11 AvrtthetlwinagNo ratings yet
- ECG EKG Examples and QuizDocument26 pagesECG EKG Examples and QuizBUBBUNo ratings yet
- Pre-Excitation Syndromes - LITFL - ECG Library DiagnosisDocument20 pagesPre-Excitation Syndromes - LITFL - ECG Library DiagnosisAayanNo ratings yet
- How To Read An ECGDocument13 pagesHow To Read An ECGNity Ganesan0% (1)
- Marathon-Related ECG ExasperationDocument24 pagesMarathon-Related ECG ExasperationmohamedsmnNo ratings yet
- P Wave With A Broad ( 0.04 Sec or 1 Small Square) and Deeply Negative ( 1 MM) Terminal Part in V1 P Wave Duration 0.12 Sec in Leads I and / or IIDocument9 pagesP Wave With A Broad ( 0.04 Sec or 1 Small Square) and Deeply Negative ( 1 MM) Terminal Part in V1 P Wave Duration 0.12 Sec in Leads I and / or IIpisbolsagogulamanNo ratings yet
- How To Read An ECGDocument15 pagesHow To Read An ECGCFTCNo ratings yet
- Diagram: Frontal Plane Leads-KHDocument1 pageDiagram: Frontal Plane Leads-KHLwin Maung Maung ThikeNo ratings yet
- All About Premature Beats-KHDocument1 pageAll About Premature Beats-KHLwin Maung Maung ThikeNo ratings yet
- The Three Fates of PAC's: 1. Normal Conduction 2. Aberrant Conduction 3. Non-conduction-KHDocument1 pageThe Three Fates of PAC's: 1. Normal Conduction 2. Aberrant Conduction 3. Non-conduction-KHLwin Maung Maung ThikeNo ratings yet
- Diagram: Type I vs. Type II 2nd Degree AV Block-KHDocument1 pageDiagram: Type I vs. Type II 2nd Degree AV Block-KHLwin Maung Maung ThikeNo ratings yet
- 163 7-PDF EcDocument1 page163 7-PDF EcLwin Maung Maung ThikeNo ratings yet
- Alan E. Lindsay, MD: A Teacher of Substance and StyleDocument1 pageAlan E. Lindsay, MD: A Teacher of Substance and StyleLwin Maung Maung ThikeNo ratings yet
- Pacemaker Lead Wire Placement Diagram - Marquette-KHDocument1 pagePacemaker Lead Wire Placement Diagram - Marquette-KHLwin Maung Maung ThikeNo ratings yet
- Cardiac Conduction System Diagram - Marquette-KHDocument1 pageCardiac Conduction System Diagram - Marquette-KHLwin Maung Maung ThikeNo ratings yet
- RV Vs LV PVC's - Marquette-KHDocument1 pageRV Vs LV PVC's - Marquette-KHLwin Maung Maung ThikeNo ratings yet
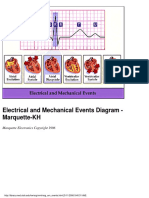
- Electrical and Mechanical Events Diagram - Marquette-KHDocument1 pageElectrical and Mechanical Events Diagram - Marquette-KHLwin Maung Maung ThikeNo ratings yet
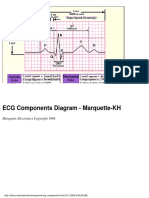
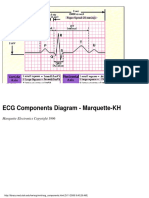
- ECG Components Diagram - Marquette-KHDocument1 pageECG Components Diagram - Marquette-KHLwin Maung Maung ThikeNo ratings yet
- Compensatory vs. Non-Compensatory Pauses - Marquette-KHDocument1 pageCompensatory vs. Non-Compensatory Pauses - Marquette-KHLwin Maung Maung ThikeNo ratings yet
- ECG Components Diagram - Marquette-KHDocument1 pageECG Components Diagram - Marquette-KHLwin Maung Maung ThikeNo ratings yet
- 151 7-PDF EcDocument1 page151 7-PDF EcLwin Maung Maung ThikeNo ratings yet
- Conceptual Framework: Arrhythmias and Conduction Abnormalities-KHDocument1 pageConceptual Framework: Arrhythmias and Conduction Abnormalities-KHLwin Maung Maung ThikeNo ratings yet
- Inferior MI: Fully Evolved-KH: Frank G.Yanowitz, M.DDocument1 pageInferior MI: Fully Evolved-KH: Frank G.Yanowitz, M.DLwin Maung Maung ThikeNo ratings yet
- 149 7-PDF EcDocument1 page149 7-PDF EcLwin Maung Maung ThikeNo ratings yet
- Diagram: Digitalis Effect On Rhythm and Conduction-KHDocument1 pageDiagram: Digitalis Effect On Rhythm and Conduction-KHLwin Maung Maung ThikeNo ratings yet
- 150 7-PDF EcDocument1 page150 7-PDF EcLwin Maung Maung ThikeNo ratings yet
- 147 7-PDF EcDocument1 page147 7-PDF EcLwin Maung Maung ThikeNo ratings yet
- High Lateral Wall MI (Seen in aVL) - KHDocument1 pageHigh Lateral Wall MI (Seen in aVL) - KHLwin Maung Maung ThikeNo ratings yet
- High Lateral Wall MI (Seen in aVL) - KHDocument1 pageHigh Lateral Wall MI (Seen in aVL) - KHLwin Maung Maung ThikeNo ratings yet
- ST Segment Depression-KH: Frank G.Yanowitz, M.DDocument1 pageST Segment Depression-KH: Frank G.Yanowitz, M.DLwin Maung Maung ThikeNo ratings yet
- 144 7-PDF EcDocument1 page144 7-PDF EcLwin Maung Maung ThikeNo ratings yet
- Left Atrial Enlargement & Nonspecific ST-T Wave Abnormalities-KHDocument1 pageLeft Atrial Enlargement & Nonspecific ST-T Wave Abnormalities-KHLwin Maung Maung ThikeNo ratings yet
- 142 7-PDF EcDocument1 page142 7-PDF EcLwin Maung Maung ThikeNo ratings yet
- A Very Subtle 1st Degree AV BlockDocument1 pageA Very Subtle 1st Degree AV BlockLwin Maung Maung ThikeNo ratings yet
- 142 7-PDF EcDocument1 page142 7-PDF EcLwin Maung Maung ThikeNo ratings yet
- Left Atrial Enlargement & Nonspecific ST-T Wave Abnormalities-KHDocument1 pageLeft Atrial Enlargement & Nonspecific ST-T Wave Abnormalities-KHLwin Maung Maung ThikeNo ratings yet
- Left Atrial Abnormality & 1st Degree AV Block-KH: Frank G.Yanowitz, M.DDocument1 pageLeft Atrial Abnormality & 1st Degree AV Block-KH: Frank G.Yanowitz, M.DLwin Maung Maung ThikeNo ratings yet
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (23)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (80)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 4 out of 5 stars4/5 (5)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (3)
- Sleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningFrom EverandSleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningRating: 4 out of 5 stars4/5 (3)
- Gut: the new and revised Sunday Times bestsellerFrom EverandGut: the new and revised Sunday Times bestsellerRating: 4 out of 5 stars4/5 (392)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDFrom EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDRating: 5 out of 5 stars5/5 (1)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisFrom EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisRating: 3.5 out of 5 stars3.5/5 (2)
- An Autobiography of Trauma: A Healing JourneyFrom EverandAn Autobiography of Trauma: A Healing JourneyRating: 5 out of 5 stars5/5 (2)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- Summary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisFrom EverandSummary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisRating: 5 out of 5 stars5/5 (3)
- 12 Rules for Life by Jordan B. Peterson - Book Summary: An Antidote to ChaosFrom Everand12 Rules for Life by Jordan B. Peterson - Book Summary: An Antidote to ChaosRating: 4.5 out of 5 stars4.5/5 (207)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (44)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)