You might also like
- Genitourinary UltrasoundDocument215 pagesGenitourinary UltrasoundAnselmus Regie100% (4)
- Uz Kontrasna SRDocument32 pagesUz Kontrasna SRjovana100% (2)
- Fundamentals of Body CT 5th EdDocument415 pagesFundamentals of Body CT 5th EdRuxandra TartaNo ratings yet
- Applied Equipment in Radio DiagnosisDocument10 pagesApplied Equipment in Radio DiagnosisVaishnobharadwaj PatiNo ratings yet
- Point-Of-care Ultrasonography N Engl J Med 3648749Document10 pagesPoint-Of-care Ultrasonography N Engl J Med 3648749Andreas Natan100% (1)
- Point of Care NHJMDocument9 pagesPoint of Care NHJMFernanda Araújo AvendanhaNo ratings yet
- Vestibular Schwannomas Diagnosis and Surgical TreaDocument10 pagesVestibular Schwannomas Diagnosis and Surgical TreaTimothy CaldwellNo ratings yet
- Fundamentals of CT PDFDocument415 pagesFundamentals of CT PDFAl Marchese100% (1)
- Jurnal 1Document10 pagesJurnal 1Putri Dery CahyaniNo ratings yet
- X-Ray Neck Carotids Heart Aorta Chest Pulmonary Kidneys Gastrointestinal LimbsDocument8 pagesX-Ray Neck Carotids Heart Aorta Chest Pulmonary Kidneys Gastrointestinal Limbsfanofchips_noodles1No ratings yet
- Thesis Endobronchial UltrasoundDocument4 pagesThesis Endobronchial Ultrasoundafknikfgd100% (2)
- Proposal New - 060952Document33 pagesProposal New - 060952sommylydiiNo ratings yet
- PIIS1053077021000537Document16 pagesPIIS1053077021000537JAVIER IZQUIERDO TAIPENo ratings yet
- Computed Tomography (CT)Document21 pagesComputed Tomography (CT)dr.anuthomas14No ratings yet
- Radiology Is A Specialty That Uses: (Hide)Document4 pagesRadiology Is A Specialty That Uses: (Hide)Dana TimushNo ratings yet
- Ultrasound (Sonography)Document14 pagesUltrasound (Sonography)dr.anuthomas14No ratings yet
- Jurnal RadiotoraxDocument5 pagesJurnal RadiotoraxKiki D. RestikaNo ratings yet
- Healthcare 09 01015Document20 pagesHealthcare 09 01015Sori B. Requena C.No ratings yet
- Medical Ultrasound - WikipediaDocument30 pagesMedical Ultrasound - WikipedianibNo ratings yet
- World's Largest Science, Technology & Medicine Open Access Book PublisherDocument18 pagesWorld's Largest Science, Technology & Medicine Open Access Book PublisherMaya LarasNo ratings yet
- Therapeutic Endoscopic UltrasoundFrom EverandTherapeutic Endoscopic UltrasoundEvangelos KalaitzakisNo ratings yet
- Diagnostic Vascular Ultrasonography With The Help of Color Doppler and Contrast-Enhanced UltrasonographyDocument13 pagesDiagnostic Vascular Ultrasonography With The Help of Color Doppler and Contrast-Enhanced Ultrasonographysudip surNo ratings yet
- Lung and Airway Ultrasound in Pediatric AnesthesiaDocument7 pagesLung and Airway Ultrasound in Pediatric Anesthesiaema moralesNo ratings yet
- Narrative Review-How To Access Nodules: Role of New Technology Including Navi-And Robo-BronchosDocument12 pagesNarrative Review-How To Access Nodules: Role of New Technology Including Navi-And Robo-Bronchosmohadese EstajiNo ratings yet
- Planning and Sizing With OsiriXHorosDocument23 pagesPlanning and Sizing With OsiriXHorosJanineNo ratings yet
- Advances in Mit 1Document6 pagesAdvances in Mit 1ayesha mahnoorNo ratings yet
- Basic Appearanceof Ultrasound Structuresand PitfallsDocument20 pagesBasic Appearanceof Ultrasound Structuresand PitfallsMateus AssisNo ratings yet
- We Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsDocument15 pagesWe Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsRui FonteNo ratings yet
- Research Paper On Ultrasound TechnologyDocument8 pagesResearch Paper On Ultrasound Technologyafnhiheaebysya100% (1)
- Veterinary Diagnostics TechniquesDocument5 pagesVeterinary Diagnostics Techniquesmarcus ciceroNo ratings yet
- X-Rays Are Especially Useful in The Detection of Pathology of The Skeletal System, But Are Also Useful ForDocument4 pagesX-Rays Are Especially Useful in The Detection of Pathology of The Skeletal System, But Are Also Useful ForJohn CrisostomoNo ratings yet
- Vena Cava DonorDocument7 pagesVena Cava Donorazizk83No ratings yet
- Contrast-Enhanced Ultrasound Imaging of Hepatic NeoplasmsFrom EverandContrast-Enhanced Ultrasound Imaging of Hepatic NeoplasmsWen-Ping WangNo ratings yet
- Pleural Ultrasonography: Paul H. Mayo, MD T, Peter Doelken, MDDocument13 pagesPleural Ultrasonography: Paul H. Mayo, MD T, Peter Doelken, MDmlannesNo ratings yet
- Ultrasound Thesis TopicsDocument6 pagesUltrasound Thesis Topicsdw9x1bxb100% (2)
- Clinical Applications of Ultrasonography in Neurocritically Ill PatientsDocument8 pagesClinical Applications of Ultrasonography in Neurocritically Ill PatientsEstefania RomanNo ratings yet
- Journal of Radiation Research and Applied Sciences: Mustafa J. Musa, Ahmed AbukonnaDocument5 pagesJournal of Radiation Research and Applied Sciences: Mustafa J. Musa, Ahmed AbukonnaLuis Mauricio Mozo MeléndezNo ratings yet
- X-Ray Contrast Media Made ClearDocument14 pagesX-Ray Contrast Media Made CleartughtedNo ratings yet
- Ultrasound A CL 2021Document17 pagesUltrasound A CL 2021Alejandra SanchezNo ratings yet
- Ecografia Pulmonar NeonatalDocument12 pagesEcografia Pulmonar NeonatalJorge CastroNo ratings yet
- UltrasoundDocument104 pagesUltrasoundlrp sNo ratings yet
- We Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsDocument27 pagesWe Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsMalikNo ratings yet
- Congenital Fetal Anomalies and The Role of Prenatal UltrassondDocument19 pagesCongenital Fetal Anomalies and The Role of Prenatal UltrassondMalu FascNo ratings yet
- Usg 17050Document7 pagesUsg 17050Amit Kumar RanoNo ratings yet
- Introduction To Ultrasound in Emergency Department: A&E Medical MeetingDocument24 pagesIntroduction To Ultrasound in Emergency Department: A&E Medical MeetingdhanudgNo ratings yet
- Possibilities of MRI Diagnostics of Focal Liver DefeatsDocument8 pagesPossibilities of MRI Diagnostics of Focal Liver DefeatsCentral Asian StudiesNo ratings yet
- Transtitional Buli CancerDocument8 pagesTranstitional Buli Cancernabila777No ratings yet
- Ultrasonic Imaging System: Hardik Tiwari (20SCE1010441) Aman Mittal (20SCSE1010518)Document10 pagesUltrasonic Imaging System: Hardik Tiwari (20SCE1010441) Aman Mittal (20SCSE1010518)Aman AgrawalNo ratings yet
- Gastrointestinal Interventional Endoscopy: Advanced TechniquesFrom EverandGastrointestinal Interventional Endoscopy: Advanced TechniquesMihir S. WaghNo ratings yet
- The Characteristic Ultrasound Features of Specific Types of Ovarian Pathology (Review)Document15 pagesThe Characteristic Ultrasound Features of Specific Types of Ovarian Pathology (Review)Sam K. AikinsNo ratings yet
- Duplex and Color Doppler Imaging of the Venous SystemFrom EverandDuplex and Color Doppler Imaging of the Venous SystemGerhard H. MostbeckNo ratings yet
- Akut Abdomen: DR Lilis, SpradDocument100 pagesAkut Abdomen: DR Lilis, SpradGaluh EkaNo ratings yet
- Ebus PDFDocument5 pagesEbus PDFNikolay ToméNo ratings yet
- AscitesDocument5 pagesAscitesSylwester SowaNo ratings yet
- Role of Transesophageal Echocardiography in Transcatheter Occlusion of Atrial Septal DefectsDocument17 pagesRole of Transesophageal Echocardiography in Transcatheter Occlusion of Atrial Septal DefectsriniambarwatiNo ratings yet
- Lympadenectomy ChapterDocument16 pagesLympadenectomy ChapterVlad CiobanuNo ratings yet
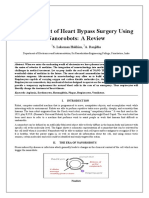
- Nanorobots The Heart SurgeonDocument7 pagesNanorobots The Heart SurgeonPoonguzhali MadhavanNo ratings yet
- Economics and Agricultural EconomicsDocument28 pagesEconomics and Agricultural EconomicsM Hossain AliNo ratings yet
- UXBenchmarking 101Document42 pagesUXBenchmarking 101Rodrigo BucketbranchNo ratings yet
- 1-Gaikindo Category Data Jandec2020Document2 pages1-Gaikindo Category Data Jandec2020Tanjung YanugrohoNo ratings yet
- Hellwalker: "What Terrors Do You Think I Have Not Already Seen?"Document2 pagesHellwalker: "What Terrors Do You Think I Have Not Already Seen?"mpotatoNo ratings yet
- TOURISM AND HOSPITALITY ORGANIZATIONS Di Pa TapooosDocument97 pagesTOURISM AND HOSPITALITY ORGANIZATIONS Di Pa TapooosDianne EvangelistaNo ratings yet
- The Rise of Political Fact CheckingDocument17 pagesThe Rise of Political Fact CheckingGlennKesslerWPNo ratings yet
- ENTRAPRENEURSHIPDocument29 pagesENTRAPRENEURSHIPTanmay Mukherjee100% (1)
- Notice: Constable (Driver) - Male in Delhi Police Examination, 2022Document50 pagesNotice: Constable (Driver) - Male in Delhi Police Examination, 2022intzar aliNo ratings yet
- Result 1st Entry Test Held On 22-08-2021Document476 pagesResult 1st Entry Test Held On 22-08-2021AsifRiazNo ratings yet
- Pilapil v. CADocument2 pagesPilapil v. CAIris Gallardo100% (2)
- The Permission Wheel Hawkes L PDFDocument8 pagesThe Permission Wheel Hawkes L PDFNandita Asthana SankerNo ratings yet
- SHS StatProb Q4 W1-8 68pgsDocument68 pagesSHS StatProb Q4 W1-8 68pgsKimberly LoterteNo ratings yet
- Medication ErrorsDocument5 pagesMedication Errorsapi-456052042No ratings yet
- Human Development IndexDocument17 pagesHuman Development IndexriyaNo ratings yet
- Haloperidol PDFDocument4 pagesHaloperidol PDFfatimahNo ratings yet
- Community Service Learning IdeasDocument4 pagesCommunity Service Learning IdeasMuneeb ZafarNo ratings yet
- VIII and IXDocument56 pagesVIII and IXTinn ApNo ratings yet
- Commercial Private Equity Announces A Three-Level Loan Program and Customized Financing Options, Helping Clients Close Commercial Real Estate Purchases in A Few DaysDocument4 pagesCommercial Private Equity Announces A Three-Level Loan Program and Customized Financing Options, Helping Clients Close Commercial Real Estate Purchases in A Few DaysPR.comNo ratings yet
- OptiX OSN 8800 6800 3800 Configuration Guide (V100R007)Document924 pagesOptiX OSN 8800 6800 3800 Configuration Guide (V100R007)vladNo ratings yet
- ANSI-ISA-S5.4-1991 - Instrument Loop DiagramsDocument22 pagesANSI-ISA-S5.4-1991 - Instrument Loop DiagramsCarlos Poveda100% (2)
- Cct4-1causal Learning PDFDocument48 pagesCct4-1causal Learning PDFsgonzalez_638672wNo ratings yet
- BSBHRM405 Support Recruitment, Selection and Induction of Staff KM2Document17 pagesBSBHRM405 Support Recruitment, Selection and Induction of Staff KM2cplerkNo ratings yet
- Ikramul (Electrical)Document3 pagesIkramul (Electrical)Ikramu HaqueNo ratings yet
- Food NutritionDocument21 pagesFood NutritionLaine AcainNo ratings yet
- Slides 99 Netslicing Georg Mayer 3gpp Network Slicing 04Document13 pagesSlides 99 Netslicing Georg Mayer 3gpp Network Slicing 04malli gaduNo ratings yet
- Wastewater Treatment: Sudha Goel, Ph.D. Department of Civil Engineering, IIT KharagpurDocument33 pagesWastewater Treatment: Sudha Goel, Ph.D. Department of Civil Engineering, IIT KharagpurSubhajit BagNo ratings yet
- LR 7833Document11 pagesLR 7833Trung ĐinhNo ratings yet
- Durst Caldera: Application GuideDocument70 pagesDurst Caldera: Application GuideClaudio BasconiNo ratings yet
- FAMILYDocument3 pagesFAMILYJenecel ZanoriaNo ratings yet
- Pasahol-Bsa1-Rizal AssignmentDocument4 pagesPasahol-Bsa1-Rizal AssignmentAngel PasaholNo ratings yet