You might also like
- EVMS Critical Care COVID-19 ProtocolDocument29 pagesEVMS Critical Care COVID-19 ProtocolJonathan LadinoNo ratings yet
- EVMS Critical Care COVID-19 ProtocolDocument23 pagesEVMS Critical Care COVID-19 ProtocoldarwinNo ratings yet
- EVMS Critical Care COVID-19 ProtocolDocument34 pagesEVMS Critical Care COVID-19 ProtocolSergiuNo ratings yet
- EVMS Critical Care COVID-19 ProtocolDocument17 pagesEVMS Critical Care COVID-19 ProtocolInternos YopalNo ratings yet
- EVMS Critical Care COVID-19 ProtocolDocument30 pagesEVMS Critical Care COVID-19 ProtocolRichard HermanNo ratings yet
- Consortium ProtocolDocument16 pagesConsortium Protocolthe kingfishNo ratings yet
- Evms Critical Care Covid-19 Management ProtocolDocument30 pagesEvms Critical Care Covid-19 Management ProtocolUsman ShoukatNo ratings yet
- EVMS Critical Care COVID-19 ProtocolDocument38 pagesEVMS Critical Care COVID-19 ProtocolDrivailaNo ratings yet
- Evms Critical Care Covid-19 Management Protocol: Paul Marik, MDDocument11 pagesEvms Critical Care Covid-19 Management Protocol: Paul Marik, MDPrashanta Barman Palas100% (1)
- COVID-19 Protocol by EVMSDocument13 pagesCOVID-19 Protocol by EVMSKrishnamurthi CG100% (1)
- EVMS Critical Care COVID-19 Protocol PDFDocument18 pagesEVMS Critical Care COVID-19 Protocol PDFGreyWolf1776No ratings yet
- Evms Critical Care Covid-19 Management ProtocolDocument39 pagesEvms Critical Care Covid-19 Management ProtocolUzletiszemNo ratings yet
- EVMS (Eastern Virginia MedicalSchool) Critical Care COVID-19 Protocol 30th November 2020Document39 pagesEVMS (Eastern Virginia MedicalSchool) Critical Care COVID-19 Protocol 30th November 2020UzletiszemNo ratings yet
- Evms Critical Care Covid-19 Management Protocol: Paul Marik, MDDocument9 pagesEvms Critical Care Covid-19 Management Protocol: Paul Marik, MDJohn GaltNo ratings yet
- FLCCC Protocols - A Guide To The Management of COVID 19 PDFDocument39 pagesFLCCC Protocols - A Guide To The Management of COVID 19 PDFSteph Cliche100% (2)
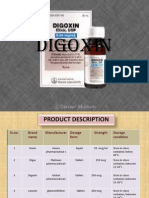
- Digitekâ® (Digoxin Tablets, Usp) Recalled (Actavis Totowa LLC) - April 28, 2008Document18 pagesDigitekâ® (Digoxin Tablets, Usp) Recalled (Actavis Totowa LLC) - April 28, 2008LenyNo ratings yet
- 07 - 10 - 21 Treatment of Covid 19 InfectionDocument26 pages07 - 10 - 21 Treatment of Covid 19 InfectionStonefalconNo ratings yet
- AIIMS Issues New Guidelines For Treatment of Covid-19 Cases: (Enter Post Title Here)Document7 pagesAIIMS Issues New Guidelines For Treatment of Covid-19 Cases: (Enter Post Title Here)senthil kumarNo ratings yet
- Imipenem, Cilastatin, and Relebactam - Drug Information - UpToDateDocument10 pagesImipenem, Cilastatin, and Relebactam - Drug Information - UpToDateMarius PapuricaNo ratings yet
- AIIMS Issues New Guidelines For Treatment of CovidDocument7 pagesAIIMS Issues New Guidelines For Treatment of Covidsenthil kumarNo ratings yet
- Monoclonal Cocktail-The Game Changer: DR - Kannan Nair Consultant-Er Sreechand Hospital, KannurDocument18 pagesMonoclonal Cocktail-The Game Changer: DR - Kannan Nair Consultant-Er Sreechand Hospital, KannurKannan NairNo ratings yet
- GentamicinDocument2 pagesGentamicinDeprama Sutikti100% (1)
- Vancomycin: Group 5 R.M 2Document31 pagesVancomycin: Group 5 R.M 2vi_wiviaNo ratings yet
- COVID-19 Antiviral and Pharmacotherapy Information: PreferentialDocument6 pagesCOVID-19 Antiviral and Pharmacotherapy Information: Preferentialmrosyidn0% (1)
- FLCCC Protocols - A Guide To The Management of COVID 19Document61 pagesFLCCC Protocols - A Guide To The Management of COVID 19Tina SangreaNo ratings yet
- April 2019-0Document25 pagesApril 2019-0SEIYADU IBRAHIM KNo ratings yet
- COVID-19 Protocol KGMU Version 6.0 17-4-21Document34 pagesCOVID-19 Protocol KGMU Version 6.0 17-4-21Kirtivaan MishraNo ratings yet
- EVMS Critical Care COVID-19 ProtocolDocument17 pagesEVMS Critical Care COVID-19 ProtocolDavid GuzmanNo ratings yet
- Spontaneous Bacterial Peritonitis Organism-Specific Therapy - Specific Organisms and Therapeutic RegimensDocument2 pagesSpontaneous Bacterial Peritonitis Organism-Specific Therapy - Specific Organisms and Therapeutic RegimensDung TranNo ratings yet
- Screenshot 2020-03-20 at 08.25.44 PDFDocument10 pagesScreenshot 2020-03-20 at 08.25.44 PDFMiguel Angel Palacios FloresNo ratings yet
- EVMS Critical Care COVID 19 Protocol 4 2 2020-RevisedDocument11 pagesEVMS Critical Care COVID 19 Protocol 4 2 2020-RevisedGabriellaNo ratings yet
- Covid 19 TreatmentDocument2 pagesCovid 19 TreatmentGio Tamaño BalisiNo ratings yet
- FLCCC Protocols - A Guide To The Management of COVID 19Document58 pagesFLCCC Protocols - A Guide To The Management of COVID 19L E100% (1)
- Medicine ManagementsDocument87 pagesMedicine ManagementsMohamed LibanNo ratings yet
- Goodman & Gilman's, The Pharmacological Basis of Therapeutics, 12 Edition, p-1538)Document6 pagesGoodman & Gilman's, The Pharmacological Basis of Therapeutics, 12 Edition, p-1538)Sandeep HavaleNo ratings yet
- MolnupiravirDocument3 pagesMolnupiravirShriefElghazalyNo ratings yet
- Drug Monograph AssignmentDocument5 pagesDrug Monograph AssignmentAdam BannonNo ratings yet
- Antibiotik For Renal FailureDocument6 pagesAntibiotik For Renal FailureWidhy Joss BangetzNo ratings yet
- Riordan Protocol For IVCDocument9 pagesRiordan Protocol For IVCNaturasfera Suplementos AlimenticiosNo ratings yet
- Vancomycin MylaninfDocument13 pagesVancomycin MylaninfAmanuel GirmayeNo ratings yet
- Micafungin Sodium-100mg Powder For Solution For InfusionDocument6 pagesMicafungin Sodium-100mg Powder For Solution For InfusionMd. Abdur RahmanNo ratings yet
- Vancomycin & Vancomycin Resistant Enterococci: Abdullah M. Kharbosh, B.SC., PharmDocument78 pagesVancomycin & Vancomycin Resistant Enterococci: Abdullah M. Kharbosh, B.SC., Pharmkharbosham100% (1)
- Aminoglycoside & VancomycinDocument10 pagesAminoglycoside & VancomycinKhor Chin PooNo ratings yet
- Intravenous Vancomycin Use in Adults - 2017Document4 pagesIntravenous Vancomycin Use in Adults - 2017Angy KarakostaNo ratings yet
- An Overview of The MATH+, I-MASK+ and I-RECOVER ProtocolsDocument55 pagesAn Overview of The MATH+, I-MASK+ and I-RECOVER ProtocolsMaung OoNo ratings yet
- Aminogycoside AntibioticsDocument31 pagesAminogycoside AntibioticsNurul Febrina100% (2)
- Digoxin Immune Therapy: ComplicationsDocument15 pagesDigoxin Immune Therapy: ComplicationsDaryl Jacob BigayNo ratings yet
- Anzcor Guideline 12 4 Medications and Fluids Aug16Document7 pagesAnzcor Guideline 12 4 Medications and Fluids Aug16flamur haskukajNo ratings yet
- Daunorubicin: Drug NameDocument7 pagesDaunorubicin: Drug NameEdgar Ledesma-MartínezNo ratings yet
- Calcitriol-0.25mcg Soft Gelatin CapsuleDocument8 pagesCalcitriol-0.25mcg Soft Gelatin CapsuleMd. Abdur RahmanNo ratings yet
- Covid Drug TherapyDocument35 pagesCovid Drug TherapyNandha KumarNo ratings yet
- DigoxinDocument20 pagesDigoxinAbdulRehmanChaudaryNo ratings yet
- FLCCC Ivermectin in The Prophylaxis and Treatment of COVID 19Document28 pagesFLCCC Ivermectin in The Prophylaxis and Treatment of COVID 19brunorepettoNo ratings yet
- Antifungal Step-Down Therapy Based On HospitalDocument8 pagesAntifungal Step-Down Therapy Based On Hospitalvaithy71No ratings yet
- Medical Management KDDocument10 pagesMedical Management KDJaen NajarNo ratings yet
- Digoxin Drug CardDocument1 pageDigoxin Drug CardMahsa Ahmadzadeh100% (2)
- Fluid Therapy in DengueDocument54 pagesFluid Therapy in DengueVithiya Chandra SagaranNo ratings yet
- 9 Drug StudyDocument11 pages9 Drug StudyJessa Mae Mauricio CastilloNo ratings yet
- Part 1: Open Games Part 3: Other Semi-Open GamesDocument7 pagesPart 1: Open Games Part 3: Other Semi-Open GamesPharmacist Ehab HammadNo ratings yet
- Engl I S Hgrammar: Ham Hot Dog Sour Cream BiscuitDocument2 pagesEngl I S Hgrammar: Ham Hot Dog Sour Cream BiscuitPharmacist Ehab HammadNo ratings yet
- T C C N: Arrant Ounty Hess EwsletterDocument2 pagesT C C N: Arrant Ounty Hess EwsletterPharmacist Ehab HammadNo ratings yet
- New Zealand Data Sheet: Page 1 of 19Document19 pagesNew Zealand Data Sheet: Page 1 of 19Pharmacist Ehab HammadNo ratings yet
- Quick Guide Dealing With Biological Chemical Dirty Bomb Attacks Poster DODDocument1 pageQuick Guide Dealing With Biological Chemical Dirty Bomb Attacks Poster DODPharmacist Ehab HammadNo ratings yet
- List of Prohibited Items: Say No To RacismDocument2 pagesList of Prohibited Items: Say No To RacismPharmacist Ehab HammadNo ratings yet
- Ielts Test 1 PDFDocument23 pagesIelts Test 1 PDFPharmacist Ehab HammadNo ratings yet
- Pharmacist Based KnowledgeDocument26 pagesPharmacist Based KnowledgePharmacist Ehab HammadNo ratings yet
- Ielts Test 1 PDFDocument23 pagesIelts Test 1 PDFBoűmřãh FōüĀdNo ratings yet
- Sci Managing Pain PDFDocument16 pagesSci Managing Pain PDFPharmacist Ehab HammadNo ratings yet
- F8DB F089:Fungal InfectionsDocument6 pagesF8DB F089:Fungal InfectionsPharmacist Ehab HammadNo ratings yet
- Otc New Items From 1-10-2013 PDFDocument1 pageOtc New Items From 1-10-2013 PDFPharmacist Ehab HammadNo ratings yet
- كرتموربلا ناحتمل ةديدج ةلئسا by./ fahmy salah: Erythrocyte Sedmentation RateDocument11 pagesكرتموربلا ناحتمل ةديدج ةلئسا by./ fahmy salah: Erythrocyte Sedmentation RatePharmacist Ehab HammadNo ratings yet
- ThymusDocument5 pagesThymusmeccha ella sojorNo ratings yet
- Pathogenesis of Graft-Versus-Host Disease (GVHD) - UpToDateDocument12 pagesPathogenesis of Graft-Versus-Host Disease (GVHD) - UpToDatemihaela popescuNo ratings yet
- Part II - Chapter 13 - Complement SystemDocument31 pagesPart II - Chapter 13 - Complement SystemVamsi Chakradhar KapagantyNo ratings yet
- Peripherally Induced Brain Tissue-Resident Memory CD8+ T Cells Mediate Protection Against CNS InfectionDocument25 pagesPeripherally Induced Brain Tissue-Resident Memory CD8+ T Cells Mediate Protection Against CNS InfectionFernandoNo ratings yet
- Hypersensitivity ReactionDocument36 pagesHypersensitivity ReactionMohana Sundaram100% (1)
- Hematology Board ReviewDocument22 pagesHematology Board ReviewEdwin OkonNo ratings yet
- Candida Revolution Free Ebook - The Candida Cancer ConnectionDocument50 pagesCandida Revolution Free Ebook - The Candida Cancer ConnectionCCWS Candida Cleanser Treatment Protocol100% (3)
- DCO Vs ETCDocument34 pagesDCO Vs ETCSebastian MihardjaNo ratings yet
- New Syllabus NCM106 2Document11 pagesNew Syllabus NCM106 2tabayoyong100% (1)
- Review Article: Autoimmune Thyroid DisordersDocument10 pagesReview Article: Autoimmune Thyroid DisordersBJ DixNo ratings yet
- Microbes (Activation and Effects)Document270 pagesMicrobes (Activation and Effects)Šï ŁãNo ratings yet
- Immunology Made Simple AF FinalDocument77 pagesImmunology Made Simple AF FinalStudy EverydayNo ratings yet
- McqsDocument10 pagesMcqsDAWOODNo ratings yet
- Serum Protein Electrophoresis: Edited by RaniDocument66 pagesSerum Protein Electrophoresis: Edited by RaniMustakim DuharingNo ratings yet
- Signature AssignmentDocument11 pagesSignature AssignmentHugoNo ratings yet
- 9700 m19 QP 12 PDFDocument16 pages9700 m19 QP 12 PDFIG UnionNo ratings yet
- 4-Cell Mediated ImmunityDocument34 pages4-Cell Mediated ImmunityleeminhoangrybirdNo ratings yet
- PLE Reviewer Pathology Inflammation and RepairDocument15 pagesPLE Reviewer Pathology Inflammation and RepairRemelou Garchitorena AlfelorNo ratings yet
- Optimal Health Blue Print MasterDocument2 pagesOptimal Health Blue Print MastermikidutzaaNo ratings yet
- Herbal Products Manufacturer Lamina Research CenterDocument30 pagesHerbal Products Manufacturer Lamina Research CenterLamina Research centerNo ratings yet
- Mohit CBC 18Document1 pageMohit CBC 18amit2352842No ratings yet
- MojoDocument2 pagesMojokike1790No ratings yet
- Value of SmileDocument5 pagesValue of SmileBerry BlueNo ratings yet
- Pharmaceutical Biotechnology-QBDocument8 pagesPharmaceutical Biotechnology-QBprateekshaNo ratings yet
- Microglia in Alzhimers JCI PaperDocument11 pagesMicroglia in Alzhimers JCI PaperRavinder SinghNo ratings yet
- Cold Agglutinin DiseaseDocument8 pagesCold Agglutinin Diseasehtunnm@gmail.comNo ratings yet
- Kikuchi-Fujimoto Disease: Adhikari RCDocument5 pagesKikuchi-Fujimoto Disease: Adhikari RCRam Chandra AdhikariNo ratings yet
- A Theory of EmotionDocument12 pagesA Theory of Emotionmihaela irofteNo ratings yet
- Bob Beck Protocol - Natural Cancer Treatments at CancerTutorDocument4 pagesBob Beck Protocol - Natural Cancer Treatments at CancerTutorThiago NunesNo ratings yet
- Catalogue: Oem/OdmDocument14 pagesCatalogue: Oem/OdmCarlito RiccyNo ratings yet