You might also like
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Dyna Lift Flyer 500 FL 000010 enDocument20 pagesDyna Lift Flyer 500 FL 000010 enErdinc SenmanNo ratings yet
- 11 Chapter 7Document14 pages11 Chapter 7ParthaSarathyNo ratings yet
- MYK Grout Card 2Document2 pagesMYK Grout Card 2Abdul Raheem SyedNo ratings yet
- Bonanza A36 ChecklistDocument10 pagesBonanza A36 Checklistalbucur100% (4)
- Refrigeration and Air Conditioning Laboratory: Lab Session 3 Absorption Refrigeration Demonstrator 816 ObjectivesDocument10 pagesRefrigeration and Air Conditioning Laboratory: Lab Session 3 Absorption Refrigeration Demonstrator 816 Objectivesjhon milliNo ratings yet
- Midterm Exam Reviewer: Surgical Handwashing QuizDocument9 pagesMidterm Exam Reviewer: Surgical Handwashing QuizOfficially RandomNo ratings yet
- Cambridge O Level: English Language 1123/22Document4 pagesCambridge O Level: English Language 1123/22Shania SeneviratneNo ratings yet
- Jurnal Dermatitis AtopikDocument20 pagesJurnal Dermatitis AtopikchintyaNo ratings yet
- Honey & Bee Product Recipes: November 2007Document29 pagesHoney & Bee Product Recipes: November 2007Kyra ThomasNo ratings yet
- D1553.140U1 German Braun Speed - Braun Card-Xi'an Yuanhua Instrument Co., LTDDocument2 pagesD1553.140U1 German Braun Speed - Braun Card-Xi'an Yuanhua Instrument Co., LTDTrong Hung NguyenNo ratings yet
- Hyperfunctional Voice DisordersDocument11 pagesHyperfunctional Voice DisordersJam PNo ratings yet
- Beeswax Craft RecipesDocument19 pagesBeeswax Craft RecipesCpetrean100% (3)
- Nikola Tesla Would Have Celebrated Christmas On January 7thDocument3 pagesNikola Tesla Would Have Celebrated Christmas On January 7thAnonymous DfeajF100% (1)
- Income Tax BasicsDocument48 pagesIncome Tax BasicsAzad Singh BajariaNo ratings yet
- FBSUPRAPAKENDocument6 pagesFBSUPRAPAKENKontczey DavidNo ratings yet
- Research ProposalDocument10 pagesResearch ProposalRonNo ratings yet
- Name: Sport: Movement PrepDocument24 pagesName: Sport: Movement PrepS HNo ratings yet
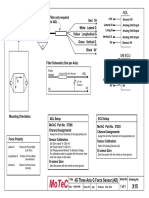
- Filter and wiring schematic for 3-axis ADL G-force sensorDocument1 pageFilter and wiring schematic for 3-axis ADL G-force sensorJuan Ramón Pérez LorenzoNo ratings yet
- The Federal Environmental Protection Authority: May 2004 Addis Ababa EthiopiaDocument44 pagesThe Federal Environmental Protection Authority: May 2004 Addis Ababa Ethiopiayared0% (1)
- From Sodomy To Safety? The Case For Defining Persecution To Include Unenforced Criminalisation of Same-Sex ConductDocument17 pagesFrom Sodomy To Safety? The Case For Defining Persecution To Include Unenforced Criminalisation of Same-Sex ConductLGBT Asylum NewsNo ratings yet
- BD 1050 PartesDocument26 pagesBD 1050 PartesFelipe RojasNo ratings yet
- Iupac 1Document15 pagesIupac 1Mayur Kumar GargNo ratings yet
- Nitrogen BlanketingDocument21 pagesNitrogen Blanketingrvkumar61No ratings yet
- Concrete Pump Hose TDSDocument2 pagesConcrete Pump Hose TDSAlaa Abu KhurjNo ratings yet
- Sedimentation Tank Design NptelDocument7 pagesSedimentation Tank Design NptelNayan HalderNo ratings yet
- Agco - DBB - f68.f69Document6 pagesAgco - DBB - f68.f69Mohd Khairi Mohd NorzianNo ratings yet
- Handling Silica in Cooling WaterDocument17 pagesHandling Silica in Cooling WaterLekhamani YadavNo ratings yet
- BKTK-2010, Failure in Material ConstructionsDocument17 pagesBKTK-2010, Failure in Material ConstructionsSorulay Way-neyNo ratings yet
- Proper Care and Use of Personal Dosimeters: HandlingDocument1 pageProper Care and Use of Personal Dosimeters: HandlingAshley JacksonNo ratings yet
- Childrens VoiceDocument26 pagesChildrens VoiceMira Alaa100% (2)