100% found this document useful (1 vote)
4K views1 pageIntake Output Chart
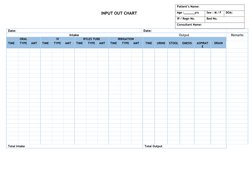
This document appears to be a chart used to track a patient's intake and output over time, including oral intake, intravenous fluids, food or medications delivered through a Ryles tube, any irrigation procedures, and output in the form of urine, stool, emesis, aspirated contents, and drainage. The chart includes spaces to record the time, type, and amount of any intake or output, as well as total intake and output amounts. It also includes fields to record the patient's name, age, sex, admission details, bed number, and consulting physician.
Uploaded by
Natasha BhasinCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as DOCX, PDF, TXT or read online on Scribd
100% found this document useful (1 vote)
4K views1 pageIntake Output Chart
This document appears to be a chart used to track a patient's intake and output over time, including oral intake, intravenous fluids, food or medications delivered through a Ryles tube, any irrigation procedures, and output in the form of urine, stool, emesis, aspirated contents, and drainage. The chart includes spaces to record the time, type, and amount of any intake or output, as well as total intake and output amounts. It also includes fields to record the patient's name, age, sex, admission details, bed number, and consulting physician.
Uploaded by
Natasha BhasinCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as DOCX, PDF, TXT or read online on Scribd