You might also like
- 8TH Edition TNM Classification and Significance of Depth of InvasionDocument75 pages8TH Edition TNM Classification and Significance of Depth of InvasionDR. ISHITA SINGHAL50% (2)
- The evolution of orthopaedic surgery and prosthesesDocument244 pagesThe evolution of orthopaedic surgery and prosthesesMarisa Piazze83% (6)
- Hong-Geun JUNG (Eds.) - Foot and Ankle Disorders - An Illustrated Reference-Springer-Verlag Berlin Heidelberg (2016)Document633 pagesHong-Geun JUNG (Eds.) - Foot and Ankle Disorders - An Illustrated Reference-Springer-Verlag Berlin Heidelberg (2016)tanyasisNo ratings yet
- Hong-Geun JUNG (Eds.) - Foot and Ankle Disorders - An Illustrated Reference-Springer-Verlag Berlin Heidelberg (2016)Document633 pagesHong-Geun JUNG (Eds.) - Foot and Ankle Disorders - An Illustrated Reference-Springer-Verlag Berlin Heidelberg (2016)tanyasisNo ratings yet
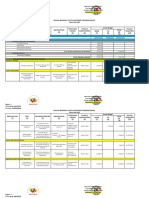
- ABYIP-2023 TemplateDocument3 pagesABYIP-2023 Templatejomar88% (26)
- H&PEDocument2 pagesH&PEDanielleNo ratings yet
- MELC-Based Health PresentationDocument17 pagesMELC-Based Health PresentationNelson Manalo88% (8)
- Dental CariesDocument42 pagesDental Cariesyongky100% (1)
- The Six Killer DiseaseDocument26 pagesThe Six Killer DiseaseFrancis Luke63% (8)
- Medical Nutrition Therapy for Pediatric Weight ManagementDocument7 pagesMedical Nutrition Therapy for Pediatric Weight Managementdakota100% (1)
- What Is MindfulnessDocument4 pagesWhat Is MindfulnessPongal PunithaNo ratings yet
- Social Work ResearchDocument15 pagesSocial Work ResearchSuresh Murugan78% (9)
- 151-Healthy-Lifestyle BenarDocument21 pages151-Healthy-Lifestyle BenarHaris PrayogoNo ratings yet
- Histomorphometric Evaluation of The Effects of Ovariectomy On Bone Turnover in Rat Caudal VertebraeDocument7 pagesHistomorphometric Evaluation of The Effects of Ovariectomy On Bone Turnover in Rat Caudal VertebraeSara HernandezNo ratings yet
- The Anatomy and Function of The Obturator ExternusDocument4 pagesThe Anatomy and Function of The Obturator ExternusAriany RomeroNo ratings yet
- Brockmeyer 2019Document11 pagesBrockmeyer 2019Jose PerezNo ratings yet
- Anterior Cruciate Ligament: An Anatomical Exploration in Humans and in A Selection of Animal SpeciesDocument11 pagesAnterior Cruciate Ligament: An Anatomical Exploration in Humans and in A Selection of Animal SpeciesMaurinho MnhNo ratings yet
- 2 2012 Attachment of The Anteroinferior Glenohumeral Ligament Labrum Complex To The Glenoid An Anatomic Study 305229222Document6 pages2 2012 Attachment of The Anteroinferior Glenohumeral Ligament Labrum Complex To The Glenoid An Anatomic Study 305229222César ArveláezNo ratings yet
- Jurnal internasional - kelenjar cowperDocument10 pagesJurnal internasional - kelenjar cowperAnggita MelaniNo ratings yet
- Acb 46 149Document8 pagesAcb 46 149soylahijadeunvampiroNo ratings yet
- Anterolateral Ligament Reconstruction Technique An Anatomic BasedDocument5 pagesAnterolateral Ligament Reconstruction Technique An Anatomic BasedEmilio Eduardo ChoqueNo ratings yet
- An Anatomic Arthroscopic Description of The Hip Capsular Ligaments For The Hip ArthroscopistDocument9 pagesAn Anatomic Arthroscopic Description of The Hip Capsular Ligaments For The Hip Arthroscopistxekar59382No ratings yet
- 2012 Article 148Document9 pages2012 Article 148João GasparNo ratings yet
- Anatomy Systematic 2016Document11 pagesAnatomy Systematic 2016Ahmed MortadaNo ratings yet
- Research Article Comparison of Structural, Architectural and Mechanical Aspects of Cellular and Acellular Bone in Two Teleost FishDocument11 pagesResearch Article Comparison of Structural, Architectural and Mechanical Aspects of Cellular and Acellular Bone in Two Teleost FishcamilaNo ratings yet
- Anatomical Study On The Anterolateral Ligament of The Knee: Original ArticleDocument6 pagesAnatomical Study On The Anterolateral Ligament of The Knee: Original ArticleAngel ArturoNo ratings yet
- Anatomy of The Anterior Cruciate Ligament With.9Document13 pagesAnatomy of The Anterior Cruciate Ligament With.9Metin HakkanNo ratings yet
- Anatomy 2Document7 pagesAnatomy 2Ahmed MortadaNo ratings yet
- Kalawadia 2018Document9 pagesKalawadia 2018سيف فلاح حسنNo ratings yet
- Biceps Femoris Tendon and Lateral Collateral Ligam PDFDocument8 pagesBiceps Femoris Tendon and Lateral Collateral Ligam PDFHONGJYNo ratings yet
- Morphological Features of The Popliteus Tendon, Popliteofibular and Lateral (Fibular) Collateral LigamentsDocument10 pagesMorphological Features of The Popliteus Tendon, Popliteofibular and Lateral (Fibular) Collateral LigamentsSaifuddin HaswareNo ratings yet
- Grupo 7 A Multidisciplinary Study of The Healing of 226432506Document7 pagesGrupo 7 A Multidisciplinary Study of The Healing of 226432506César ArveláezNo ratings yet
- The Early Development and Ossification of The Human Clavicle An Embryologic StudyDocument6 pagesThe Early Development and Ossification of The Human Clavicle An Embryologic StudyGabriel Alexandru GhiațăNo ratings yet
- Analysis of Sacrococcygeal Morphology in Koreans Using Computed TomographyDocument9 pagesAnalysis of Sacrococcygeal Morphology in Koreans Using Computed TomographyUkik SaliroNo ratings yet
- Fundamentals of Anatomy and Physiology 10th Edition Martini Solutions Manual 1Document36 pagesFundamentals of Anatomy and Physiology 10th Edition Martini Solutions Manual 1toddvaldezamzxfwnrtq96% (28)
- Gross, Arthroscopic, and Radiographicanatomiesof TheanteriorcruciateligamentDocument15 pagesGross, Arthroscopic, and Radiographicanatomiesof TheanteriorcruciateligamentDiana IparraguirreNo ratings yet
- Jexbio 27 3 264Document28 pagesJexbio 27 3 264Nikhil JohnNo ratings yet
- The “Ligamentization” Process in Anterior Cruciate Ligament Reconstruction (1)Document9 pagesThe “Ligamentization” Process in Anterior Cruciate Ligament Reconstruction (1)marcelogascon.oNo ratings yet
- Sella TurcicaDocument4 pagesSella TurcicaHeidar ZaarourNo ratings yet
- The Evolution of The Pectoral GirdleDocument6 pagesThe Evolution of The Pectoral GirdleHarsh DalalNo ratings yet
- Abjs 8 332Document11 pagesAbjs 8 332angelluis1980No ratings yet
- The Anatomy of The Anterior Cruciate Ligament and Its Relevance To The Technique of ReconstructionDocument7 pagesThe Anatomy of The Anterior Cruciate Ligament and Its Relevance To The Technique of ReconstructionMetin HakkanNo ratings yet
- Variation of Rotation Moment Arms With Hip Flexion: Scott L. Delp, William E. Hess, David S. Hungerford, Lynne C. JonesDocument9 pagesVariation of Rotation Moment Arms With Hip Flexion: Scott L. Delp, William E. Hess, David S. Hungerford, Lynne C. JonesAryan SalihNo ratings yet
- OUtcome After Limted or Extensive BursectomyDocument8 pagesOUtcome After Limted or Extensive BursectomySeno adipNo ratings yet
- The Iliotibial Tract: Imaging, Anatomy, Injuries, and Other PathologyDocument19 pagesThe Iliotibial Tract: Imaging, Anatomy, Injuries, and Other PathologyBeah Marie AlisosoNo ratings yet
- Final Thesis (Dr. Neeraj)Document79 pagesFinal Thesis (Dr. Neeraj)Prosenjit BhowalNo ratings yet
- Anatomy Summary BasicDocument54 pagesAnatomy Summary BasicDungani AllanNo ratings yet
- Prolonged Caloric Restriction Ameliorates Age Related Atro - 2021 - ExperimentalDocument10 pagesProlonged Caloric Restriction Ameliorates Age Related Atro - 2021 - ExperimentalasdfaasdgasNo ratings yet
- Tendon Del Subescapular - Sistema de Clasificación - AnatomíaDocument7 pagesTendon Del Subescapular - Sistema de Clasificación - AnatomíajesusglezctNo ratings yet
- 2014 The Anatomy of The Hip Abductors MusclesDocument13 pages2014 The Anatomy of The Hip Abductors Musclesmari netaNo ratings yet
- An Evaluation of TheDocument12 pagesAn Evaluation of TheMedrechEditorialNo ratings yet
- A Rare Anomaly of The Clavicle - Bifurcation of The Lateral One-ThirdDocument3 pagesA Rare Anomaly of The Clavicle - Bifurcation of The Lateral One-ThirdSigmundNo ratings yet
- New Insight Into The Iliofemoral Ligament Based On The Anatomical Study of The Hip Joint CapsuleDocument8 pagesNew Insight Into The Iliofemoral Ligament Based On The Anatomical Study of The Hip Joint Capsulexekar59382No ratings yet
- Kinematics Reveal Muscle Contractures Causing Knee Flexion GaitDocument17 pagesKinematics Reveal Muscle Contractures Causing Knee Flexion GaitAmanda TuckerNo ratings yet
- Journal Of: The Sacroiliac Joint: An Overview of Its Anatomy, Function and Potential Clinical ImplicationsDocument31 pagesJournal Of: The Sacroiliac Joint: An Overview of Its Anatomy, Function and Potential Clinical ImplicationsGabriel Gaspar Bike FitNo ratings yet
- Nrutik Paper PDFDocument5 pagesNrutik Paper PDFNrutik PatelNo ratings yet
- The Skeletal System of The FrogDocument3 pagesThe Skeletal System of The FrogLuther Abaya MolinaNo ratings yet
- Anatomic Posterolateral Corner Reconstruction With AutograftsDocument7 pagesAnatomic Posterolateral Corner Reconstruction With AutograftsVõ Văn Phúc ToànNo ratings yet
- Mathew 2017Document12 pagesMathew 2017Negru TeodorNo ratings yet
- Evolutionary Consequences of Skeletal DifferentiationDocument22 pagesEvolutionary Consequences of Skeletal Differentiationjulio7345No ratings yet
- Franci Oz I 2018Document7 pagesFranci Oz I 2018Carlos Mauricio Salazar BedollaNo ratings yet
- Journal of Anatomy - 2012 - Willard - The Thoracolumbar Fascia Anatomy Function and Clinical ConsiderationsDocument30 pagesJournal of Anatomy - 2012 - Willard - The Thoracolumbar Fascia Anatomy Function and Clinical ConsiderationsTamires fogaçaNo ratings yet
- Anatomical and Functional Relationships Between The External Abdominal Oblique Muscle and The Posterior Layer of The Thoracolumbar FasciaDocument8 pagesAnatomical and Functional Relationships Between The External Abdominal Oblique Muscle and The Posterior Layer of The Thoracolumbar FasciaKeneuoe MokoenaNo ratings yet
- Hypothesis of Human Penile Anatomy, Erection Hemodynamics and Their Clinical ApplicationsDocument10 pagesHypothesis of Human Penile Anatomy, Erection Hemodynamics and Their Clinical ApplicationsPeter69No ratings yet
- The Structure of The Periodontal Ligament An UpdateDocument26 pagesThe Structure of The Periodontal Ligament An UpdateNawaf RuwailiNo ratings yet
- 1998 The Anterior Tibial Vessels and Their Role in Epiphyseal and Diaphyseal Transfer of The Fibula Experimental Study and Clinical Applications.Document19 pages1998 The Anterior Tibial Vessels and Their Role in Epiphyseal and Diaphyseal Transfer of The Fibula Experimental Study and Clinical Applications.suryaNo ratings yet
- Anatomy Biomechanics Lateral Side Knee Surgical ImplicationsDocument8 pagesAnatomy Biomechanics Lateral Side Knee Surgical ImplicationsFasilNigusseNo ratings yet
- A Cadaveric Study of The Morphology of The Extensor Hallucis LongusDocument7 pagesA Cadaveric Study of The Morphology of The Extensor Hallucis LongusDavid BertossiNo ratings yet
- 1 s2.0 S0021929015001931 MainDocument7 pages1 s2.0 S0021929015001931 MainceliaNo ratings yet
- Postero Lateral Corner of KneeDocument5 pagesPostero Lateral Corner of KneeAnwar MarthyaNo ratings yet
- Kumar PDFDocument79 pagesKumar PDFLina LinuxNo ratings yet
- A Biomechanical Analysis of The Vertebral and RibDocument10 pagesA Biomechanical Analysis of The Vertebral and RibDorin DorinNo ratings yet
- Letter To The Editor: Antibiotic Prophylaxis Regimens in Trauma and Orthopaedic SurgeryDocument3 pagesLetter To The Editor: Antibiotic Prophylaxis Regimens in Trauma and Orthopaedic SurgerytanyasisNo ratings yet
- Kneeling After Total Knee Arthroplasty: Raj M. Amin, MD Vikram Vasan Julius K. Oni, MDDocument6 pagesKneeling After Total Knee Arthroplasty: Raj M. Amin, MD Vikram Vasan Julius K. Oni, MDtanyasisNo ratings yet
- Effect of Dislocation Timing Following Primary Total Hip Arthroplasty On The Risk of Redislocation and RevisionDocument7 pagesEffect of Dislocation Timing Following Primary Total Hip Arthroplasty On The Risk of Redislocation and RevisiontanyasisNo ratings yet
- Impact of Ulnar Styloid Fractures On The Treatment Effect of Distal Radius Fractures With Volar Plate Fixation: A Case Control StudyDocument8 pagesImpact of Ulnar Styloid Fractures On The Treatment Effect of Distal Radius Fractures With Volar Plate Fixation: A Case Control StudytanyasisNo ratings yet
- Injury: Andrew H. SchmidtDocument4 pagesInjury: Andrew H. SchmidttanyasisNo ratings yet
- A Protocol For The Management of Adhesive Small Bowel ObstructionDocument9 pagesA Protocol For The Management of Adhesive Small Bowel ObstructiontanyasisNo ratings yet
- Femoro Acetabular Impingement Clinical Research: Is A Composite Outcome The Answer?Document7 pagesFemoro Acetabular Impingement Clinical Research: Is A Composite Outcome The Answer?tanyasisNo ratings yet
- 2013jul SepInformedconsentIssuesandchallenges JAPTR43134 140Document8 pages2013jul SepInformedconsentIssuesandchallenges JAPTR43134 140tanyasisNo ratings yet
- Main PDFDocument5 pagesMain PDFtanyasisNo ratings yet
- Informed ConsentDocument7 pagesInformed ConsenttanyasisNo ratings yet
- Venous Thromboembolism in Over 16s Reducing The Risk of Hospitalacquired Deep Vein Thrombosis or Pulmonary Embolism PDF 1837703092165Document43 pagesVenous Thromboembolism in Over 16s Reducing The Risk of Hospitalacquired Deep Vein Thrombosis or Pulmonary Embolism PDF 1837703092165tanyasisNo ratings yet
- Informed Consent: Guidance For ApplicantsDocument7 pagesInformed Consent: Guidance For ApplicantstanyasisNo ratings yet
- Currentconceptsof Femoroacetabular Impingement: Aria Ghaffari,, Ivan Davis,, Troy Storey,, Michael MoserDocument18 pagesCurrentconceptsof Femoroacetabular Impingement: Aria Ghaffari,, Ivan Davis,, Troy Storey,, Michael MosertanyasisNo ratings yet
- Ankle Sprains: Evaluation, Rehabilitation, and Prevention: Raining Revention AND EhabilitationDocument7 pagesAnkle Sprains: Evaluation, Rehabilitation, and Prevention: Raining Revention AND EhabilitationtanyasisNo ratings yet
- Non-Steroidal Anti-In Ammatory Drugs For Spinal Pain: A Systematic Review and Meta-AnalysisDocument11 pagesNon-Steroidal Anti-In Ammatory Drugs For Spinal Pain: A Systematic Review and Meta-AnalysistanyasisNo ratings yet
- (J. K. Rowling, Mary GrandPré) Harry Potter HardcDocument376 pages(J. K. Rowling, Mary GrandPré) Harry Potter HardcDiego RobertNo ratings yet
- Osteomyelitis-Bojan Rafaj (2012) PDFDocument188 pagesOsteomyelitis-Bojan Rafaj (2012) PDFtanyasisNo ratings yet
- Wong2015 PDFDocument28 pagesWong2015 PDFtanyasisNo ratings yet
- Respiratory Tract Virus Infections in The Elderly With PneumoniaDocument11 pagesRespiratory Tract Virus Infections in The Elderly With PneumoniatanyasisNo ratings yet
- Nsaids For Chronic Low Back Pain: Jama Clinical Evidence SynopsisDocument2 pagesNsaids For Chronic Low Back Pain: Jama Clinical Evidence SynopsistanyasisNo ratings yet
- Aines 2008Document85 pagesAines 2008tanyasisNo ratings yet
- Risk Factors For N e in NeonatesDocument9 pagesRisk Factors For N e in NeonatestanyasisNo ratings yet
- Riete & CapriniDocument2 pagesRiete & CaprinitanyasisNo ratings yet
- DiniDocument10 pagesDiniMuhammad Yasdar BahriNo ratings yet
- Intestinal Dysbiosis in Preterm Infants Preceding N eDocument15 pagesIntestinal Dysbiosis in Preterm Infants Preceding N etanyasisNo ratings yet
- Stan Nard 2014Document2 pagesStan Nard 2014tanyasisNo ratings yet
- HerbicidesDocument28 pagesHerbicidesDr.KanamNo ratings yet
- Capstone SolutionDocument1 pageCapstone Solutiondave magcawasNo ratings yet
- Chap3 Display QualDocument25 pagesChap3 Display QualCatalina Sabogal OrtegónNo ratings yet
- SGL 7 (Nutrition Basics 1)Document21 pagesSGL 7 (Nutrition Basics 1)Joo Se HyukNo ratings yet
- Critical Care Update PDFDocument25 pagesCritical Care Update PDFHugo PozoNo ratings yet
- Flow rate uniformity of TARAL 200 PITON TURBO sprayer for pest controlDocument4 pagesFlow rate uniformity of TARAL 200 PITON TURBO sprayer for pest controlAndreea DiaconuNo ratings yet
- Septoplasty: Information For Patients From Head and NeckDocument4 pagesSeptoplasty: Information For Patients From Head and NeckKris RNo ratings yet
- Gronning 2017 CloningDocument4 pagesGronning 2017 CloningKlyde Orly R. YusoresNo ratings yet
- 6Document11 pages6UgaugaaNo ratings yet
- Echo - Medical Supplies and Equipment For Primary Health CareDocument192 pagesEcho - Medical Supplies and Equipment For Primary Health CareKing Solomon CatralNo ratings yet
- PT&T Policy Against Married WomenDocument12 pagesPT&T Policy Against Married WomenHershey Delos SantosNo ratings yet
- PR 2Document14 pagesPR 2Eduardo TalamanNo ratings yet
- TC Electronic M-100 User ManualDocument21 pagesTC Electronic M-100 User Manualzewdaroo9599No ratings yet
- Acute Pain Questions - LathaDocument5 pagesAcute Pain Questions - LathaNishanth yedavalliNo ratings yet
- Chapter 6 - Adipose TissueDocument13 pagesChapter 6 - Adipose TissueREMAN ALINGASANo ratings yet
- Jurnal Internasional BiofarmasetikaDocument9 pagesJurnal Internasional BiofarmasetikaHandriko DsNo ratings yet
- Xerox Wc423 SMDocument600 pagesXerox Wc423 SMkerintNo ratings yet
- What Is Moxibustion Acupuncturedrcmt PDFDocument3 pagesWhat Is Moxibustion Acupuncturedrcmt PDFStillingKruse2No ratings yet
- Aefi - Mop 2014 FinalDocument106 pagesAefi - Mop 2014 FinalJethro Floyd QuintoNo ratings yet
- 849 FullDocument13 pages849 FullAnsuf WicaksonoNo ratings yet