You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5796)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Ptr. Shem Enebrad: Certificate of RecognitionDocument9 pagesPtr. Shem Enebrad: Certificate of Recognitionrizalina maxilomNo ratings yet
- A Conceptual Model To Measure Customer S Satisfaction in Electric Power Distribution ServicesDocument22 pagesA Conceptual Model To Measure Customer S Satisfaction in Electric Power Distribution ServicesaggarwalakankshaNo ratings yet
- June 2001 North American Native Orchid JournalDocument79 pagesJune 2001 North American Native Orchid JournalNorth American Native Orchid JournalNo ratings yet
- Wireless Cellular and LTE 4G Broadband 1Document76 pagesWireless Cellular and LTE 4G Broadband 1PRANEETH DpvNo ratings yet
- Kaizen ToolsDocument43 pagesKaizen Toolssandee1983No ratings yet
- Under Water Wind Mill ReportDocument13 pagesUnder Water Wind Mill ReportASHUTOSH SAHOOLME011 (LME011)No ratings yet
- Shoib CV Scaffold EngineerDocument3 pagesShoib CV Scaffold EngineerMohd Shoib100% (1)
- Code Billing Heads Rate Quantity Amount in RsDocument2 pagesCode Billing Heads Rate Quantity Amount in RsPrasanna Nammalwar85% (27)
- Tunnel EngineeringDocument53 pagesTunnel EngineeringshankaregowdaNo ratings yet
- MobilenetV2 (Quantization)Document4 pagesMobilenetV2 (Quantization)Akash BhogarNo ratings yet
- Procurement 2023 Ten Cpo Actions To Defy The Toughest Challenges - FinalDocument8 pagesProcurement 2023 Ten Cpo Actions To Defy The Toughest Challenges - FinalDennis DuNo ratings yet
- WORKING CAPITAL MANAGEMENT of Axis Bank Finance Research 2014 2Document112 pagesWORKING CAPITAL MANAGEMENT of Axis Bank Finance Research 2014 2pawanmamaniyaNo ratings yet
- Learn To Create A Basic Calculator in Java Using NetbeansDocument9 pagesLearn To Create A Basic Calculator in Java Using NetbeansRicardo B. ViganNo ratings yet
- Manual EQD Depths PDFDocument2 pagesManual EQD Depths PDFClaudio Villagra Revisor ArqNo ratings yet
- Dunnaway Reviewer 1Document38 pagesDunnaway Reviewer 1march8200871% (7)
- Applied Geography: Marco VizzariDocument11 pagesApplied Geography: Marco Vizzarialexandra mp100% (1)
- Parliamentary Election Impact W14299-PDF-ENGDocument8 pagesParliamentary Election Impact W14299-PDF-ENGHarshit ShubhankarNo ratings yet
- Review Notes FinalDocument12 pagesReview Notes FinalJoseph AbalosNo ratings yet
- RELEJI ZA Volkswagen Passat B3 PDFDocument4 pagesRELEJI ZA Volkswagen Passat B3 PDFBorisNo ratings yet
- Social Media Strategy TemplateDocument11 pagesSocial Media Strategy TemplateCall Central USA ITNo ratings yet
- KHKJHKDocument8 pagesKHKJHKMD. Naimul Isalm ShovonNo ratings yet
- Ann Charlton - Steamy DecemberDocument203 pagesAnn Charlton - Steamy Decembershrutigarodia95% (22)
- Pr1 CP Mathandscigr11Document65 pagesPr1 CP Mathandscigr11AllyNo ratings yet
- Quick Locator Guide Controllers / Machine Room: SeesincDocument11 pagesQuick Locator Guide Controllers / Machine Room: SeesincFelipe VillegasNo ratings yet
- Long Slot Array For Wireless Power Transmission: Mauro Ettorre, Waleed A. Alomar, Anthony GrbicDocument2 pagesLong Slot Array For Wireless Power Transmission: Mauro Ettorre, Waleed A. Alomar, Anthony GrbichosseinNo ratings yet
- 1964 1obli ChronicleDocument12 pages1964 1obli Chronicleapi-198872914No ratings yet
- CNC - How To Build A - Router Part 1, 2 and 3 PDFDocument11 pagesCNC - How To Build A - Router Part 1, 2 and 3 PDFfjagorNo ratings yet
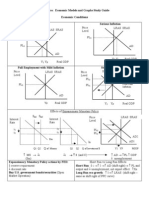
- AP Macroeconomic Models and Graphs Study GuideDocument23 pagesAP Macroeconomic Models and Graphs Study GuideAznAlexT90% (21)
- Dwnload Full Introduction To Environmental Geology 5th Edition Keller Test Bank PDFDocument35 pagesDwnload Full Introduction To Environmental Geology 5th Edition Keller Test Bank PDFgilmadelaurentis100% (12)
- Basic Ecological Concepts and PrinciplesDocument12 pagesBasic Ecological Concepts and PrinciplesShamira Yessa Lazaro Espinosa100% (3)