You might also like
- Nurturing with Nutrition: Everything You Need to Know About Feeding Infants and ToddlersFrom EverandNurturing with Nutrition: Everything You Need to Know About Feeding Infants and ToddlersNo ratings yet
- Issues of Maternal and Child Health NursingDocument31 pagesIssues of Maternal and Child Health NursingAnonymous XK9fWOhxNo ratings yet
- Navigating Parenthood's Greatest Challenges with Grace and GrowthFrom EverandNavigating Parenthood's Greatest Challenges with Grace and GrowthNo ratings yet
- Issues of Maternal and Child Health NursingDocument12 pagesIssues of Maternal and Child Health Nursingcitidotnet87% (31)
- Promoting Responsive Feeding During Breastfeeding, Bottle-Feeding, and the Introduction to Solid FoodsFrom EverandPromoting Responsive Feeding During Breastfeeding, Bottle-Feeding, and the Introduction to Solid FoodsNo ratings yet
- When Your Child Won’T Eat or Eats Too Much: A Parents’ Guide for the Prevention and Treatment of Feeding Problems in Young ChildrenFrom EverandWhen Your Child Won’T Eat or Eats Too Much: A Parents’ Guide for the Prevention and Treatment of Feeding Problems in Young ChildrenNo ratings yet
- Preventive ObstetricDocument12 pagesPreventive ObstetricRicha KohliNo ratings yet
- Teach Children About Nutrition: The Most Common Nutrition Myths and Real Nutritional Needs for Children: The Master Parenting Series, #10From EverandTeach Children About Nutrition: The Most Common Nutrition Myths and Real Nutritional Needs for Children: The Master Parenting Series, #10No ratings yet
- Rethinking Nutrition: Connecting Science and Practice in Early Childhood SettingsFrom EverandRethinking Nutrition: Connecting Science and Practice in Early Childhood SettingsNo ratings yet
- Healthy Child, Whole Child: Integrating the Best of Conventional and Alternative Medicine to Keep Your Kids HealthyFrom EverandHealthy Child, Whole Child: Integrating the Best of Conventional and Alternative Medicine to Keep Your Kids HealthyRating: 1 out of 5 stars1/5 (1)
- Super Nutrition for Babies: The Right Way to Feed Your Baby for Optimal HealthFrom EverandSuper Nutrition for Babies: The Right Way to Feed Your Baby for Optimal HealthNo ratings yet
- Transcultural Nursing Across The Life Span: Ma. Flossie L. TangpuzDocument23 pagesTranscultural Nursing Across The Life Span: Ma. Flossie L. TangpuzSheila VerbaNo ratings yet
- B. P. Koirala Institute of Health Sciences College of Nursing Dharan, Sunsari, NepalDocument5 pagesB. P. Koirala Institute of Health Sciences College of Nursing Dharan, Sunsari, NepalBhagwati PandeyNo ratings yet
- Culturally Competent Childbearing CareDocument6 pagesCulturally Competent Childbearing CareSeika SouiNo ratings yet
- The CALM Baby Method: Solutions for Fussy Days and Sleepless NightsFrom EverandThe CALM Baby Method: Solutions for Fussy Days and Sleepless NightsNo ratings yet
- Breaking Free: Overcoming Anorexia and Body Image DistortionFrom EverandBreaking Free: Overcoming Anorexia and Body Image DistortionNo ratings yet
- Trans CulturalDocument6 pagesTrans CulturalAlyssa Santos JavierNo ratings yet
- Healthy Kids, Happy Moms: 7 Steps to Heal and Prevent Common Childhood IllnessesFrom EverandHealthy Kids, Happy Moms: 7 Steps to Heal and Prevent Common Childhood IllnessesNo ratings yet
- When Your Child Hates Food: Parent’s Practical Guide to Help Kids Overcome Eating Disorder (Anorexia)From EverandWhen Your Child Hates Food: Parent’s Practical Guide to Help Kids Overcome Eating Disorder (Anorexia)Rating: 5 out of 5 stars5/5 (1)
- The Wholesome Child: A Nutrition Guide with More Than 140 Family-Friendly RecipesFrom EverandThe Wholesome Child: A Nutrition Guide with More Than 140 Family-Friendly RecipesNo ratings yet
- The Importance of Nutrition Literacy: Understanding the Importance Behind Nutrition EducationFrom EverandThe Importance of Nutrition Literacy: Understanding the Importance Behind Nutrition EducationNo ratings yet
- Journal FormatDocument2 pagesJournal FormatJescel Angel Jade B LandinginNo ratings yet
- Cultural Influences on Childbearing PerspectivesDocument9 pagesCultural Influences on Childbearing PerspectivesDan Dan ManaoisNo ratings yet
- A Caregivers Plan for Caring for Children & Adults with Special Needs: Navigating Special Needs CareFrom EverandA Caregivers Plan for Caring for Children & Adults with Special Needs: Navigating Special Needs CareNo ratings yet
- Family Nutrition GuideFrom EverandFamily Nutrition GuideNo ratings yet
- The Clean-Eating Kid: Grocery Store Food Swaps for an Anti-Inflammatory DietFrom EverandThe Clean-Eating Kid: Grocery Store Food Swaps for an Anti-Inflammatory DietNo ratings yet
- The Complete Guide to Nursing and Interview Questions and AnswersFrom EverandThe Complete Guide to Nursing and Interview Questions and AnswersNo ratings yet
- The Preemie Parents' Companion: The Essential Guide to Caring for Your Premature Baby in the Hospital, at Home, and Through the First YearsFrom EverandThe Preemie Parents' Companion: The Essential Guide to Caring for Your Premature Baby in the Hospital, at Home, and Through the First YearsNo ratings yet
- Practical 11 Health Education: 11 0 ObjectivesDocument10 pagesPractical 11 Health Education: 11 0 ObjectivesÑàgùr BåshaNo ratings yet
- Aging Well: Solutions to the Most Pressing Global Challenges of AgingFrom EverandAging Well: Solutions to the Most Pressing Global Challenges of AgingNo ratings yet
- Rehabit Your Life: A Doctor’s Notebook on Navigating Health & Well-beingFrom EverandRehabit Your Life: A Doctor’s Notebook on Navigating Health & Well-beingNo ratings yet
- The Blocked Milk Ducts Mastery Bible: Your Blueprint for Complete Blocked Milk Ducts ManagementFrom EverandThe Blocked Milk Ducts Mastery Bible: Your Blueprint for Complete Blocked Milk Ducts ManagementNo ratings yet
- The Nourishing Traditions Book of Baby & Child CareFrom EverandThe Nourishing Traditions Book of Baby & Child CareRating: 4.5 out of 5 stars4.5/5 (14)
- Conversations with My Daughter - How to Have a Healthy Baby:: How to Have a Healthy BabyFrom EverandConversations with My Daughter - How to Have a Healthy Baby:: How to Have a Healthy BabyNo ratings yet
- Introduction, Concept of Child CareDocument42 pagesIntroduction, Concept of Child CareArchana80% (5)
- Well-Child Care in Infancy: Promoting Readiness for LifeFrom EverandWell-Child Care in Infancy: Promoting Readiness for LifeNo ratings yet
- Camarines Sur Polythenic CollegesDocument4 pagesCamarines Sur Polythenic CollegesleahraizaNo ratings yet
- Parenting a Child with Eating Disorder: A Comprehensive Guide to Parenting a Child with Eating Disorder and Building ResilienceFrom EverandParenting a Child with Eating Disorder: A Comprehensive Guide to Parenting a Child with Eating Disorder and Building ResilienceNo ratings yet
- Reimagine Well Learn Guide: Palliative Care: A Holistic Approach to Life-Limiting DiseaseFrom EverandReimagine Well Learn Guide: Palliative Care: A Holistic Approach to Life-Limiting DiseaseNo ratings yet
- Framework For Maternal and Child Health NursingDocument18 pagesFramework For Maternal and Child Health NursingTrisha ApalisNo ratings yet
- Ncm107mch Module1 FrameworkDocument30 pagesNcm107mch Module1 FrameworkVenus Anne LamayoNo ratings yet
- Family Life EducationDocument6 pagesFamily Life EducationKALAI AKSHAYANo ratings yet
- Remembering 2020: Year of the Most Memorable National ChallengesFrom EverandRemembering 2020: Year of the Most Memorable National ChallengesNo ratings yet
- Maternal BookDocument54 pagesMaternal Bookpaulriqs100% (3)
- The Nutrient-Dense Eating Plan: A Lifetime Eating Guide to Exceptional Foods for Super HealthFrom EverandThe Nutrient-Dense Eating Plan: A Lifetime Eating Guide to Exceptional Foods for Super HealthNo ratings yet
- Family Child Health Nursing: Deborah Padgett CoehloDocument46 pagesFamily Child Health Nursing: Deborah Padgett CoehloFahri GunawanNo ratings yet
- Building Bridges A Parent's Road to Inclusive Education for Special Needs ChildrenFrom EverandBuilding Bridges A Parent's Road to Inclusive Education for Special Needs ChildrenNo ratings yet
- A Healthy Baby's Diet and Care: Feeding and Traditional Care for Your Baby During The First Year of Its LifeFrom EverandA Healthy Baby's Diet and Care: Feeding and Traditional Care for Your Baby During The First Year of Its LifeNo ratings yet
- The Postnatal Cookbook: Simple and Nutritious Recipes to Nourish Your Body and Spirit During the Fourth TrimesterFrom EverandThe Postnatal Cookbook: Simple and Nutritious Recipes to Nourish Your Body and Spirit During the Fourth TrimesterNo ratings yet
- Answer Pharma Case Study Week 1Document2 pagesAnswer Pharma Case Study Week 1Threcia RotaNo ratings yet
- Maintaining Homeostasis and the Autonomic Nervous SystemDocument30 pagesMaintaining Homeostasis and the Autonomic Nervous SystemThrecia RotaNo ratings yet
- Drugs Affecting Reproductive & Cardiovascular SystemsDocument27 pagesDrugs Affecting Reproductive & Cardiovascular SystemsThrecia RotaNo ratings yet
- Nursing Assessment in Family Nursing PracticeDocument2 pagesNursing Assessment in Family Nursing PracticeThrecia RotaNo ratings yet
- Nursing Problems TypologyDocument8 pagesNursing Problems TypologyClifford Ogad0% (1)
- RE: Schedule of Finance Collection and Signing of ClearanceDocument1 pageRE: Schedule of Finance Collection and Signing of ClearanceThrecia RotaNo ratings yet
- Reviewed Cervical Polyps CS UnfinishedDocument20 pagesReviewed Cervical Polyps CS UnfinishedThrecia RotaNo ratings yet
- St. Mary's College Bachelor of Science in NursingDocument21 pagesSt. Mary's College Bachelor of Science in NursingThrecia RotaNo ratings yet
- Week 1b TaskDocument1 pageWeek 1b TaskThrecia RotaNo ratings yet
- Grade 11 ABM COMED 422 Transmuted GradesDocument4 pagesGrade 11 ABM COMED 422 Transmuted GradesThrecia RotaNo ratings yet
- Unit 5 Swimming Rules & Regulations, and Basic Live-Saving Skill & SwimmingDocument14 pagesUnit 5 Swimming Rules & Regulations, and Basic Live-Saving Skill & SwimmingThrecia RotaNo ratings yet
- Answer Pharma Case Study Week 1Document2 pagesAnswer Pharma Case Study Week 1Threcia RotaNo ratings yet
- GROWTH and DEVELOPMENTDocument38 pagesGROWTH and DEVELOPMENTThrecia RotaNo ratings yet
- 11 4 Calibo PDFDocument34 pages11 4 Calibo PDFnelmaNo ratings yet
- Contraindications: DRUG STUDY: MetronidazoleDocument1 pageContraindications: DRUG STUDY: MetronidazoleKimberly OlarteNo ratings yet
- Grades Name 1St Q 2Ndq 3Rdq 4ThqDocument32 pagesGrades Name 1St Q 2Ndq 3Rdq 4ThqThrecia RotaNo ratings yet
- Basic Drug Calculation Formula LessonDocument20 pagesBasic Drug Calculation Formula LessonThrecia RotaNo ratings yet
- Republic of The Philippines Department of Trade and Industry Business Name Registration Sole Proprietorship Application FormDocument4 pagesRepublic of The Philippines Department of Trade and Industry Business Name Registration Sole Proprietorship Application FormJaime GonzalesNo ratings yet
- Bataan Action Plan On SBFPDocument3 pagesBataan Action Plan On SBFPNCabredoRegina100% (2)
- ACC 211 SIM Week 6 7Document40 pagesACC 211 SIM Week 6 7Threcia Rota50% (2)
- ACC 214L 1st Practical ExamDocument6 pagesACC 214L 1st Practical ExamThrecia RotaNo ratings yet
- EZ Computer Shop Customer Balance Detail ReportDocument2 pagesEZ Computer Shop Customer Balance Detail ReportThrecia RotaNo ratings yet
- Register Sole Proprietorship Business Name PhilippinesDocument7 pagesRegister Sole Proprietorship Business Name PhilippinesThrecia RotaNo ratings yet
- Activity 4Document1 pageActivity 4Threcia RotaNo ratings yet
- Register Sole Proprietorship Business Name PhilippinesDocument7 pagesRegister Sole Proprietorship Business Name PhilippinesThrecia RotaNo ratings yet
- Planting (NSTP)Document2 pagesPlanting (NSTP)Threcia RotaNo ratings yet
- Template - MET 01 ANSWER SHEETDocument4 pagesTemplate - MET 01 ANSWER SHEETThrecia RotaNo ratings yet
- Met 01Document2 pagesMet 01Threcia RotaNo ratings yet
- Rasos Nav3Document1 pageRasos Nav3Threcia RotaNo ratings yet
- Management of LabourDocument38 pagesManagement of LabourAnjali Rahul AjmeriNo ratings yet
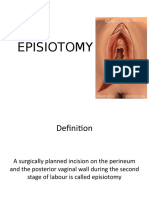
- EPISIOTOMY FinalDocument30 pagesEPISIOTOMY FinalBindu PhilipNo ratings yet
- Essential Intrapartum and Newborn Care Practice Session ChecklistDocument28 pagesEssential Intrapartum and Newborn Care Practice Session ChecklistMonica Melchor DoriaNo ratings yet
- Ncma217 Lec Week10 ModuleDocument10 pagesNcma217 Lec Week10 ModuleABEGAIL BALLORANNo ratings yet
- Cesarean Section CaseStudyDocument23 pagesCesarean Section CaseStudyDada Malicsi LandichoNo ratings yet
- EpisiorrhaphyDocument20 pagesEpisiorrhaphyAhmed Ben BellaNo ratings yet
- Perineal RuptureDocument24 pagesPerineal RuptureIzz ShuhaimiNo ratings yet
- Jurnal Rupture Perineum 5Document5 pagesJurnal Rupture Perineum 5Muh AqwilNo ratings yet
- 13 Genital Tract InjuriesDocument100 pages13 Genital Tract InjuriesRana Vandana100% (1)
- Postpartum case studyDocument3 pagesPostpartum case studyDwaine TolentinoNo ratings yet
- VacumDocument16 pagesVacumGkpmi Ekklesia JayapuraNo ratings yet
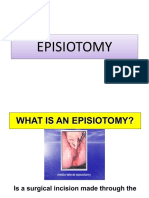
- Episiotomy PDFDocument15 pagesEpisiotomy PDFNabighah ZukriNo ratings yet
- Mother Friendly Care PracticesDocument67 pagesMother Friendly Care PracticesSeth Josiah E. MacalaladNo ratings yet
- Vacuum DeliveryDocument31 pagesVacuum DeliveryAparna LaxmanNo ratings yet
- Wits Obstetrics 2008Document134 pagesWits Obstetrics 2008Muvenn Kannan100% (1)
- Nursing Care of The Family During The Postpartum PeriodDocument13 pagesNursing Care of The Family During The Postpartum PeriodGladys YaresNo ratings yet
- Labor Stage II (Expulsion)Document15 pagesLabor Stage II (Expulsion)nursereview100% (7)
- GCPDocument89 pagesGCPmaria apolonia mancaoNo ratings yet
- Obs & Gynae InstrumentsDocument66 pagesObs & Gynae InstrumentsEng AbdiRahim Khalif Ali71% (7)
- Teves, J. Owen NCP Risk For Infection R:T Episiotomy WoundDocument3 pagesTeves, J. Owen NCP Risk For Infection R:T Episiotomy WoundJoi Owen Teves100% (1)
- 51 EpisiotomyDocument21 pages51 Episiotomydr_asaleh100% (2)
- PGD 5 AnswersDocument14 pagesPGD 5 AnswersDianeNo ratings yet
- Journal Reading DELIVERY ROOMDocument16 pagesJournal Reading DELIVERY ROOMShyenNo ratings yet
- Business Communication Building Critical Skills 6th Edition Locker Test BankDocument34 pagesBusiness Communication Building Critical Skills 6th Edition Locker Test Bankrubepazuqo88% (8)
- Postpartum CareDocument56 pagesPostpartum CareJan Oliver YaresNo ratings yet
- Evidence-Based Practices For Safe & Quality Care of Birthing Mothers & Their NewbornsDocument15 pagesEvidence-Based Practices For Safe & Quality Care of Birthing Mothers & Their NewbornsLore Anne Mhae SantosNo ratings yet
- EPISIOTOMY: Mediolateral TechniqueDocument27 pagesEPISIOTOMY: Mediolateral TechniqueRaluca HabaNo ratings yet
- ALL Ob-Gyn MCQS: Compiled and Edited byDocument297 pagesALL Ob-Gyn MCQS: Compiled and Edited byTianah davis100% (1)
- CPG On Normal Labor and DeliveryDocument59 pagesCPG On Normal Labor and DeliveryHedy Suico Galela - Racines100% (2)
- Postpartum Care GuideDocument10 pagesPostpartum Care GuideKelvin KurtNo ratings yet