You might also like
- Health Sector StrategyDocument11 pagesHealth Sector StrategyRaymunda Rauto-avilaNo ratings yet
- Health Care Delivery System (Reviewer)Document4 pagesHealth Care Delivery System (Reviewer)JOEL VINCENT PURUGGANANNo ratings yet
- Communication With Other Healthcare ProfessionalsDocument16 pagesCommunication With Other Healthcare ProfessionalsSittie Fahieda Aloyodan100% (1)
- Unit 3-Health Promotion and DiversityDocument37 pagesUnit 3-Health Promotion and DiversityKrista KloseNo ratings yet
- Singapore Vs Taiwan HealthcareDocument3 pagesSingapore Vs Taiwan HealthcareCrystal ChiaNo ratings yet
- Far Eastern University - Dr. Nicanor Reyes Medical FoundationDocument30 pagesFar Eastern University - Dr. Nicanor Reyes Medical FoundationJulia Cabingao100% (1)
- Health System Delivery in BangladeshDocument50 pagesHealth System Delivery in BangladeshDip Ayan MNo ratings yet
- 1 W2 Healthcare System 2Document64 pages1 W2 Healthcare System 292vsmzv6t2No ratings yet
- This Study Resource WasDocument8 pagesThis Study Resource WasMae Ann BusicoNo ratings yet
- CH 3 Health Care Delivery SystemDocument18 pagesCH 3 Health Care Delivery SystemMOHAMMAD BORENENo ratings yet
- Health System - His - LecDocument5 pagesHealth System - His - LecBea Princess AletaNo ratings yet
- An Approach To Addressing Governance From A Health System Framework PerspectiveDocument11 pagesAn Approach To Addressing Governance From A Health System Framework PerspectiveDebashree GogoiNo ratings yet
- Ao 2022 OmnibusDocument13 pagesAo 2022 OmnibusZandra Lyn AlundayNo ratings yet
- 1 Health System Key Components PDFDocument2 pages1 Health System Key Components PDFAbi El CakepNo ratings yet
- LecDocument7 pagesLecJoseph MadlangbayanNo ratings yet
- Far Eastern University - Dr. Nicanor Reyes Medical FoundationDocument30 pagesFar Eastern University - Dr. Nicanor Reyes Medical FoundationJulia CabingaoNo ratings yet
- Improving Health in Saudi Arabia: Through Population Health ManagementDocument27 pagesImproving Health in Saudi Arabia: Through Population Health Managementiyad.alsabiNo ratings yet
- CHN MidtermDocument12 pagesCHN MidtermalicantemaryroselNo ratings yet
- Midterm ReviewerDocument62 pagesMidterm Reviewerchelseabalbarona102No ratings yet
- Health Systems Strengthening: Brief)Document2 pagesHealth Systems Strengthening: Brief)MusaNo ratings yet
- Health FinancingDocument10 pagesHealth FinancingoskraraujoNo ratings yet
- Chapter IiiDocument12 pagesChapter IiiMica-Ella CasasolaNo ratings yet
- BRIEF 3 - What Are The Key Behaviors For Governance of Health Systems V3Document13 pagesBRIEF 3 - What Are The Key Behaviors For Governance of Health Systems V3Souheil DamajNo ratings yet
- Health SystemDocument7 pagesHealth SystemkatieminnixNo ratings yet
- Healthy Life ExceptionDocument4 pagesHealthy Life ExceptionZahid Nawaz KhanNo ratings yet
- Australias Health System 2016Document13 pagesAustralias Health System 2016TuigenNo ratings yet
- T C M I H: Owards A Anadian Odel OF Ntegrated EalthcareDocument23 pagesT C M I H: Owards A Anadian Odel OF Ntegrated EalthcaredocbkNo ratings yet
- Managing Healthcare OrganisationsDocument16 pagesManaging Healthcare OrganisationsSamuel Josafat Olam100% (1)
- RP248 Health Systems, Management, and Organization in Low-And Middle Income CountriesDocument15 pagesRP248 Health Systems, Management, and Organization in Low-And Middle Income CountriesBoyIPNo ratings yet
- HEPO Framework Strategy DOH-Administrative-Order-No-2020-0042Document6 pagesHEPO Framework Strategy DOH-Administrative-Order-No-2020-0042Nicole RocamoraNo ratings yet
- Brochure Department of HealthDocument2 pagesBrochure Department of HealthMaica MedranoNo ratings yet
- Economic Issues in Health Planning and PolicyDocument4 pagesEconomic Issues in Health Planning and PolicyPrashanth ThotaNo ratings yet
- ID Sistem Pelayanan Kesehatan Puskesmas AkeDocument10 pagesID Sistem Pelayanan Kesehatan Puskesmas AkeSeno Atau OsinNo ratings yet
- Health Promotion PolicyDocument12 pagesHealth Promotion PolicyLalita A/P AnbarasenNo ratings yet
- Ao2020 0038Document12 pagesAo2020 0038John Philip TiongcoNo ratings yet
- CHN 2 PrelimsDocument32 pagesCHN 2 PrelimsDarylle Hannah De GuzmanNo ratings yet
- Technical Brief Series - Brief No 8Document3 pagesTechnical Brief Series - Brief No 8gteshomeNo ratings yet
- 3 Health SystemDocument113 pages3 Health SystemHendryNo ratings yet
- Midterm Reviewer in POLGOVDocument16 pagesMidterm Reviewer in POLGOVJam AlindadaNo ratings yet
- Draft UHC Pilot Project ProposalDocument19 pagesDraft UHC Pilot Project ProposalNanditha ChowhanNo ratings yet
- Healthy Public Policy: The Five Major Areas/Strategies in Health Promotion (Ottawa Charter)Document11 pagesHealthy Public Policy: The Five Major Areas/Strategies in Health Promotion (Ottawa Charter)Johnjohn MateoNo ratings yet
- Week 11 - Erwin and BrownsonDocument6 pagesWeek 11 - Erwin and BrownsonDavid FernandezNo ratings yet
- Santosh Kane 2023 Extending Kingdon S Multiple Streams Policy Framework Through An Analysis of How Community HealthDocument16 pagesSantosh Kane 2023 Extending Kingdon S Multiple Streams Policy Framework Through An Analysis of How Community Healthnupurranjan4No ratings yet
- Health Systems 101Document56 pagesHealth Systems 101Hasrah JunaidiNo ratings yet
- Public Relations in The Healthcare Industry: Laurel TraynowiczDocument9 pagesPublic Relations in The Healthcare Industry: Laurel TraynowiczShashwat ShuklaNo ratings yet
- Health Care System (Reviewer)Document3 pagesHealth Care System (Reviewer)JOEL VINCENT PURUGGANANNo ratings yet
- Strengthening Health Systems: Moving Beyond Supporting The Health System: Entering The Third DimensionDocument31 pagesStrengthening Health Systems: Moving Beyond Supporting The Health System: Entering The Third DimensionAngellaNo ratings yet
- HandoutsDocument4 pagesHandoutsyazNo ratings yet
- Leadership and GovernanceDocument22 pagesLeadership and Governancemohit7898No ratings yet
- Comparison of House and Senate Health Reform Bills 11 24 09 - FINALDocument6 pagesComparison of House and Senate Health Reform Bills 11 24 09 - FINALc3colorectalNo ratings yet
- Health Sector Reform HSR in India Vol IDocument121 pagesHealth Sector Reform HSR in India Vol Ibkshukla6669No ratings yet
- HMR 0000000000000154Document13 pagesHMR 0000000000000154Marcelo VelizNo ratings yet
- Role of Institutions in Public Health EducationDocument5 pagesRole of Institutions in Public Health EducationDeepakNo ratings yet
- Guidelines On The Transformationof The Health Promotion and Communication Service (HPCS) To The Health Promotion Bureau (HPB)Document7 pagesGuidelines On The Transformationof The Health Promotion and Communication Service (HPCS) To The Health Promotion Bureau (HPB)Harold Paulo MejiaNo ratings yet
- Institutional Analysis of Health System Governance: Seye Abimbola, Joel Negin, Alexandra L Martiniuk and Stephen JanDocument8 pagesInstitutional Analysis of Health System Governance: Seye Abimbola, Joel Negin, Alexandra L Martiniuk and Stephen JanDr. Kashif HussainNo ratings yet
- Health Services DeliveryDocument13 pagesHealth Services DeliveryRonit ChandNo ratings yet
- WHO StrategyDocument10 pagesWHO StrategyzigxoxNo ratings yet
- How To Do or Not To Do A Benefit Incidence AnalysiDocument10 pagesHow To Do or Not To Do A Benefit Incidence Analysivanyywalters1987No ratings yet
- Collecting and Applying Data On Social Determinants of Health in Health Care SettingsDocument4 pagesCollecting and Applying Data On Social Determinants of Health in Health Care SettingsThienanNo ratings yet
- Is Universal Healthcare Financially Sustainable?: Howard LyonsDocument41 pagesIs Universal Healthcare Financially Sustainable?: Howard Lyonshendra andrianoNo ratings yet
- 13 Universal Health CareDocument2 pages13 Universal Health CareJanelle Ann AntonioNo ratings yet
- The politics of health promotion: Case studies from Denmark and EnglandFrom EverandThe politics of health promotion: Case studies from Denmark and EnglandNo ratings yet
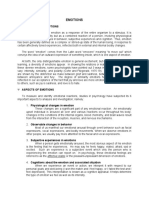
- Emotion SGDocument6 pagesEmotion SGFlint RockNo ratings yet
- AT Transfer-ActivitiesDocument7 pagesAT Transfer-ActivitiesFlint RockNo ratings yet
- CBR Prelims MergedDocument11 pagesCBR Prelims MergedFlint RockNo ratings yet
- Script HNWDocument4 pagesScript HNWFlint RockNo ratings yet
- CBR Midterms: Assessment of Vital Signs Key TermsDocument4 pagesCBR Midterms: Assessment of Vital Signs Key TermsFlint RockNo ratings yet
- CBR Midterms: Assessment of Vital Signs Key TermsDocument4 pagesCBR Midterms: Assessment of Vital Signs Key TermsFlint RockNo ratings yet
- ArtappDocument2 pagesArtappDianne Nicole Gao MurilloNo ratings yet
- Coupling Progress: Explain Importance ComponentsDocument4 pagesCoupling Progress: Explain Importance ComponentsFlint RockNo ratings yet
- Joker Film ReviewDocument1 pageJoker Film ReviewFlint RockNo ratings yet
- Coupling Progress: Explain Importance ComponentsDocument4 pagesCoupling Progress: Explain Importance ComponentsFlint RockNo ratings yet
- Chapter 7 Economic Evaluation of Health ProgramDocument6 pagesChapter 7 Economic Evaluation of Health ProgramSophia AbatayNo ratings yet
- Whodas 2.0Document2 pagesWhodas 2.0Don MashakNo ratings yet
- Ensuring Patient Safety in Dentistry: Denice Stewart, DDS, MHSADocument26 pagesEnsuring Patient Safety in Dentistry: Denice Stewart, DDS, MHSARifka Zahrotun NisaNo ratings yet
- HEALTH CARE Structure in Nigeria-1Document9 pagesHEALTH CARE Structure in Nigeria-1abdulNo ratings yet
- 0-5 Years Child Death Line List HUD: The NilgirisDocument45 pages0-5 Years Child Death Line List HUD: The NilgiristharniNo ratings yet
- HMKP 115 IF00 Transcript 20170308Document1,271 pagesHMKP 115 IF00 Transcript 20170308mokilpoNo ratings yet
- Hospital A Complex EntityDocument4 pagesHospital A Complex EntitySamNo ratings yet
- Auditing Hospital Associated InfectionsDocument59 pagesAuditing Hospital Associated Infectionstummalapalli venkateswara raoNo ratings yet
- Reducing Hospital Readmissions For The ElderlyDocument4 pagesReducing Hospital Readmissions For The ElderlytaniaNo ratings yet
- IRG Health Care ReportDocument57 pagesIRG Health Care ReportAnthony DaBruzziNo ratings yet
- AyusynkDocument2 pagesAyusynknahar570No ratings yet
- ABMAF Heintzeman "Lifeline" Fact CheckDocument4 pagesABMAF Heintzeman "Lifeline" Fact CheckabettermnNo ratings yet
- Directory WilmingtonDocument5 pagesDirectory WilmingtonDaniel RODRIGUEZ SERNANo ratings yet
- Health Disparities BrochureDocument2 pagesHealth Disparities Brochureapi-276375030100% (1)
- Drug Utilization PatternsDocument14 pagesDrug Utilization PatternsEdilma VargasNo ratings yet
- Masterlist Kalendar Kursus NIOSH 2023 - HQ JANUARI - JUN 1Document5 pagesMasterlist Kalendar Kursus NIOSH 2023 - HQ JANUARI - JUN 1zieyzzNo ratings yet
- Friday Problem Statement PresentationDocument7 pagesFriday Problem Statement PresentationyashramawatNo ratings yet
- Are Nyc Health + Hospitals Facilities Located in Community Districts With The Highest Shares of Uninsured New Yorkers?Document1 pageAre Nyc Health + Hospitals Facilities Located in Community Districts With The Highest Shares of Uninsured New Yorkers?ZacharyEJWilliamsNo ratings yet
- Healthcare in PakistanDocument1 pageHealthcare in Pakistanv64wvym7n4100% (1)
- FINAL YOU BrochureDocument16 pagesFINAL YOU BrochureFN2187tNo ratings yet
- Relationship Between Maternal Characteristics and Postpartum Hemorrhage: A Meta-Analysis StudyDocument11 pagesRelationship Between Maternal Characteristics and Postpartum Hemorrhage: A Meta-Analysis Study16.11Hz MusicNo ratings yet
- Practically Perfect Prescribing June 2023 HandoutDocument21 pagesPractically Perfect Prescribing June 2023 HandoutahsanNo ratings yet
- Pschyc Nursing (Assignment#1)Document3 pagesPschyc Nursing (Assignment#1)Nicole Anne TungolNo ratings yet
- WA Health Fees and Charges ManualDocument136 pagesWA Health Fees and Charges ManualFuadNo ratings yet
- Maternal, Child and Adolescent Health Services: Lawrence Ryan A. Daug, RN, MPM CHN 1 - InstructorDocument32 pagesMaternal, Child and Adolescent Health Services: Lawrence Ryan A. Daug, RN, MPM CHN 1 - InstructorLawrence Ryan DaugNo ratings yet
- Gabriel D. Vasilescu 68 Dorchester Road Ronkonkoma, Ny 11779Document3 pagesGabriel D. Vasilescu 68 Dorchester Road Ronkonkoma, Ny 11779Meg Ali AgapiNo ratings yet
- Identify The Role of Infection Prevention and Control in The Work SettingDocument21 pagesIdentify The Role of Infection Prevention and Control in The Work SettingTeenu JobyNo ratings yet
- Intergy EHRDocument2 pagesIntergy EHRMD Solutions, Inc.No ratings yet