You might also like
- 2020 SSC Guidelines For Septic Shock in Children PDFDocument58 pages2020 SSC Guidelines For Septic Shock in Children PDFAtmaSearch Atma JayaNo ratings yet
- Surviving Sepsis Campaign International Guidelines For The Management of Septic Shock and Sepsis Associated Organ Dysfunction in ChildrenDocument58 pagesSurviving Sepsis Campaign International Guidelines For The Management of Septic Shock and Sepsis Associated Organ Dysfunction in ChildrenmarianaglteNo ratings yet
- 2018 Article 1048Document18 pages2018 Article 1048hectorNo ratings yet
- Patient Blood ManagementDocument5 pagesPatient Blood ManagementIndra kusuma mardiaNo ratings yet
- Perit Dial Int 2011 Blake 218 39Document22 pagesPerit Dial Int 2011 Blake 218 39Ika AgustinNo ratings yet
- Literature Review HaemodialysisDocument8 pagesLiterature Review Haemodialysisjvfmdjrif100% (1)
- 2020 Article 642Document9 pages2020 Article 642Anett Pappné LeppNo ratings yet
- 03 Do We Need Other GuidelinesDocument7 pages03 Do We Need Other GuidelinesGold4allNo ratings yet
- American Society of Hematology 2019 Guidelines For Immune ThrombocytopeniaDocument38 pagesAmerican Society of Hematology 2019 Guidelines For Immune ThrombocytopeniaolesyaNo ratings yet
- Itp 2k19 GuidelinesDocument38 pagesItp 2k19 Guidelinesfauzia farhatNo ratings yet
- Septic Shock Carcillo PDFDocument14 pagesSeptic Shock Carcillo PDFjesus_berber_2No ratings yet
- Protocolo RVD Pós TXDocument9 pagesProtocolo RVD Pós TXdiogofc123No ratings yet
- Surviving Sepsis Campaign Guidelines 2021 Highlights For The Practicing ClinicianDocument8 pagesSurviving Sepsis Campaign Guidelines 2021 Highlights For The Practicing ClinicianMariah BrownNo ratings yet
- Seminars in Fetal & Neonatal Medicine: Timur Azhibekov, Sadaf Soleymani, Ben H. Lee, Shahab Noori, Istvan SeriDocument9 pagesSeminars in Fetal & Neonatal Medicine: Timur Azhibekov, Sadaf Soleymani, Ben H. Lee, Shahab Noori, Istvan SeriAyu MarthaNo ratings yet
- Guidelines For Treatment of Septic Shock in ResourDocument21 pagesGuidelines For Treatment of Septic Shock in ResourdintaboiceNo ratings yet
- Peña2020 Article AdolescentPolycysticOvarySyndrDocument16 pagesPeña2020 Article AdolescentPolycysticOvarySyndrpaolaNo ratings yet
- s00134 022 06882 ZDocument18 pagess00134 022 06882 ZEmmanuel Hernandez SantiagoNo ratings yet
- Pediatric Hydrocephalus: Systematic Literature Review and Evidence-Based Guidelines. Part 1: Introduction and MethodologyDocument5 pagesPediatric Hydrocephalus: Systematic Literature Review and Evidence-Based Guidelines. Part 1: Introduction and MethodologyagusNo ratings yet
- 10 1001@jama 2019 0554 PDFDocument15 pages10 1001@jama 2019 0554 PDFFaisal Reza AdiebNo ratings yet
- Article 1Document7 pagesArticle 1gogih64190No ratings yet
- Global Incidence of Necrotizing Enterocolitis A SyDocument15 pagesGlobal Incidence of Necrotizing Enterocolitis A SyJihan AnisaNo ratings yet
- Jama Howell 2017 Gs 170001Document2 pagesJama Howell 2017 Gs 170001Sergio Daniel Chumacero SánchezNo ratings yet
- 2014 12 jns132352Document12 pages2014 12 jns132352Tommy WidjayaNo ratings yet
- Treggiari Miriam M Guidelines For The NeurocriticalDocument28 pagesTreggiari Miriam M Guidelines For The NeurocriticalBelén Fabbrizi100% (1)
- Rehabilitación CardiacaDocument17 pagesRehabilitación Cardiacamsq.cv5919No ratings yet
- Cherukuri Et Al. 2018 - Home Haemodialysis Treatment and Outcomes, Retrospective Analysis of KIHDNEyDocument10 pagesCherukuri Et Al. 2018 - Home Haemodialysis Treatment and Outcomes, Retrospective Analysis of KIHDNEyShareDialysisNo ratings yet
- MousaDocument12 pagesMousaGiriNo ratings yet
- KDIGO 2021 GD Guideline Executive SummaryDocument27 pagesKDIGO 2021 GD Guideline Executive SummaryMahmoud ElsheikhNo ratings yet
- Research Open Access: Singh Et Al. Critical Care (2020) 24:65Document16 pagesResearch Open Access: Singh Et Al. Critical Care (2020) 24:65BrîndușaPetcariuNo ratings yet
- E103 FullDocument10 pagesE103 FullSorin IordacheNo ratings yet
- Abrir Nuevas Guias Hemorragia SubaracnoideaDocument23 pagesAbrir Nuevas Guias Hemorragia SubaracnoideaGustavo Adolfo Nato VázquezNo ratings yet
- E Diabetes CareDocument48 pagesE Diabetes CareRuwan ManjulaNo ratings yet
- Guia Neurocritcal HSA 2023Document28 pagesGuia Neurocritcal HSA 2023Julieta PereyraNo ratings yet
- American Society of ExtraCorporeal Technology - Development of Standards and Guidelines For Pediatric and Congenital Perfusion Practice (2019)Document9 pagesAmerican Society of ExtraCorporeal Technology - Development of Standards and Guidelines For Pediatric and Congenital Perfusion Practice (2019)jq4rhbh2pzNo ratings yet
- Intervention For Myopia in ChildrenDocument5 pagesIntervention For Myopia in Childrennana khrisnaNo ratings yet
- Blake Et Al 2011 Clinical Practice Guidelines and Recommendations On Peritoneal Dialysis Adequacy 2011Document22 pagesBlake Et Al 2011 Clinical Practice Guidelines and Recommendations On Peritoneal Dialysis Adequacy 2011Gema CanalesNo ratings yet
- Survival of Pediatric Patients After CPRDocument11 pagesSurvival of Pediatric Patients After CPRMaria Regina CamargoNo ratings yet
- Management Arteriosclerosis and ClaudicationDocument41 pagesManagement Arteriosclerosis and ClaudicationLuqman AlwiNo ratings yet
- Current Use of Inotropes in Circulatory Shock: Research Open AccessDocument13 pagesCurrent Use of Inotropes in Circulatory Shock: Research Open AccessAli AftabNo ratings yet
- Adequcy of HDDocument22 pagesAdequcy of HDzulfiqarNo ratings yet
- Self-Management Interventions For Adults With Stroke: A Scoping ReviewDocument10 pagesSelf-Management Interventions For Adults With Stroke: A Scoping ReviewFarel LaisyaNo ratings yet
- Literature Review Cardiopulmonary ResuscitationDocument6 pagesLiterature Review Cardiopulmonary Resuscitationaflskkcez100% (1)
- 2001 - ACCP - Management of Spontaneous PneumothoraksDocument13 pages2001 - ACCP - Management of Spontaneous PneumothoraksblueicelandNo ratings yet
- Pediatric Sepsis Guidelines: Summary For Resource-Limited CountriesDocument12 pagesPediatric Sepsis Guidelines: Summary For Resource-Limited CountriesRamya MNo ratings yet
- Standard Operating Procedures (Sops) For Palliative Care in German Comprehensive Cancer Centers - An Evaluation of The Implementation StatusDocument9 pagesStandard Operating Procedures (Sops) For Palliative Care in German Comprehensive Cancer Centers - An Evaluation of The Implementation StatusSujan KhanNo ratings yet
- Surviving Sepsis: Going Beyond The Guidelines: Review Open AccessDocument6 pagesSurviving Sepsis: Going Beyond The Guidelines: Review Open AccessTasya Arsy LiyanaNo ratings yet
- Haspel 2014Document7 pagesHaspel 2014FOURAT OUERGHEMMINo ratings yet
- Common Sense Approach To Managing SepsisDocument12 pagesCommon Sense Approach To Managing SepsiszepedrocorreiaNo ratings yet
- s13054 020 03273 yDocument13 pagess13054 020 03273 yAndi Tiara S. AdamNo ratings yet
- How Can Clinical Epidemiology Better Support Evidence-Based Guidelines and Policies in Low-Income CountriesDocument3 pagesHow Can Clinical Epidemiology Better Support Evidence-Based Guidelines and Policies in Low-Income CountriesEko Wahyu AgustinNo ratings yet
- Self-Monitoring of Blood Pressure Among Women With Hypertensive Disorders of Pregnancy - A SYSTEMATIC REVIEWDocument16 pagesSelf-Monitoring of Blood Pressure Among Women With Hypertensive Disorders of Pregnancy - A SYSTEMATIC REVIEWWeslley FerreiraNo ratings yet
- 2020 Sha CPR GuidelinesDocument132 pages2020 Sha CPR GuidelineschellczyNo ratings yet
- 2022 Article 2728Document24 pages2022 Article 2728Lal NandaniNo ratings yet
- Appraisal: And-Youth-5-17Document1 pageAppraisal: And-Youth-5-17tuio2002No ratings yet
- PBM Frankfurt 2018Document16 pagesPBM Frankfurt 2018Umt TORAXNo ratings yet
- Recommendations From The Guideline For Pcos-NoprintDocument16 pagesRecommendations From The Guideline For Pcos-NoprintpopasorinemilianNo ratings yet
- Arthritis Rheumatology - 2021 - Chung - 2021 American College of Rheumatology Vasculitis Foundation Guideline For TheDocument10 pagesArthritis Rheumatology - 2021 - Chung - 2021 American College of Rheumatology Vasculitis Foundation Guideline For TheDiana RamirezNo ratings yet
- Rectus Diastais Guidelines Full TextDocument14 pagesRectus Diastais Guidelines Full TextlakshitNo ratings yet
- Assessment of Knowledge and Attitude Towards Blood DonationDocument17 pagesAssessment of Knowledge and Attitude Towards Blood DonationbigxNo ratings yet
- CA-BAB TrialDocument7 pagesCA-BAB TrialManju KumariNo ratings yet
- Delayed Versus Immediate Cord Clamping in Preterm Infants: Original ArticleDocument11 pagesDelayed Versus Immediate Cord Clamping in Preterm Infants: Original ArticleManju KumariNo ratings yet
- Antibiotic Stewardship in Premature Infants A Systematic ReviewDocument14 pagesAntibiotic Stewardship in Premature Infants A Systematic ReviewManju KumariNo ratings yet
- Randomized Trial Early or Delayed Enteral Feeding For Preterm Growth-Restricted Infants: ADocument11 pagesRandomized Trial Early or Delayed Enteral Feeding For Preterm Growth-Restricted Infants: AManju KumariNo ratings yet
- Souvenir Book Updated Compressed-1 PDFDocument184 pagesSouvenir Book Updated Compressed-1 PDFManju Kumari100% (1)
- BPD - PROP StudyDocument14 pagesBPD - PROP StudyManju KumariNo ratings yet
- CAP - 11 Year Neurobehavioural OutcomesDocument13 pagesCAP - 11 Year Neurobehavioural OutcomesManju KumariNo ratings yet
- Awaken StudyDocument9 pagesAwaken StudyManju KumariNo ratings yet
- Activity Book For 4-5 Years Children PDFDocument62 pagesActivity Book For 4-5 Years Children PDFAsiyaNaqviNo ratings yet
- The Denver Developmental Screening Test: August, 1967 The Journal o (PEDIATRICS 1 8 1Document11 pagesThe Denver Developmental Screening Test: August, 1967 The Journal o (PEDIATRICS 1 8 1Manju Kumari100% (1)
- Growth and Development PDFDocument1 pageGrowth and Development PDFManju KumariNo ratings yet
- Microcytic Anemia AAP PDFDocument15 pagesMicrocytic Anemia AAP PDFManju KumariNo ratings yet
- European Consensus Guidelines On The Management of Respiratory Distress Syndrome 2019 UpdateDocument19 pagesEuropean Consensus Guidelines On The Management of Respiratory Distress Syndrome 2019 UpdateRodrigo F. RengifoNo ratings yet
- HINE FormDocument4 pagesHINE FormJohannes Purwanto100% (1)
- NNF Guidelines 2011Document344 pagesNNF Guidelines 2011Vijay Dihora0% (1)
- Antibiotic Stewardship in Premature Infants A Systematic ReviewDocument14 pagesAntibiotic Stewardship in Premature Infants A Systematic ReviewManju KumariNo ratings yet
- Apnea de La Prematuridad-439Document7 pagesApnea de La Prematuridad-439Patricia AlonsoNo ratings yet
- Early Developmental Care Interventions of Preterm Very Low Birth Weight InfantsDocument6 pagesEarly Developmental Care Interventions of Preterm Very Low Birth Weight InfantsManju KumariNo ratings yet
- ImmunisationDocument12 pagesImmunisationManju KumariNo ratings yet
- Apnea de La Prematuridad-439Document7 pagesApnea de La Prematuridad-439Patricia AlonsoNo ratings yet
- Microcytic Anemia AAP PDFDocument15 pagesMicrocytic Anemia AAP PDFManju KumariNo ratings yet
- Current Controversies in The Management of Patent Ductus Arteriosus in Preterm InfantsDocument6 pagesCurrent Controversies in The Management of Patent Ductus Arteriosus in Preterm InfantsManju KumariNo ratings yet
- Guidelines Recommendations Child Health PDFDocument38 pagesGuidelines Recommendations Child Health PDFManju KumariNo ratings yet
- LBW, Care & FeedingDocument34 pagesLBW, Care & FeedingManju KumariNo ratings yet
- 4.fluid and ElectrolytesDocument23 pages4.fluid and ElectrolytesManju KumariNo ratings yet
- LBW, Care & FeedingDocument34 pagesLBW, Care & FeedingManju KumariNo ratings yet
- Jurnal Cpap 2Document10 pagesJurnal Cpap 2Febrian AlfaroNo ratings yet
- Magnesium Sulphate (Mgso4) For Fetal Neuroprotection: DR Rajiv KumarDocument16 pagesMagnesium Sulphate (Mgso4) For Fetal Neuroprotection: DR Rajiv KumarManju KumariNo ratings yet
- BleaseGenius MRIDocument2 pagesBleaseGenius MRIHEIDI CASTELLANOSNo ratings yet
- Anesthesia and Myasthenia Gravis2012Document22 pagesAnesthesia and Myasthenia Gravis2012Alisher AgzamovNo ratings yet
- Agh Service CharterDocument75 pagesAgh Service Charternecator samiricanusNo ratings yet
- Human Reproduction QuestionsDocument2 pagesHuman Reproduction Questionsapi-220690063No ratings yet
- Sleep HygieneDocument12 pagesSleep HygieneEmily EresumaNo ratings yet
- E Ticket ReceiptDocument9 pagesE Ticket ReceiptSrinidhi ChandraguthiNo ratings yet
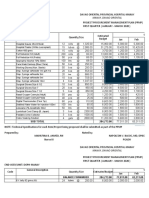
- PPMP Medical Supplies 2020Document16 pagesPPMP Medical Supplies 2020Jan Oneille Y. VallesNo ratings yet
- NABH Standard Document Matrix D125Document18 pagesNABH Standard Document Matrix D125senthilNo ratings yet
- Daftar PustakaDocument2 pagesDaftar PustakaSalwiyadiNo ratings yet
- Neurological EponymsDocument403 pagesNeurological EponymsMario Anderson100% (2)
- Pre-Test Maternal and Child Health NursingDocument18 pagesPre-Test Maternal and Child Health NursingDefensor Pison GringgoNo ratings yet
- Prepare and Administer Parenteral Medications 2Document30 pagesPrepare and Administer Parenteral Medications 2poineNo ratings yet
- AmnesiaDocument2 pagesAmnesiachoc2489No ratings yet
- Thesis TopicsDocument10 pagesThesis TopicsAmithVishalNo ratings yet
- Facial Nerve Palsy in Newborn PeriodDocument5 pagesFacial Nerve Palsy in Newborn PeriodjajNo ratings yet
- 2012 Caribbean V2020 Regional MeetingDocument160 pages2012 Caribbean V2020 Regional Meetingeyecarecaribbean100% (2)
- Low Back Exam PDFDocument2 pagesLow Back Exam PDFDeeea1991No ratings yet
- Transesophageal EchocardiogramDocument3 pagesTransesophageal EchocardiogramsiddharthaNo ratings yet
- Chapter 1 Nov. 24 RevisionDocument12 pagesChapter 1 Nov. 24 RevisionOdessa Fortu LandichoNo ratings yet
- A Guide Benefits of PodiatryDocument20 pagesA Guide Benefits of PodiatryIga AmandaNo ratings yet
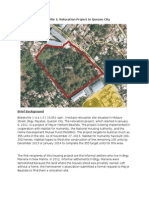
- Bistekville 1: Relocation Project in Quezon CityDocument3 pagesBistekville 1: Relocation Project in Quezon CityJakeNo ratings yet
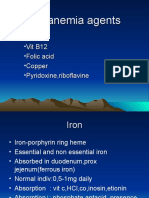
- Obat Anti AnemiaDocument18 pagesObat Anti AnemiaKatate KimekaNo ratings yet
- Data of Doctors in TexasDocument54 pagesData of Doctors in TexasAdnanNo ratings yet
- Care Hospital Bhubaneswar - Doctors, Appointment, Charges, Other DetailsDocument7 pagesCare Hospital Bhubaneswar - Doctors, Appointment, Charges, Other DetailsSubhasish GiriNo ratings yet
- Taking A 12 Lead ECGDocument4 pagesTaking A 12 Lead ECGmadiehahNo ratings yet
- Curricullum Vitae Fajar Agung P OkeDocument3 pagesCurricullum Vitae Fajar Agung P OkeMrprads5No ratings yet
- Surgical Drains 0 PDFDocument3 pagesSurgical Drains 0 PDFawniNo ratings yet
- DS3000 2014Document2 pagesDS3000 2014Francisco TorresNo ratings yet
- Refractory Seizure in Childhood: Dyke-Davidoff-Masson Syndrome RevisitedDocument5 pagesRefractory Seizure in Childhood: Dyke-Davidoff-Masson Syndrome RevisitedaghniajolandaNo ratings yet
- The Cervical & Thoracic Spine Mechanical Diagnosis & Therapy - Vol 1Document313 pagesThe Cervical & Thoracic Spine Mechanical Diagnosis & Therapy - Vol 1Eduardo Batista100% (10)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (80)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (23)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Gut: the new and revised Sunday Times bestsellerFrom EverandGut: the new and revised Sunday Times bestsellerRating: 4 out of 5 stars4/5 (392)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 4 out of 5 stars4/5 (5)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (3)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- 12 Rules for Life by Jordan B. Peterson - Book Summary: An Antidote to ChaosFrom Everand12 Rules for Life by Jordan B. Peterson - Book Summary: An Antidote to ChaosRating: 4.5 out of 5 stars4.5/5 (207)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- Sleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningFrom EverandSleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningRating: 4 out of 5 stars4/5 (3)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisFrom EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisRating: 3.5 out of 5 stars3.5/5 (2)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDFrom EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDRating: 5 out of 5 stars5/5 (1)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)
- An Autobiography of Trauma: A Healing JourneyFrom EverandAn Autobiography of Trauma: A Healing JourneyRating: 5 out of 5 stars5/5 (2)