You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- JURISPRUDENCE (Concept of Liability)Document13 pagesJURISPRUDENCE (Concept of Liability)brijen singh thakur100% (2)
- Notes On Pre-Trial Conference in Criminal CasesDocument2 pagesNotes On Pre-Trial Conference in Criminal CasesJurilBrokaPatiño100% (2)
- Yale - Abnormal Uterine Bleeding Preceptor - 389620 - 284 - 45546 - v1Document12 pagesYale - Abnormal Uterine Bleeding Preceptor - 389620 - 284 - 45546 - v1omegasauron0gmailcomNo ratings yet
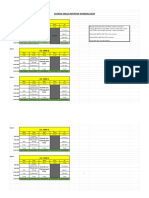
- CSI Schedule 2019-2020Document2 pagesCSI Schedule 2019-2020omegasauron0gmailcomNo ratings yet
- Remediating The Struggling ResidentDocument52 pagesRemediating The Struggling Residentomegasauron0gmailcomNo ratings yet
- Ccu Survival GuideDocument10 pagesCcu Survival Guideomegasauron0gmailcom100% (1)
- Mary Clare Higgins-Chen, MD, MPH Donna Windish, MD, MPH: Alopecia Week 25Document9 pagesMary Clare Higgins-Chen, MD, MPH Donna Windish, MD, MPH: Alopecia Week 25omegasauron0gmailcomNo ratings yet
- EBM Therapy and Diagnosis-Interpretation of Results ExerciseDocument3 pagesEBM Therapy and Diagnosis-Interpretation of Results Exerciseomegasauron0gmailcomNo ratings yet
- Welcome To UNC Hematology/Oncology!Document80 pagesWelcome To UNC Hematology/Oncology!omegasauron0gmailcomNo ratings yet
- AM Curriculum Review-2019-2020Document3 pagesAM Curriculum Review-2019-2020omegasauron0gmailcomNo ratings yet
- Allergy H&PDocument3 pagesAllergy H&Pomegasauron0gmailcomNo ratings yet
- EBM Video TutorialsDocument1 pageEBM Video Tutorialsomegasauron0gmailcomNo ratings yet
- Therapy Article questions-ALLHATDocument2 pagesTherapy Article questions-ALLHATomegasauron0gmailcomNo ratings yet
- Supplemental Guide For Allergy and ImmunologyDocument52 pagesSupplemental Guide For Allergy and Immunologyomegasauron0gmailcomNo ratings yet
- Breast Cancer Screening ResDocument7 pagesBreast Cancer Screening Resomegasauron0gmailcomNo ratings yet
- 186) Estrada V DesiertoDocument3 pages186) Estrada V DesiertoMav EstebanNo ratings yet
- Legal EthicsDocument17 pagesLegal EthicsMagdalena TabaniagNo ratings yet
- Omnibus Rules On Leave: Rule Xvi of The Omnibus Rules Implementing Book V of Eo 292Document2 pagesOmnibus Rules On Leave: Rule Xvi of The Omnibus Rules Implementing Book V of Eo 292Miguel GonzalesNo ratings yet
- Prohibition of Child Marriage ActDocument13 pagesProhibition of Child Marriage ActSatyam PathakNo ratings yet
- Chapter III of Companies Act - Prospectus & Allotment of SecuritiesDocument11 pagesChapter III of Companies Act - Prospectus & Allotment of SecuritiesJohn AllenNo ratings yet
- Carey MTD OrderDocument17 pagesCarey MTD OrderTHROnlineNo ratings yet
- Tracy Jackson v. Continental Bank & Trust Company, Administrator, Estate of Harvey Edwin Serfass, JR., Deceased, 443 F.2d 1344, 10th Cir. (1971)Document10 pagesTracy Jackson v. Continental Bank & Trust Company, Administrator, Estate of Harvey Edwin Serfass, JR., Deceased, 443 F.2d 1344, 10th Cir. (1971)Scribd Government DocsNo ratings yet
- Banasthali VidyapeethDocument7 pagesBanasthali VidyapeethNisha PasariNo ratings yet
- National Investment and Development Corp V Judge Aquino 163 Scra 153Document37 pagesNational Investment and Development Corp V Judge Aquino 163 Scra 153Kaye Miranda LaurenteNo ratings yet
- Umali V ComelecDocument3 pagesUmali V ComelecsashinaNo ratings yet
- Welcome To Braamfontein Improvement District (BID) Now Trading As BraamDocument2 pagesWelcome To Braamfontein Improvement District (BID) Now Trading As BraamGrant FrostNo ratings yet
- CasesDocument37 pagesCasesAlia Arnz-DragonNo ratings yet
- Labor Relations NotesDocument33 pagesLabor Relations NotesGeraldine B. MasiglatNo ratings yet
- Office of The Provincial Prosecutor of Zamboanga Del Norte vs. CADocument13 pagesOffice of The Provincial Prosecutor of Zamboanga Del Norte vs. CAfirmo minoNo ratings yet
- Special Power of AttorneyDocument2 pagesSpecial Power of AttorneyRyan SarabiaNo ratings yet
- (U) Daily Activity Report: Marshall DistrictDocument5 pages(U) Daily Activity Report: Marshall DistrictFauquier NowNo ratings yet
- Rule 16 To 36-1Document8 pagesRule 16 To 36-1DenardConwiBesaNo ratings yet
- Metcalf V Bochco (Copyright)Document5 pagesMetcalf V Bochco (Copyright)gesmerNo ratings yet
- Human Rights, Environmental Rights.Document42 pagesHuman Rights, Environmental Rights.Emmanuel O.100% (2)
- Chapter One. ROBBERY: Against or Intimidation of Persons, Even If The Robbery Was Committed in A Dwelling HouseDocument30 pagesChapter One. ROBBERY: Against or Intimidation of Persons, Even If The Robbery Was Committed in A Dwelling Housemichelle jane reyesNo ratings yet
- 101 103Document6 pages101 103Carlos JamesNo ratings yet
- Republic Vs FelicianoDocument1 pageRepublic Vs FelicianoDanny AnneNo ratings yet
- Habeas CorpusDocument1 pageHabeas CorpusEmanuela PascariNo ratings yet
- Police Operation Part 4Document4 pagesPolice Operation Part 4phic.vtanchulinghospitalNo ratings yet
- Types of PrisonDocument4 pagesTypes of PrisonJayson BauyonNo ratings yet
- DemocracyvauthoritarianDocument9 pagesDemocracyvauthoritarianapi-301535260No ratings yet
- KhiwiDocument23 pagesKhiwiAdeWaleNo ratings yet
- Affidavit of Undertaking For PNP Birth Date - RodriguezDocument1 pageAffidavit of Undertaking For PNP Birth Date - Rodriguezwilson abrasaldoNo ratings yet