Professional Documents
Culture Documents
C M B G T: Avernous Alformations of The Asal Anglia and Halamus
Uploaded by
Zdravko HeinrichOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
C M B G T: Avernous Alformations of The Asal Anglia and Halamus
Uploaded by
Zdravko HeinrichCopyright:
Available Formats
TOPIC REVIEW
Bradley A. Gross, M.D. CAVERNOUS MALFORMATIONS OF THE BASAL
Department of Neurological Surgery,
Feinberg School of Medicine and GANGLIA AND THALAMUS
McGaw Medical Center,
Northwestern University,
Chicago, Illinois, and CAVERNOUS MALFORMATIONS OF the basal ganglia and thalamus present a unique
Division of Neurosurgery,
Evanston Northwestern Healthcare,
therapeutic challenge to the neurosurgeon given their unclear natural history, the risk
Evanston, Illinois of surgical treatment, and the unproven efficacy of radiosurgical therapy. Via a PubMed
search of the English and French literature, we have systematically reviewed the natu-
H. Hunt Batjer, M.D. ral history and surgical and radiosurgical management of these lesions reported through
Department of Neurological Surgery, April 2008. Including rates cited for “deep” cavernous malformations, annual bleeding
Feinberg School of Medicine and
McGaw Medical Center,
rates for these lesions varied from 2.8% to 4.1% in the natural history studies. Across
Northwestern University, surgical series providing postoperative or long-term outcome data on 103 patients, we
Chicago, Illinois, and found an 89% resection rate, a 10% risk of long-term surgical morbidity, and a 1.9%
Division of Neurosurgery,
Evanston Northwestern Healthcare,
risk of surgical mortality. The decrease in hemorrhage risk reported 2 years after radio-
Evanston, Illinois surgery might be a result of natural hemorrhage clustering, underscoring the unproven
efficacy of this therapeutic modality. Given the compounded risks of radiation-induced
Issam A. Awad, M.D. injury and post-radiosurgical rebleeding, radiosurgery at modest dosimetry (12–14 Gy
Department of Neurological Surgery, marginal doses) is only an option for patients with surgically inaccessible, aggressive lesions.
Feinberg School of Medicine and
McGaw Medical Center, KEY WORDS: Angioma, Basal ganglia, Cavernous malformation, Natural history, Radiosurgery, Surgery,
Northwestern University, Surgical approach, Thalamus
Chicago, Illinois, and
Division of Neurosurgery, Neurosurgery 65:7–19, 2009 DOI: 10.1227/01.NEU.0000347009.32480.D8 www.neurosurgery-online.com
Evanston Northwestern Healthcare,
Evanston, Illinois
C
avernous malformations (CMs) are deficits (1, 37, 67), with a particular sensitivity
Bernard R. Bendok, M.D.
clusters of sinusoidal channels filled of highly eloquent tissue to even minor mor-
Department of Neurological Surgery,
Feinberg School of Medicine and
with blood at various stages of evolu- phological changes (67). A prime example is
McGaw Medical Center, tion (54, 55). Vessel walls comprise a flattened CMs of the basal ganglia or thalamus, rela-
Northwestern University, endothelium and a thin fibrous adventitia, tively rare lesions with the potential to cause
Chicago, Illinois, and lacking elastin and smooth muscle (54, 55). significant, devastating neurological deficits
Division of Neurosurgery,
Although these are low-pressure lesions (46), (13, 28, 31, 35, 68, 90). Their rarity has limited
Evanston Northwestern Healthcare,
Evanston, Illinois they are remarkably dynamic with a potential descriptions of their natural history and sur-
to both enlarge and diminish in size (17, 37, gical and radiosurgical management to pri-
Reprint requests: 43, 69). Although the latter is often attributed marily case reports (13, 28, 35, 40, 49, 73, 76,
H. Hunt Batjer, M.D., to hematoma absorption (17, 37), a variety of 82, 90) and larger, broad series (51, 87). This
Department of Neurological Surgery, mechanisms of enlargement have been pro- has obscured the unique challenge these
Feinberg School of Medicine,
Northwestern University,
posed. These include hemosiderin deposition lesions present from a management stand-
676 N. St. Clair Street, with reactive gliosis (69, 82, 95), sinusoidal point. In comprehensively reviewing the nat-
Suite 2210, proliferation (75, 82, 83), neovascularization ural history and surgical and radiosurgical lit-
Chicago, IL 60611. into an environment of local coagulopathy erature on these lesions, we synthesized a
Email: h-batjer@northwestern.edu
(24, 69, 78), recanalization after intraluminal management algorithm while highlighting
thrombosis (78, 91, 97), cystic enlargement via the nuances of particular surgical approaches
Received, June 18, 2008.
osmosis with reactive neocapillary network- and radiosurgical therapy.
Accepted, January 9, 2009.
ing (86), or the activation of angiogenic fac-
Copyright © 2009 by the tors by microhemorrhage (69, 97). Either local PATIENTS AND METHODS
Congress of Neurological Surgeons mass effect from lesion enlargement or
extralesional bleeding can cause neurological A literature search of the PubMed database for
English and French language articles published from
ABBREVIATIONS: CM, cavernous malformation; January 1970 to April 2008 was performed. The
DVA, developmental venous anomaly search terms, “cavernoma,” “cavernous malforma-
tion,” “cavernous angioma,” “basal ganglia,” “thal-
NEUROSURGERY VOLUME 65 | NUMBER 1 | JULY 2009 | 7
GROSS ET AL.
amus,” “deep,” “natural history,” “surgery,” and “radiosurgery” were with the results from Pozzati’s (68) series of thalamic CMs, results in
used. We further reviewed all references provided in our identified an approximate significant long-term morbidity rate of 15% to 33%
articles, incorporating all relevant cited articles. Publications or partic- from deep CM hemorrhage. Overall, natural history studies have
ular patients within our reviewed series without specific postoperative reported annual bleeding rates ranging from 3.1% to 4.1% for deep
or long-term outcome data for CMs of the basal ganglia or thalamus CMs and from 2.82% to 2.9% for CMs of the basal ganglia and thala-
were excluded (53 patients) (24, 50, 51, 53, 57, 60, 87, 97). Because of the mus specifically.
rarity of CMs of the basal ganglia and thalamus, we incorporated case
reports into our analysis of surgical treatment, adding reporter and Clinical Presentation
publication bias but also affording a more comprehensive picture of CMs of the basal ganglia and thalamus traditionally present with
these lesions. contralateral sensorimotor deficits when symptomatic (9, 8, 22, 29, 31,
45, 51, 62, 68). Severe headache (31, 45, 77) and seizures (20, 68, 90,
Natural History 101) are less common presentations. Although any large CM hemor-
The prevalence of CMs has been reported to range from 0.4% to rhage can cause hydrocephalus (28, 35), medial or dorsal thalamic
0.6% across several natural history and autopsy studies (37, 63, 72, 76), lesions abutting the ventricular system intuitively have a greater
with 5% to 17% (average of 9% across natural history studies) occuring probability of causing obstructive hydrocephalus after a bleed (44, 51,
in the basal ganglia or thalamus (1, 11, 37, 41, 59, 67, 72). Prospective 68). Twenty-five percent of thalamic CMs presented with hydro-
natural history studies have reported CM annual bleeding rates rang- cephalus in the series by Pozzati (68); 15% of thalamic CMs in the
ing from 0.7% to 3.1% (41, 59, 67, 72). Whereas lesion size does not seem series by Mathiesen et al. (51) presented with hydrocephalus.
to affect hemorrhage rates (59, 72), female sex (59, 72) and previous Thalamic lesions can also present with hemianopsia (19, 68), thalamic
bleeds (1, 41) have been proposed as risk factors for hemorrhage. pain syndromes (62), or oculomotor paresis as a result of extension
Although not seen in the study by Moriarity et al. (59), the prospective into the mesencephalon (62, 68). Parkinsonism (23) and extrapyrami-
natural history studies of Kondziolka et al. (41) and Aiba et al. (1) dal symptoms have also been reported for CMs of the basal ganglia
demonstrated a significantly increased risk of rebleeding, citing annual and thalamus (2, 10, 13, 21, 30, 42, 87, 99).
rebleed rates of 4.5% and 22.9%, respectively. Variability in rebleeding Several cases of ganglionic lesions causing hemichorea are described
rates may be attributed in part to hemorrhage clustering, a phenome- in the literature (10, 13, 21, 42, 99). In 1 case report in which a patient
non elegantly demonstrated in the study by Barker et al. (6). with hemichorea and a putaminal CM declined surgery, sodium val-
Deep CM location is a controversial risk factor for hemorrhage. proate was effectively used to improve, but not eliminate, the sympto-
Using a rigorous definition of symptomatic extralesional hemorrhage, matology (21). Yakinci et al. (99) reported alleviation of symptoms in a
Moriarity et al. (59) demonstrated no significant difference in hemor- child with a caudostriatal CM and hemichorea with pimozide. Another
rhage rates between superficial and deep lesions. The annual bleeding patient with hemichorea and a caudate CM had complete resolution of
rate for deep lesions in this study was 3.1%. In a prospective study, symptoms after surgical excision (13). The authors proposed a mecha-
Kondziolka et al. (41) also reported no significant effect of location on nism of release phenomena caused by interruption of striatal neurons
hemorrhage rates, citing an overall annual bleeding rate of 2.9% for projecting to the globus pallidus externa. Hidaka et al. (30) proposed a
CMs of the basal ganglia and thalamus. Tew et al. (89) observed 8 similar mechanism to explain hemiballismus caused by a putaminal
patients with CMs of the basal ganglia and thalamus over a mean CM. After biopsy of the lesion, symptoms transiently ceased, poten-
period of 5.1 years. Two patients rebled and 2 patients experienced tially because of interruption of excitatory fibers from the thalamus
progressive neurological deficits. Among patients experiencing hemor- and cortex projecting to the striatum by a postoperative hematoma. As
rhage from a thalamic CM in the study by Pozzati (68), 1 patient the hematoma resolved, symptoms returned.
remained severely disabled, 3 patients had mild nondisabling dysesthe-
sias, and 3 patients recovered, although 2 underwent surgical interven- A B
tion. This study cited a 6.1% annual rebleed rate for thalamic CMs, not-
ing that all rebleeds occurred within 2 years. Aiba et al. (1) reported an
annual rebleed rate of 11% over a mean follow-up period of 6.51 years
for CMs of the basal ganglia and thalamus, citing no significant relation
of lesion location and rebleed rates.
In a retrospective study, Cantu et al. (11) reported an annual bleed-
ing rate of 2.82% for deep hemispheric lesions, significantly greater
than the 1.22% annual rate for lobar CMs in this study. Porter et al.
(67) reported a 4.1% annual hemorrhage rate and a 10.6% annual clin-
ical event rate for deep lesions, a significant contrast to the 0% rate
reported for superficial lesions. Fifteen clinical events occurred in
patients with lesions in the brainstem, whereas 1 occurred in a patient
with a thalamic CM. The sensitivity of highly eloquent parenchyma
in the basal ganglia, thalamus, and brainstem to minor morphologi-
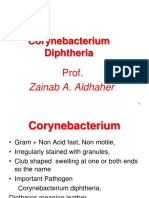
cal changes likely explains the increased aggressiveness of deep CMs FIGURE 1. A, this multiloculated, thalamic cavernous malformation
reported in such studies. In contrast, hemorrhage in a noneloquent (CM) demonstrates the classic appearance of these lesions on T2-
location can go undetected, further inflating relative bleeding rates of weighted imaging: a reticulated mixed signal core with a surrounding
deeper lesions. Importantly, however, Porter et al. reported no signif- hypointense hemosiderin halo. B, after recurrent bleeding, this CM with
icant difference in the degree of recovery between hemorrhagic and ample lateral extension was successfully resected via a distal transsyl-
nonhemorrhagic clinical events (67). Approximately one-third of vian approach.
patients did not improve after a clinical event, which, taken together
8 | VOLUME 65 | NUMBER 1 | JULY 2009 www.neurosurgery-online.com
CAVERNOUS MALFORMATIONS OF THE BASAL GANGLIA AND THALAMUS
TABLE 1. Approaches to cavernous malformations of the basal ganglia and thalamus
Location/approach Comments
Caudate
Interhemispheric transcallosal
Contralateral interhemispheric Added lateral exposure
transcallosal (44, 45)
Transcortical Most direct route
Best used with stereotaxy if hematoma cavity extends close to cortical surface
Risk of postoperative seizures (81) and neuropsychological deficits (14, 96)
Transsylvian For lesions with large hematoma cavities with ample lateral extent
Lentiform
Transsylvian, transinsular Approach of choice
Transcortical Transsulcal with stereotaxy (49) if hematoma cavity extends close to cortical surface
Dorsal/medial thalamus
Interhemispheric transcallosal Risk of forniceal injury
Contralateral interhemispheric Approach of choice
transcallosal (44, 45) Risk of forniceal injury
Added lateral exposure
Transparietal transventricular Potential damage to optic radiations
Added lateral exposure
Posterior thalamus
Occipital interhemispheric subcallosal Wider exposure
Extensive dissection of deep venous system
Supracerebellar infratentorial Dependent on slope of tentorium, limited superior and lateral exposure
Paraculminar supracerebellar infratentorial/ Tentorium can be cut to extend field superolaterally
transtentorial (62)
No need to retract culmen downward
Lateral thalamus/significant lateral
extension of hematoma
Posterior transsylvian transinsular
Dystonia is another less common presentation of both thalamic (68, (62, 87). Two of 9 partially resected lesions rebled, leading to poor out-
87) and ganglionic CMs (2, 49). Akbostanci et al. (2) reported improve- comes in both cases (9, 78). Another partially resected CM regrew,
ment of symptoms with biperiden. Lorenzana et al. (49) reported a requiring reoperation (83).
focal hand dystonia as the exclusive presentation of a lentiform CM. Early postoperative and long-term morbidity is difficult to calculate
Symptoms resolved after surgical excision. The authors proposed dis- given variable surgical selection criteria, outcome reporting, and fol-
ruption of striatopallidothalamic projections to the premotor cortex as low-up. Steinberg et al. (87) reported common transient hemiparesis
the mechanism of the symptomatology. after resection of 15 CMs of the basal ganglia and thalamus. Across our
reviewed surgical series and case reports, 10 of 103 patients (10%) were
Surgical Approaches and Results worse at the time of the long-term follow-up evaluation. Two of 103
After diagnosis of a thalamic or ganglionic CM via its pathogno- patients (1.9%) died from surgery, 1 of them from a postoperative thal-
monic appearance on magnetic resonance imaging (Fig. 1A), surgery is amic infarct after resection of a CM with an associated developmental
often considered for symptomatic patients with aggressive lesions with venous anomaly (DVA) (68).
a noneloquent corridor of access. Surgical approaches are summarized
in Table 1. We have chronologically tabulated results from case reports Caudate CMs
and surgical series reported through June 2008 (Tables 2–5). Fourteen caudate CMs are reviewed in Table 3. Eleven of 12 (92%)
A total of 103 CMs were reviewed. Using data from series provid- were completely resected. Four patients (33%) were worse postopera-
ing specific information on lesion resection rates, 71 of 80 lesions tively, and 1 neonate had moderate mental retardation at the time
(89%) were completely resected. Two recurrences were noted 2 and 8 of follow-up (28). One patient developed debilitating obsessive-
years after radiographically confirmed complete surgical resection compulsive disorder, potentially from frontal deafferentation leading to
NEUROSURGERY VOLUME 65 | NUMBER 1 | JULY 2009 | 9
GROSS ET AL.
TABLE 2. General surgical series and case reports of cavernous malformations of the basal gangliaa
No. of Preoperative Resection Early postoperative
Series (ref. no.) Long-term outcome
patients condition rate morbidity
Aiba et al., 1995 (1) b 5 All bled at least 3 excellent/good;
once 2 moderate disability from
surgery
Attar et al., 2001 (5) 1 HP bled None
Bertalanffy et al., 2002 (8) 8 8/8 No permanent complications
Di Rocco et al., 1996 (20) 2 1 seizure, both bled 2/2 None Both improved/same
Koukkari et al., 1996 (42) 1 Hemichorea No surgical Improved, hemichorea
complicationsc resolved without medication
Lobato et al., 1988 (48) 1 Progressive HP 1/1 Same
Matz et al., 1995 (52) 1 Intact 1/1 Intact
Scott et al., 1992 (78) 1 Symptomatic 1/1 None
Tomlinson et al., 1994 (91) 3 Symptomatic None All with focal deficits and/or
headaches improved
Vaquero et al., 1983 (93) 1 HP 0/1 Same
Winkler et al., 2006 (98) 1 Symptomatic 1/1 Same
Zamorano et al., 1997 (101) 1 Seizures 1/1 Transient HP Improved
Zhao et al., 2007 (102) b 11 11/11 1 transient HP; All improved/same
1 transient facial paresis
a
HP, hemiparesis.
b
Series include both ganglionic and thalamic cavernous malformations.
c
Patient was transiently worse from phenytoin.
dysfunction of frontostriatal loops and a loss of inhibition of automatic plication. Such an approach is generally only considered when the
behavior (90). hematoma cavity closely abuts the sulcus.
The interhemispheric transcallosal approach is the common approach
of choice, given the ability to avoid incising cortex and decreasing the Thalamic CMs
risk of postoperative seizures (81) and neuropsychological deficits (14, Thirty-three thalamic CMs are reviewed in Table 5. Twenty-seven of
96). A contralateral approach adds lateral exposure and may be particu- 33 (82%) were completely resected; 2 lesions recurred at 2 and 8 years
larly attractive for dominant hemisphere lesions (45); it was successfully after ostensibly successful complete surgical resection (62, 87). Thirteen
used for 4 CMs, as shown in Table 2. All were excised completely with- patients (39%) were reported as transiently worse postoperatively, and
out reported complications (3, 45). Although transcortical approaches 2 patients (6%) died from surgery, 1 from a thalamic infarct after resec-
with intraoperative stereotaxy provide a more direct route to the CM, tion of a lesion with an associated DVA (68). Long-term surgical morbid-
they are best used exclusively for lesions with large hematoma cavities ity was observed in 6 patients (18%), attributed to capsular damage in
that allow for minimization of cortical transgression. 2 patients as a result of attempts to remove perilesional gliotic tissue (9).
CMs presenting to the ependymal surface of the dorsal or medial
Lentiform CMs thalamus are best approached via either an ipsilateral or contralateral
Eight lentiform CMs are reviewed in Table 4. All but 1 patient had interhemispheric transcallosal approach. The contralateral transcallosal
a preoperative hemiparesis, making these results less applicable to approach, popularized by Lanzino et al. (44) and Lawton et al. (45), pro-
asymptomatic or minimally symptomatic patients. Overall, 7 of 8 vides added lateral exposure. With the sagittal suture parallel to the
CMs (88%) were completely resected, and 2 of 8 patients (25%) expe- floor, retraction of the lesion-containing hemisphere is facilitated by the
rienced transient worsening of their hemiparesis, although all falx while gravity retracts the contralateral hemisphere downward and
patients were ultimately in improved condition at the time of follow- brings the lesion down into view. The interhemispheric dissection is per-
up. The transsylvian approach with intraoperative stereotaxy is the formed on the contralateral side, an advantage for dominant hemisphere
common approach of choice, with larger hematoma cavities facilitat- lesions. Using this approach, Lawton et al. (45) completely resected 3
ing dissection and minimizing the amount of transgressed cortex. thalamic CMs without complication. A transparietal, transventricular
Additionally, Duffau (22) used subcortical stimulation and somato- approach provides added lateral exposure (7, 68, 77, 89), although it is
topically mapped the internal capsule, noting 4 mm of brain shift. less frequently used and less appealing because of the need for a corti-
Lorenzana et al. (49) described an interesting case of a lentiform CM cal incision and the risk of damage to the optic radiations. Lesions with
presenting exclusively with a focal hand dystonia. The lesion was ample lateral extension of their hematoma cavity may also be removed
resected stereotactically via the second frontal sulcus without com- via a posterior transsylvian approach (19, 39) (Fig. 1).
10 | VOLUME 65 | NUMBER 1 | JULY 2009 www.neurosurgery-online.com
CAVERNOUS MALFORMATIONS OF THE BASAL GANGLIA AND THALAMUS
TABLE 3. Surgical series and case reports of cavernous malformations of the caudate nucleusa
Early
No. of Preoperative Resection Long-term
Series (ref. no.) Approach postoperative
patients condition rate outcome
morbidity
Alves de Sousa, 2007 (3) 3 Contralateral, 3/3 None All in good
interhemispheric condition
transcallosal
Bicknell et al., 1978 (10) 1 Arm monoparesis, 1/1 Same
choreoathetoid
movements
Carpay et al., 1994 (13) 1 Worsening hemichorea Stereotactic, 1/1 None ASx after 0.2 y
deteriorating to transfrontal
hemiballismus
Multiple bleeds
Hashimoto et al., 1997 (28) 1 Neonate 1/1 HCP, VPS Moderate mental
retardation
IPH, IVH 1 seizure
Houtteville, 1995 (31) 2 Both severe HA 1 transparietal 2/2 1 transient Both ASx
leg paresis
Both no focal deficit 1 transsylvian
Both bled
1 SAH
Kerchner et al., 2006 (35) 1 HCP Anterior 1/1 Transient Improved
cognitive
Multiple bleeds Interhemispheric Impairment
Lawton et al., 1996 (45) 1 HA Contralateral anterior 1/1 None
Bled Interhemispheric
Transcallosal
Pozzati et al., 1996 (69) 2 1 seizure Both same/
improved
1 progressive HP
Both bled
Both growing
Stacey et al., 2000 (83) 1 HP, dysphasia 0/1 Regrew Improved
then resected long term
completely
Multiple bleeds
Thobois et al., 2004 (90) 1 Comatose 1/1 Total recovery OCD
R HP Otherwise ASx
a
ASx, asymptomatic; HCP, hydrocephalus; VPS, ventriculoperitoneal shunt; IPH, intraparenchymal hemorrhage; IVH, intraventricular hemorrhage; HA, headache; SAH, subarachnoid
hemorrhage; OCD, obsessive-compulsive disorder; R, right; HP, hemiparesis.
CMs of the posterior thalamus may be approached via an occipital for manual occipital lobe retraction. They successfully removed 1 poste-
interhemispheric subcallosal or supracerebellar infratentorial approach. rior thalamic CM without complication. The occipital interhemispheric
Although the former is encumbered by requisite dissection of the deep approach was specifically described for 3 additional thalamic CMs (Table
galenic venous system, it provides a wider exposure. Chi and Lawton 5) (3, 51, 68). Although 2 patients experienced transient worsening of sen-
(16) noted improved visual outcomes and decreased need for manual sorimotor symptoms, all 3 CMs were completely removed, and all
retraction, less blood loss, and less postoperative edema for patients patients were ultimately in improved condition. Otani et al. (62) used a
positioned laterally (as compared with supine) for posterior interhemi- paraculminar supracerebellar approach with selective tentorial incision
spheric approaches. They attributed this, in part, to the decreased need to give added superolateral exposure in the resection of 6 thalamic CMs.
NEUROSURGERY VOLUME 65 | NUMBER 1 | JULY 2009 | 11
GROSS ET AL.
TABLE 4. Surgical series and case reports of cavernous malformations of the lentiform nucleusa
Early
No. of Preoperative Resection Long-term
Series (ref. no.) Approach postoperative
patients condition rate outcome
morbidity
Duffau, 2000 (22) 1 HP 3 bleeds Stereotactic distal 1/1 Transient Improved
transsylvianb worse HP
Heffez, 1997 (29)c 4 All HP, 3 HS Stereotactic pterional 4/4 1 transient All improved
transsylvian transinsulard worse HP, HS
Kon et al., 2007 (40) 1 HP growing Transsylvian 0/1e Improvedf
Lorenzana et al., 1992 (49) 1 Focal hand Stereotactic via second 1/1 None Improved
dystonia frontal sulcus
Yamasaki et al., 1986 (100) 1 HP, HS bled 1/1 None Improved
a
HP, hemiparesis; HS, hemisensory deficits.
b
Adjunctive subcortical stimulation of internal capsule.
c
Cavernous malformations were described as 0.5 to 2 cm deep to the insular cortex.
d
Adjunctive somatosensory evoked potentials did not change any procedures; however, changes were observed in patients with postoperative hemisensory deficit worsening.
e
Limited by profuse intraoperative bleeding.
f
Underwent postoperative radiotherapy.
This approach averted the need for downward retraction of the culmen. The striking parallel between post-radiosurgical hemorrhage rates
Mild transient morbidity was reported in 2 of 6 patients, and 5 of 6 and the natural history of aggressive CMs further reinforces the need
patients ultimately improved from their preoperative condition. for a prospective, randomized trial of radiosurgery compared with
observation. As mentioned previously, Barker et al. (6) reported a sig-
Radiosurgery nificant decrease in hemorrhage rates after 2 years among aggressive
Radiosurgical treatment of CMs has been regarded with a consider- CMs, and Pozzati (68) reported no rebleeds after 2 years in a smaller
able amount of skepticism (71, 80). Given the known proclivity for series of 12 thalamic CMs. The series by Pozzati (68) and Pozzati et al.
CMs to naturally decrease in size with hematoma resorption (17, 37), (69) and Tung et al. (92) also demonstrated a proclivity toward hemor-
and the lack of imaging modalities to demonstrate lesion obliteration, rhage clustering among aggressive lesions; however, it should be noted
we have relied on post-radiosurgical hemorrhage rates as an indicator that the data from these studies were collected retrospectively.
of radiosurgical efficacy. Although an indirect measure of lesion oblit- In addition to the unclear therapeutic effects of radiosurgery in the
eration, hemorrhage rates more directly reflect clinical outcome. treatment of CMs, multiple series have demonstrated an increased risk
Larger radiosurgical series have reported annual hemorrhage rates of radiation-induced deficits compared with radiosurgery of arteriove-
of 6.3% to 22.4% in the first 2 years after radiosurgery, decreasing to nous malformations (33, 65), potentially from the radiosensitizing
0.8% to 4.5% after this “latency period” (4, 15, 27, 33, 36, 47, 65). The effects of iron and/or radiation of associated DVAs (68, 88).
startling early post-radiosurgical hemorrhage rates were generally Nonetheless, experienced centers have demonstrated waning radio-
comparable or even improved compared with pre-radiosurgical hem- surgical morbidity rates with accumulating experience (27). Across
orrhage rates, underscoring the fact that most radiosurgical data in larger radiosurgical series, radiation-induced early morbidity varied
surgical series is for highly aggressive CMs. However, many lesions widely from 2.5% to 59% (4, 15, 27, 33, 36, 47, 65), likely related to
ultimately underwent surgical resection, deflating reported hemor- operator experience, available imaging and radiosurgical technology,
rhage rates with time (15, 27, 33). and dosimetry (4, 33, 36, 47, 65). In a radiosurgical series of 125 patients
For CMs of the basal ganglia and thalamus in particular, Amin- (14 with CM in the basal ganglia or thalamus), Liu et al. (47) used the
Hanjani et al. (4) demonstrated a notable decrease in annual hemorrhage lowest mean marginal dose (12.1 Gy) and reported the lowest radia-
rate from 16.4% to 2.2% (including the first 2 years) after radiosurgical tion-induced early complication rate of 2.5%.
treatment of 16 lesions. This improvement was markedly better than Among series with specific morbidity data on CMs of the basal gan-
that observed for brainstem CMs in this series. In contrast, Karlsson glia and thalamus, permanent radiation-induced complication rates
et al. (33) reported no significant impact of CM location on hemorrhage have ranged from 0% to 75% (Table 6). In most cases, dosimetry and
rate, reporting an overall post-radiosurgical hemorrhage rate of 11% for follow-up was not specified for this subset of patients, although taken
the first 4 years after radiosurgery decreasing to 6% thereafter. Seven of together, 11 of 50 patients (22%) in these series experienced radiation-
22 CMs in this series were in the basal ganglia or thalamus. Mitchell et al. induced complications that were permanent in 7 of 50 cases (14%).
(58) reported 2 rebleeds after radiosurgical treatment of 7 CMs of the
basal ganglia and thalamus. Across the series by García-Muñoz et al. (25)
(follow-up duration, 6.3 years), Kayali et al. (34) (median follow-up dura- DISCUSSION
tion, 2.5 years), Huang et al. (32) (mean follow-up duration, 5 years), Kim
et al. (38) (mean follow-up duration, 2.5 years), and Stea et al. (85) (mean CMs of the basal ganglia and thalamus present a unique
follow-up duration, 3 years), 0 of 19 CMs of the basal ganglia or thala- therapeutic challenge. In contradistinction to arteriovenous
mus rebled after radiosurgery. malformations of these locations that are oftentimes “reflex-
12 | VOLUME 65 | NUMBER 1 | JULY 2009 www.neurosurgery-online.com
CAVERNOUS MALFORMATIONS OF THE BASAL GANGLIA AND THALAMUS
ively” treated radiosurgically, the neurosurgeon, faced with a Once surgery has been selected, an anatomic (Table 1) or
paucity of information on the natural history and surgical and hematoma-produced surgical approach is selected. DVAs can
radiosurgical treatment of these lesions must often rely on be a particular source of postoperative morbidity and mortal-
anecdotal data and intuition, affording a “best guess.” ity (9, 66, 68). Their benign natural history (0.15%–0.34% symp-
Our review of natural history studies demonstrated an tomatic annual hemorrhage rate) (26, 56, 61), coupled with their
annual bleed risk ranging from 2.8% to 4.1%, with some stud- role in draining normal parenchyma (66, 79), make them an
ies reporting elevated annual rebleed rates of 6.1% to 11% (1, important influence on the selected surgical approach. Their
68), a striking parallel to modern natural history data for arte- disruption must be avoided to prevent potentially fatal venous
riovenous malformations (84). However, these annual bleed infarction (9, 68, 66, 79). Thus, they may contraindicate surgery
and rebleed rates are based on the false assumption of a con- because of their size or if they lie between the requisite corridor
stant, linear risk. They are likely overestimates for initially of access and the lesion. Intraoperative ultrasound is a useful
asymptomatic lesions that are often underrepresented in nat- adjunct to facilitate detection of the DVA (98).
ural history studies. Several reports have demonstrated the Although minimally invasive or endoscopic approaches for
potential benign course deep CMs can follow (12, 68, 69, 73). the successful management of 3 deep CMs have been reported
Thus, we believe that asymptomatic or minimally sympto- (64), we are less inclined to use these, advocating the premise
matic lesions should be observed. Our 10% long-term mor- of “more is more” when it comes to fashioning our craniotomy
bidity rate from surgery comes from the most experienced for deep-seated lesions. Even though CMs are low-flow lesions,
hands operating on primarily symptomatic lesions; it is the potential for intraoperative bleeding, and, more impor-
undoubtedly an underestimate for asymptomatic or minimally tantly, incomplete surgical excision, demand a more generous
symptomatic lesions. We think it outweighs the 15% to 33% exposure. Intraoperative stereotaxy, motor evoked potentials,
risk of significant, long-term morbidity from deep CM hemor- and somatosensory evoked potentials are requisite adjuncts (8,
rhage, should it even occur. 16, 29, 78, 87, 101, 102). We are inclined to account for brain
Conversely, a significant, fixed neurological deficit can serve shift via intraoperative ultrasound (29, 102) or subcortical stim-
as a convincing factor to the patient and surgeon that opera- ulation mapping (22) as opposed to catheter implantation (50).
The potential for intraoperative diffusion-weighted imaging is
tive intervention is less likely to add further disability, but
an exciting area of study that might further reduce potential
may prevent further deterioration from future bleeding. Thus,
surgical morbidity (18). One report of diffusion-weighted imag-
surgical intervention after a single hemorrhage is only a con-
ing used to guide the resection of 4 lesions (including 1 occip-
sideration for patients with: 1) fixed, significant, or progressive
ital CM) in close proximity to the optic radiations demonstrated
neurological deficits, and 2) convincing pial/ependymal rep-
no persistent postoperative visual field deficits (18).
resentation of their CM or hematoma cavity on T1-weighted
Persistently symptomatic lesions that have hemorrhaged twice
imaging. “Bloom effect” leading to overestimation of the prox-
without a surgical corridor of access may undergo radiosurgery
imity of the CM to an accessible surface makes T2-weighted
at modest dosimetry (12–14 Gy to the margin). Notwithstanding
imaging merely an initial, sensitive diagnostic tool for CMs
the confounding factors of natural CM hemorrhage clustering (6)
(87). In Pozzati’s (68) surgical series of 4 thalamic CMs, all
and of selecting patients for surgery after radiotherapy, there
lesions protruded into the lateral ventricle or posterior inci- does seem to be a decrease in rebleed rates after radiosurgery,
sural space. Although we concur with Steinberg et al. (87) that particularly after 2 years (4, 15, 27, 33, 36, 47, 65). However, these
small incisions of the pulvinar portion of the thalamus may be data come from series of predominantly aggressive CMs. It is
tolerated, we are only inclined to perform such incisions with therefore not applicable to minimally symptomatic CMs or those
intraoperative stereotaxy and hemosiderin staining of the sur- that have bled once with stable or improving neurological
face of the thalamus. deficits. These patients should be observed.
After a second clinically significant hemorrhage, the possibil- Our review of radiosurgical series suggests a potentially
ity of further hemorrhage clustering (6, 69) and escalating mor- decreased risk of radiosurgical morbidity for these lesions as
bidity (69, 92) compel us to forego our first inclusion criterion compared with brainstem lesions (4, 27, 85). The overall 14%
for surgery. Two exceptions are patients with multiple lesions risk of permanent morbidity we cite is further compounded by
and those with lentiform CM, given the decreased likelihood of the known risk of rebleeding and its associated morbidity.
surgical cure in the former case and significant risk of postoper- Overall, this modality therefore poses a greater risk of morbid-
ative motor weakness in the latter. As mentioned previously, the ity than surgery for accessible lesions. Thus, it is only an alter-
vast majority of patients with lentiform CM undergoing surgery native to observation for clinically aggressive, surgically inac-
were hemiparetic preoperatively. Similar to Houtteville (31), we cessible lesions, particularly lentiform, capsular, and ventral
are hesitant to operate on patients who have fully recovered thalamic lesions (Fig. 2).
after 2 clinically symptomatic hemorrhages from their lentiform
CM. In addition, given the rarity of mortality from CM hemor- CONCLUSIONS
rhage, the potential benefit of surgery for patients with complete
preoperative motor loss is questionable, even though the risk of Natural history studies of CMs of the basal ganglia and thal-
intervention is seemingly decreased. amus cite annual bleed rates of 2.8% to 4.1%. CMs of the basal
NEUROSURGERY VOLUME 65 | NUMBER 1 | JULY 2009 | 13
GROSS ET AL.
TABLE 5. Surgical series and case reports of cavernous malformations of the thalamusa
Early
No. of Preoperative Resection Long-term
Series (ref. no.) Approach postoperative
patients condition rate outcome
morbidity
Alves de Sousa, 1 Occipital interhemispheric 1/1 Transient HP Good outcome
2007 (3) transventricular
Becker et al., 1 HP, HS Transparietal transventricular 1/1 Transient dysphasia Persistent HP
1979 (7) Bled Incised posteromedial thal
Bertalanffy et al., 2 Both mild HP Anterior interhemispheric 1/2 1 residual Both worse HP
1991 (9) transcallosal rebleed
1 venous infarctb 1 new memory deficit
Bertalanffy et al., 4 1 frontal interhemispheric 4/4 1 long-term memory
2002 (8) transcallosal worsening
3 supracerebellar infratentorial
Chi and Lawton, 1 HP, HS Contralateral interhemispheric 1/1 None mRS 1
2006 (16) occipital transfalcinec
Multiple bleeds
Cohen et al., 1982 (19) 1 HP, HS Posterior transsylvian, 1/1 Thal pain Improving with thal
transinsular syndrome pain syndrome
Hemianopsia
2 bleeds
Houtteville, 1995 (31) 1 Progressive HP, HS Interhemispheric transcallosal 0/1 Asymptomatic
Severe bleed
Kobata et al., 1999 (39) 1 HP Transsylvian (large hematoma) Improved
Multiple bleeds
Lawton et al., 1996 (45) 3 1 HA Contralateral interhemispheric 3/3 None
transcallosal
2 HP, HS
All bled
Mathiesen et al., 1 HP Contralateral transcallosal 1/1 Transient worse Improved
2003 (51)d HP, mutism
Mathiesen et al., 1 Bled twice Occipital interhemispheric 1/1 Transient worse HS Improved
2003 (51)d
Subcallosal transpulvinar
Otani et al., 6 5 oculomotor def Paraculminar supracerebellar 5/6 1 transient 4 improved
2008 (62) infratentorial/transtentorial hemianopsia
4 sensorimotor def 1 transient vertical 1 same
gaze paresis
1 thal pain 1 improved after repeat
syndrome surgery for recurrence
4 bled (3 IVH) 3 independent
2 progressive def
Pannek et al., 3 Retroauricular bur hole with None
1999 (64) stereotaxy with sleeve
Pozzati, 2000 (68) 1 Thal hand, diplopia Occipital interhemispheric subsplenial 1/1 Improved
4 bleeds
Pozzati, 2000 (68)e 3 2 HCP 1 transcallosal 2/3 1 death from thal 1 asymptomatic
infarctf
1 progressive HP, HS 2 transcortical transventricular 1 same
1 dead
Continues
14 | VOLUME 65 | NUMBER 1 | JULY 2009 www.neurosurgery-online.com
CAVERNOUS MALFORMATIONS OF THE BASAL GANGLIA AND THALAMUS
TABLE 5. Continued
Early
No. of Preoperative Resection Long-term
Series (ref. no.) Approach postoperative
patients condition rate outcome
morbidity
Roda et al., 1990 (74) 1 HP Interhemispheric 1/1 New motor aphasia, Worse
worse HP
Bled Transcallosal
Sato and Kubota, 1995 (77) 1 HA Transcortical 1/1 Asymptomatic
Transventricular
Scott et al., 1992 (78) 1 HP Transcallosal 0/1 Worse—III, VII, HP Worse, rebled
Steinberg et al., 2000 (87)g 2 Both HP 1 transcallosal 1/2 Both worse HP Both HP improved
transpulvinar to baseline
1 hemidystonia 1 interhemispheric 1 recurred
transcallosal
1 worse after SRS
Tew et al., 1995 (89) 6 4 transcortical 4 improved
2 transcallosal 1 same
1 worse
Tung et al., 1990 (92) 1 HP, seizure 1/1 Same/improved
4 episodes
Vaquero et al., 1987 (94) 1 Progressive HP, Died Died
dysphasia
Zamorano et al., 1997 (101) 1 Seizures 1/1 None
a
HP, hemiparesis; HS, hemisensory deficit; thal, thalamic; mRS, modified Rankin Scale; HA, headache; def, deficit; IVH, intraventricular hemorrhage; HCP, hydrocephalus;
SRS, stereotactic radiosurgery; III, third nerve palsy; VII, seventh nerve palsy; CM, cavernous malformation.
b
Possible damage to draining vein/developmental venous anomaly.
c
The falx was sectioned; the tentorium was not.
d
This series included a total of 13 CMs of the basal ganglia or thalamus. Our data are from detailed explanations provided for 2 thalamic cases in figure captions. Only patients
with postoperative CM rebleeding had permanent morbidity in this series. Twenty-five of 29 CMs of the basal ganglia, thalamus, or brainstem were completely resected in
this series with a 69% early morbidity rate. At a mean follow-up duration of 4.6 years, 69% of patients were improved, 10% were the same, 17% were worse (mainly from
rebleeding), and 3% were dead.
e
This series provided long-term follow-up data on patients in the earlier report of Pozzati et al. (70).
f
This lesion had an associated developmental venous anomaly.
g
This series included a total of 15 CMs of the basal ganglia or thalamus. Our data are from detailed explanations provided for 2 thalamic cases in figure captions. Fifty-two
of 56 CMs of the basal ganglia, thalamus, or brainstem were completely resected in this series with a 29% early morbidity rate. At a mean follow-up of 4.7 years, 52% of
patients were improved, 43% were the same, and 5% were worse.
TABLE 6. Radiosurgical morbidity rates among series providing data specifically on cavernous malformations of the basal ganglia and thalamusa
Early radiation- Permanent radiation-
Series (ref. no.) No. of patients Radiation source
induced morbidity induced morbidity
Amin-Hanjani et al., 1998 (4) 16 Proton beam 4/16 4/16
Kayali et al., 2004 (34) 5 LA 0/5 0/5
Hasegawa et al., 2002 (27) 13 GK 2/13 0/13
Mitchell et al., 2000 (58) 7 GK 1/7 0/7
Pollock et al., 2000 (65) 4 3/4
Stea et al., 1994 (85) 5 LA 1/5 0/5
a
LA, linear accelerator; GK, gamma knife.
ganglia and thalamus most often present with sensorimotor Across a review of 103 CMs in surgical series, 71 of 80 CMs
deficits. Other, less common presentations include headache, (89%) were documented as completely resected, 10 of 103
hydrocephalus, seizures, and extrapyramidal symptoms. patients (10%) experienced permanent, long-term morbidity
NEUROSURGERY VOLUME 65 | NUMBER 1 | JULY 2009 | 15
GROSS ET AL.
A B
FIGURE 2. A and B, after 3 successive, symptomatic hemorrhages over the Gy in 5 hypofractionated doses (equivalent single marginal dose of approx-
course of 1 year, these 2 thalamic CMs, lacking pial or ependymal represen- imately 12 Gy), this large CM did not demonstrate any further bleeding at
tation, were successfully radiated at moderate dosimetry. A, after radiosur- the time of the 3-year follow-up evaluation. Fractionated radiosurgery was
gical treatment with a marginal dose of 13 Gy, this small, deep thalamic CM used to limit radiation exposure to the hypothalamus and optic pathways.
with a prominent, associated developmental venous anomaly did not demon- Both patients demonstrated near-complete recovery at the time of the most
strate any further bleeding at 2 years’ follow-up. B, after treatment with 20 recent follow-up evaluation.
from surgery, and 2 of 103 patients (1.9%) died as a result of ton beam therapy in 98 cases at the Harvard Cyclotron. Neurosurgery
surgery. These impressive morbidity rates are from experienced 42:1229–1238, 1998.
5. Attar A, Ugur HC, Savas A, Yüceer N, Egemen N: Surgical treatment of
neurosurgeons operating on primarily symptomatic CMs,
intracranial cavernous angiomas. J Clin Neurosci 8:235–239, 2001.
thereby having “less to lose.” 6. Barker FG 2nd, Amin-Hanjani S, Butler WE, Lyons S, Ojemann RG,
Radiosurgery is only an option at modest dosimetry (12–14 Chap man PH, Ogilvy CS: Temporal clustering of hemorrhages from
Gy) for surgically inaccessible, aggressive CMs. An approxi- untreated cavernous malformations of the central nervous system.
mate 14% risk of permanent morbidity from radiation must be Neurosurgery 49:15–25, 2001.
7. Becker DH, Townsend JJ, Kramer RA, Newton TH: Occult cerebrovascular
further compounded to morbidity from rebleeding after radio- malformations. A series of 18 histologically verified cases with negative
surgery, although rebleeding rates seem to decrease, particu- angiography. Brain 102:249–287, 1979.
larly 2 years after treatment. 8. Bertalanffy H, Benes L, Miyazawa T, Alberti O, Siegel AM, Sure U: Cerebral
cavernomas in the adult. Review of the literature and analysis of 72 surgi-
cally treated patients. Neurosurg Rev 25:1–55, 2002.
Disclosure 9. Bertalanffy H, Gilsbach JM, Eggert HR, Seeger W: Microsurgery of deep-
The authors have no personal financial or institutional interest in any of the seated cavernous angiomas: Report of 26 cases. Acta Neurochir (Wien)
drugs, materials, or devices described in this article. 108:91–99, 1991.
10. Bicknell JM, Carlow TJ, Kornfeld M, Stovring J, Turner P: Familial cavernous
angiomas. Arch Neurol 35:746–749, 1978.
REFERENCES 11. Cantu C, Murillo-Bonilla L, Arauz A, Higuera J, Padilla J, Barinagar-
rementeria F: Predictive factors for intracerebral hemorrhage in patients
1. Aiba T, Tanaka R, Koike T, Kameyama S, Takeda N, Komata T: Natural his- with cavernous angiomas. Neurol Res 27:314–318, 2005.
tory of intracranial cavernous malformations. J Neurosurg 83:56–59, 1995. 12. Cappabianca P, Spaziante R, de Divitiis E, Villanacci R: Thalamic cavernous
2. Akbostanci MC, Yiğit A, Ulkatan S: Cavernous angioma presenting with malformations. J Neurosurg 75:169–171, 1991.
hemidystonia. Clin Neurol Neurosurg 100:234–237, 1998. 13. Carpay HA, Arts WF, Kloet A, Hoogland PH, Van Duinen SG: Hemichorea
3. Alves de Sousa A: Deep-seated (corpus callosum, intraventricular, basal reversible after operation in a boy with cavernous angioma in the head of
ganglia and insula) and brain stem cavernous angiomas. Experience in Brazil caudate nucleus. J Neurol Neurosurg Psychiatry 57:1547–1548, 1994.
[in French]. Neurochirurgie 53:182–191, 2007. 14. Carton CA, Hickey WC: Arteriovenous malformation of the head of the
4. Amin-Hanjani S, Ogilvy CS, Candia GJ, Lyons S, Chapman PH: Stereotactic caudate nucleus; report of a case with total removal. J Neurosurg 12:414–418,
radiosurgery for cavernous malformations: Kjellberg’s experience with pro- 1955.
16 | VOLUME 65 | NUMBER 1 | JULY 2009 www.neurosurgery-online.com
CAVERNOUS MALFORMATIONS OF THE BASAL GANGLIA AND THALAMUS
15. Chang SD, Levy RP, Adler JR Jr, Martin DP, Krakovitz PR, Steinberg GK: 39. Kobata H, Kondo A, Iwasaki K, Hattori I: Massive subependymal hemor-
Stereotactic radiosurgery of angiographically occult vascular malformations: rhage caused by an occult vascular malformation—Two case reports. Neurol
14-year experience. Neurosurgery 43:213–221, 1998. Med Chir (Tokyo) 39:302–307, 1999.
16. Chi JH, Lawton MT: Posterior interhemispheric approach: Surgical tech- 40. Kon T, Mori H, Hasegawa K, Nishiyama K, Tanaka R, Takahashi H:
nique, application to vascular lesions, and benefits of gravity retraction. Neonatal cavernous angioma located in the basal ganglia with profuse intra-
Neurosurgery 59 [Suppl 1]:ONS41–ONS49, 2006. operative bleeding. Childs Nerv Syst 23:449–453, 2007.
17. Clatterbuck RE, Moriarity JL, Elmaci I, Lee RR, Breiter SN, Rigamonti D: 41. Kondziolka D, Lunsford LD, Kestle JR: The natural history of cerebral cav-
Dynamic nature of cavernous malformations: A prospective magnetic reso- ernous malformations. J Neurosurg 83:820–824, 1995.
nance imaging study with volumetric analysis. J Neurosurg 93:981–986, 42. Koukkari MW, Vanefsky MA, Steinberg GK, Hahn JS: Phenytoin-related
2000. chorea in children with deep hemispheric vascular malformations. J Child
18. Coenen VA, Huber KK, Krings T, Weidemann J, Gilsbach JM, Rohde V: Neurol 11:490–491, 1996.
Diffusion-weighted imaging-guided resection of intracerebral lesions involv- 43. Labauge P, Brunereau L, Lévy C, Laberge S, Houtteville JP: The natural his-
tory of familial cerebral cavernomas: A retrospective MRI study of 40
ing the optic radiation. Neurosurg Rev 28:188–195, 2005.
patients. Neuroradiology 42:327–332, 2000.
19. Cohen HC, Tucker WS, Humphreys RP, Perrin RJ: Angiographically cryptic
44. Lanzino G, Wanebo JE, Spetzler RF: Contralateral interhemispheric resection
histologically verified cerebrovascular malformations. Neurosurgery 10:704–
of thalamic cavernous malformations with frameless stereotaxy. Oper Tech
714, 1982.
Neurosurg 5:191–197, 2002.
20. Di Rocco C, Iannelli A, Tamburrini G: Cavernomas of the central nervous
45. Lawton MT, Golfinos JG, Spetzler RF: The contralateral transcallosal
system in children. A report of 22 cases. Acta Neurochir (Wien) 138:1267–
approach: Experience with 32 patients. Neurosurgery 39:729–735, 1996.
1274, 1996.
46. Little JR, Awad IA, Jones SC, Ebrahim ZY: Vascular pressures and cortical
21. Donmez B, Cakmur R, Uysal U, Men S: Putaminal cavernous angioma pre-
blood flow in cavernous angioma of the brain. J Neurosurg 73:555–559, 1990.
senting with hemichorea. Mov Disord 19:1379–1380, 2004. 47. Liu KD, Chung WY, Wu HM, Shiau CY, Wang LW, Guo WY, Pan DH:
22. Duffau H: Intraoperative direct subcortical stimulation for identification of Gamma knife surgery for cavernous hemangiomas: An analysis of 125
the internal capsule, combined with an image-guided stereotactic system patients. J Neurosurg 102 [Suppl]:81–86, 2005.
during surgery for basal ganglia lesions. Surg Neurol 53:250–254, 2000. 48. Lobato RD, Perez C, Rivas JJ, Cordobes F: Clinical, radiological, and patho-
23. Ertan S, Benbir G, Tanriverdi T, Alver I, Uzan M: Parkinsonism caused by logical spectrum of angiographically occult intracranial vascular malforma-
cavernoma located in the basal ganglion. Parkinsonism Relat Disord tions. Analysis of 21 cases and review of the literature. J Neurosurg
11:517–519, 2005. 68:518–531, 1988.
24. Frim DM, Scott RM: Management of cavernous malformations in the pedi- 49. Lorenzana L, Cabezudo JM, Porras LF, Polaina M, Rodriguez-Sanchez JA,
atric population. Neurosurg Clin N Am 10:513–518, 1999. Garcia-Yagüe LM: Focal dystonia secondary to cavernous angioma of the
25. García-Muñoz L, Velasco-Campos F, Lujan-Castilla P, Enriquez-Barrera M, basal ganglia: Case report and review of the literature. Neurosurgery
Cervantes-Martínez A, Carrillo-Ruiz J: Radiosurgery in the treatment of 31:1108–1112, 1992.
brain cavernomas. Experience with 17 lesions treated in 15 patients [in 50. Mao Y, Zhou L, Du G, Chen L: Image-guided resection of cerebral cavernous
French]. Neurochirurgie 53:243–250, 2007. malformations. Chin Med J (Engl) 116:1480–1483, 2003.
26. Garner TB, Del Curling O Jr, Kelly DL Jr, Laster DW: The natural history of 51. Mathiesen T, Edner G, Kihlström L: Deep and brainstem cavernomas: A
intracranial venous angiomas. J Neurosurg 75:715–722, 1991. consecutive 8-year series. J Neurosurg 99:31–37, 2003.
27. Hasegawa T, McInerney J, Kondziolka D, Lee JY, Flickinger JC, Lunsford LD: 52. Matz P, McDermott M, Gutin P, Dillon W, Wilson C: Cavernous malforma-
Long-term results after stereotactic radiosurgery for patients with cavernous tions: Results of image-guided resection. J Image Guid Surg 1:273–279, 1995.
malformations. Neurosurgery 50:1190–1198, 2002. 53. Mazza C, Scienza R, Beltramello A, Da Pian R: Cerebral cavernous malfor-
28. Hashimoto H, Sakaki T, Ishida Y, Shimokawara T: Fetal cavernous mations (cavernomas) in the pediatric age-group. Childs Nerv Syst
angioma—Case report. Neurol Med Chir (Tokyo) 37:346–349, 1997. 7:139–146, 1991.
29. Heffez DS: Stereotactic transsylvian transinsular approach for deep-seated 54. McCormick WF: The pathology of vascular (“arteriovenous”) malforma-
lesions. Surg Neurol 48:113–124, 1997. tions. J Neurosurg 24:807–816, 1966.
30. Hidaka M, Shimoda M, Sato O, Watabe T, Tsugane R, Ohsuga H, Araki G: 55. McCormick WF, Nofzinger JD: “Cryptic” vascular malformations of the cen-
Case report: Hemiballism due to a putaminal cavernous hemangioma [in tral nervous system. J Neurosurg 24:865–875, 1966.
56. McLaughlin MR, Kondziolka D, Flickinger JC, Lunsford S, Lunsford LD: The
Japanese]. No To Shinkei 41:1135–1139, 1989.
prospective natural history of cerebral venous malformations. Neurosurgery
31. Houtteville JP: The surgery of cavernomas both supra-tentorial and infra-
43:195–201, 1998.
tentorial. Adv Tech Stand Neurosurg 22:185–259, 1995.
57. Mehdorn HM, Barth H, Buhl R, Nabavi A, Weinert D: Intracranial caver-
32. Huang YC, Tseng CK, Chang CN, Wei KC, Liao CC, Hsu PW: LINAC radio-
nomas: Indications for and results of surgery. Neurol Med Chir Suppl
surgery for intracranial cavernous malformation: 10-year experience. Clin
(Tokyo) 38:245–249, 1998.
Neurol Neurosurg 108:750–756, 2006.
58. Mitchell P, Hodgson TJ, Seaman S, Kemeny AA, Forster DM: Stereotactic
33. Karlsson B, Kihlström L, Lindquist C, Ericson K, Steiner L: Radiosurgery for
radiosurgery and the risk of haemorrhage from cavernous malformations. Br
cavernous malformations. J Neurosurg 88:293–297, 1998.
J Neurosurg 14:96–100, 2000.
34. Kayali H, Sait S, Serdar K, Kaan O, Ilker S, Erdener T: Intracranial caver- 59. Moriarity JL, Wetzel M, Clatterbuck RE, Javedan S, Sheppard JM, Hoenig-
nomas: analysis of 37 cases and literature review. Neurol India 52:439–442, Rigamonti K, Crone NE, Breiter SN, Lee RR, Rigamonti D: The natural his-
2004. tory of cavernous malformations. A prospective study of 68 patients.
35. Kerchner GA, Smith W, Lawton MT, Singh V: Co-occurrence of a cavernous Neurosurgery 44:1166–1173, 1999.
malformation and contralateral moyamoya. Neurology 66:1601–1602, 2006. 60. Mottolese C, Hermier M, Stan H, Jouvet A, Saint-Pierre G, Froment JC, Bret
36. Kida Y, Kobayashi T, Mori Y: Radiosurgery of angiographically occult vas- P, Lapras C: Central nervous system cavernomas in the pediatric age group.
cular malformations. Neurosurg Clin N Am 10:291–303, 1999. Neurosurg Rev 24:55–73, 2001.
37. Kim DS, Park YG, Choi JU, Chung SS, Lee KC: An analysis of the natural his- 61. Naff NJ, Wemmer J, Hoenig-Rigamonti K, Rigamonti DR: A longitudinal
tory of cavernous malformations. Surg Neurol 48:9–18, 1997. study of patients with venous malformations: Documentation of a negligible
38. Kim MS, Pyo SY, Jeong YG, Lee SI, Jung YT, Sim JH: Gamma knife surgery hemorrhage risk and benign natural history. Neurology 50:1709–1714, 1998.
for intracranial cavernous hemangioma. J Neurosurg 102 [Suppl]:102–106, 62. Otani N, Fujioka M, Oracioglu B, Muroi C, Khan N, Roth P, Yonekawa Y:
2005. Thalamic cavernous angioma: Paraculminar supracerebellar infratentorial
NEUROSURGERY VOLUME 65 | NUMBER 1 | JULY 2009 | 17
GROSS ET AL.
transtentorial approach for the safe and complete surgical removal. Acta 89. Tew JM Jr, Lewis AI, Reichert KW: Management strategies and surgical
Neurochir Suppl 103:29–36, 2008. techniques for deep-seated supratentorial arteriovenous malformations.
63. Otten P, Pizzolato GP, Rilliet B, Berney J: 131 cases of cavernous angiomas Neurosurgery 36:1065–1072, 1995.
(cavernomas) of the CNS, discovered by a retrospective analysis of 24,535 90. Thobois S, Jouanneau E, Bouvard M, Sindou M: Obsessive-compulsive dis-
autopsies [in French]. Neurochirurgie 35:82–83, 128–131, 1989. order after unilateral caudate nucleus bleeding. Acta Neurochir (Wien)
64. Pannek HW, Oppel F: Minimally invasive lesionectomies through a stereo- 146:1027–1031, 2004.
tactically guided working sleeve. Neurol Res 21:51–59, 1999. 91. Tomlinson FH, Houser OW, Scheithauer BW, Sundt TM Jr, Okazaki H, Parisi
65. Pollock BE, Garces YI, Stafford SL, Foote RL, Schomberg PJ, Link MJ: JE: Angiographically occult vascular malformations: A correlative study of
Stereotactic radiosurgery for cavernous malformations. J Neurosurg features on magnetic resonance imaging and histological examination.
93:987–991, 2000. Neurosurgery 34:792–800, 1994.
66. Porter RW, Detwiler PW, Spetzler RF, Lawton MT, Baskin JJ, Derksen PT, 92. Tung H, Giannotta SL, Chandrasoma PT, Zee CS: Recurrent intraparenchy-
mal hemorrhages from angiographically occult vascular malformations.
Zabramski JM: Cavernous malformations of the brainstem: Experience with
J Neurosurg 73:174–180, 1990.
100 patients. J Neurosurg 90:50–58, 1999.
93. Deleted in proof.
67. Porter PJ, Willinsky RA, Harper W, Wallace MC: Cerebral cavernous malfor-
94. Vaquero J, Salazar J, Martínez R, Martínez P, Bravo G: Cavernomas of the cen-
mations: Natural history and prognosis after clinical deterioration with or
tral nervous system: Clinical syndromes, CT scan diagnosis, and prognosis
without hemorrhage. J Neurosurg 87:190–197, 1997.
after surgical treatment in 25 cases. Acta Neurochir (Wien) 85:29–33, 1987.
68. Pozzati E: Thalamic cavernous malformations. Surg Neurol 53:30–40, 2000.
95. Voigt K, Yaşargil MG: Cerebral cavernous haemangiomas or cavernomas.
69. Pozzati E, Acciarri N, Tognetti F, Marliani F, Giangaspero F: Growth, subse-
Incidence, pathology, localization, diagnosis, clinical features and treatment.
quent bleeding, and de novo appearance of cerebral cavernous angiomas.
Review of the literature and report of an unusual case. Neurochirurgia
Neurosurgery 38:662–670, 1996. 19:59–68, 1976.
70. Pozzati E, Gaist G, Poppi M, Morrone B, Padovani R: Microsurgical removal 96. Waga S: Surgical treatment of arteriovenous malformations in the lateral
of paraventricular cavernous angiomas. J Neurosurg 55:308–311, 1981. ventricle. Neurol Res 8:18–24, 1986.
71. Robinson JR, Spetzler RF: An analysis of the natural history of cavernous 97. Wilson CB: Cryptic vascular malformations. Clin Neurosurg 38:49–84, 1992.
malformations. Surg Neurol 48:17–18, 1997 (comment). 98. Winkler D, Lindner D, Strauss G, Richter A, Schober R, Meixensberger J:
72. Robinson JR, Awad IA, Little JR: Natural history of the cavernous angioma. Surgery of cavernous malformations with and without navigational sup-
J Neurosurg 75:709–714, 1991. port—A comparative study. Minim Invasive Neurosurg 49:15–19, 2006.
73. Roda JM, Alvarez F, Isla A: Thalamic cavernous malformations. J Neurosurg 99. Yakinci C, Durmaz Y, Korkut M, Aladag A, Onal C, Aydinli M: Cavernous
75:169–170, 1991 (letter). hemangioma in a child presenting with hemichorea: Response to pimozide.
74. Roda JM, Alvarez F, Isla A, Blázquez MG: Thalamic cavernous malforma- J Child Neurol 16:685–688, 2001.
tion: Case report. J Neurosurg 72:647–649, 1990. 100. Yamasaki T, Handa H, Yamashita J, Paine JT, Tashiro Y, Uno A, Ishikawa M,
75. Rothbart D, Awad IA, Lee J, Kim J, Harbaugh R, Criscuolo GR: Expression Asato R: Intracranial and orbital cavernous angiomas. A review of 30 cases.
of angiogenic factors and structural proteins in central nervous system vas- J Neurosurg 64:197–208, 1986.
cular malformations. Neurosurgery 38:915–925, 1996. 101. Zamorano L, Matter A, Saenz A, Buciuc R, Diaz F: Interactive image-guided
76. Sarwar M, McCormick WF: Intracerebral venous angioma. Case report and resection of cerebral cavernous malformations. Comput Aided Surg
review. Arch Neurol 35:323–325, 1978. 2:327–332, 1997.
77. Sato K, Kubota T: Large calcified cystic cavernous angioma in the thala- 102. Zhao J, Wang Y, Kang S, Wang S, Wang J, Wang R, Zhao Y: The benefit of
mus—Case report. Neurol Med Chir (Tokyo) 35:100–103, 1995. neuronavigation for the treatment of patients with intracerebral cavernous
78. Scott RM, Barnes P, Kupsky W, Adelman LS: Cavernous angiomas of the malformations. Neurosurg Rev 30:313–319, 2007.
central nervous system in children. J Neurosurg 76:38–46, 1992.
79. Senegor M, Dohrmann GJ, Wollmann RL: Venous angiomas of the posterior
fossa should be considered as anomalous venous drainage. Surg Neurol COMMENTS
19:26–32, 1983.
80. Seo Y, Fukuoka S, Takanashi M, Nakagawara J, Suematsu K, Nakamura J,
Nagashima K: Gamma knife surgery for angiographically occult vascular
malformations. Stereotact Funct Neurosurg 64 [Suppl 1]:98–109, 1995.
T his research article is important. Gross et al. have not only dis-
cussed their own experience within the difficult field of cavernous
malformations of the basal ganglia and thalamus but have researched
81. Shucart WA, Stein BM: Transcallosal approach to the anterior ventricular the available literature and have drawn some conclusions. The review
system. Neurosurgery 3:339–343, 1978. is an excellent condensed summary formulated from the collection of
82. Simard JM, Garcia-Bengochea F, Ballinger WE Jr, Mickle JP, Quisling RG: literature published in French and English during the past 38 years.
Cavernous angioma: A review of 126 collected and 12 new clinical cases. The findings of this study are what neurosurgeons involved in this
Neurosurgery 18:162–172, 1986. specialized area need to know.
83. Stacey RJ, Ashkan K, Edwards JM: Rapid growth in a cavernoma. Br J
Neurosurg 14:585–588, 2000. Albino Bricolo
84. Stapf C, Mast H, Sciacca RR, Choi JH, Khaw AV, Connolly ES, Pile-Spellman Verona, Italy
J, Mohr JP: Predictors of hemorrhage in patients with untreated brain arte-
T
riovenous malformation. Neurology 66:1350–1355, 2006. he outcome of management of cavernous malformations is still less
85. Stea RA, Schicker L, King GA, Winfield JA: Stereotactic linear radiosurgery then optimal. On the other hand, they are relatively rare, and only
for cavernous angiomas. Stereotact Funct Neurosurg 63:255–265, 1994. a multicenter study can provide any statistically sound data. Despite
86. Steiger HJ, Markwalder TM, Reulen HJ: Clinicopathological relations of cere-
the limitations of a meta-analysis, it is currently the best option avail-
bral angiomas: Observations in eleven cases. Neurosurgery 21:879–884, 1987.
able. This is an extensive and very well-written meta-analysis of the
87. Steinberg GK, Chang SD, Gewirtz RJ, Lopez JR: Microsurgical resection of
brainstem, thalamic and basal ganglia angiographically occult vascular mal-
natural history and surgical and radiosurgical management of cav-
formations. Neurosurgery 46:260–271, 2000. ernous malformations of the basal ganglia and thalamus.
88. St George EJ, Perks J, Plowman PN: Stereotactic radiosurgery XIV: The role The natural history, clinical presentation, and surgical treatment,
of the haemosiderin ‘ring’ in the development of adverse reactions follow- including the alternative operative approaches, are discussed in detail.
ing radiosurgery for intracranial cavernous malformations: A sustainable Published data showed that in natural history studies, the annual
hypothesis. Br J Neurosurg 16:385–391, 2002. bleeding rates for these lesions was found to vary from 2.8% to 4.1%.
18 | VOLUME 65 | NUMBER 1 | JULY 2009 www.neurosurgery-online.com
CAVERNOUS MALFORMATIONS OF THE BASAL GANGLIA AND THALAMUS
Surgical series provided outcome data on 103 patients; the resection does not lie in the actual removal. The morbidity lies in the access cor-
rate was 89%, the risk of long-term surgical morbidity was 10%, and ridor necessary to reach the cavernous malformation. Lesions that pres-
the risk of surgical mortality was 1.9%. After radiosurgery, the risk of ent on pial or ependymal surfaces are more amenable to surgical extir-
hemorrhage declines in 2 years; however, it remains an option for pation because the access to the “real estate” is less morbid; 3)
patients with surgically inaccessible, aggressive lesions. radiosurgical management is an option for those patients who have
high-risk cavernous malformations with 2 or more bleeding episodes
Venelin M. Gerganov and who do not have a reasonable surgical corridor that can be used by
Madjid Samii experienced surgeons working in a center of excellence. In our experi-
Hannover, Germany ence of 102 solitary cavernous malformations located in deep areas of
critical brain function, the risk of bleeding in that group of patients
T his literature review is an excellent analysis of the current knowl-
edge base regarding cavernous malformations of the basal ganglia
and thalamus. These lesions are so rare that the only method for under-
decreases from 32% per year (after 2 prior bleeds) to 1% per year or less
after a latency interval of 2 years.
I believe that the doses described in this report are not correct. Doses
standing their natural history and treatment options is to pool the vary, but it is unlikely that marginal doses of 12 Gy are therapeutic. We
available clinical information. I completely agree with the conclusions believe that doses in the range of 13 to 16 Gy at the edge are more likely
of this study. to be effective. However, dose at the edge is only 1 factor. Highly con-
However, as the authors note, several biases are introduced in this formal and selective radiosurgery is critical. Modalities that are unable
type of report and should be highlighted. Most of the lesions reported to provide this degree of sharp dose falloff or selectivity in areas of crit-
in the literature will have presented with significant symptoms and/or ical brain function are much more likely to sustain radiosurgically
hemorrhage. Therefore, natural history information might not be rele- related morbidity. This is in part related to the hemosiderin stain sur-
vant for incidental or minimally symptomatic lesions. Similarly, the rounding brain (well seen on T2-weighted magnetic resonance imaging
surgical outcome data carry a publication bias, i.e., from surgeons with and dramatic on a gradient series which detects blood pigment).
extensive experience and relatively good outcomes. As well, for the Because this iron-sensitized brain is more likely to be affected by radio-
most part, surgeons have only performed resection on malformations surgical doses, we have emphasized radiosurgical dose conformality.
in these critical areas in patients with significant neurological deficits, Patients with multiple cavernous malformations, again, should be
and the potential morbidity for a minimally symptomatic patient is observed. Only those lesions that have had more than 2 bleeding events
vastly underestimated. should be considered for some form of surgical or radiosurgical man-
I have been very reluctant to operate on patients with cavernous agement. Clustering of bleeding events from a cavernous malformation
malformations in the basal ganglia, thalamus, internal capsule, and has been hypothesized, as noted within this article. However, this tem-
brainstem unless there is a clear path of progressive and devastating poral clustering phenomenon appears to be noted only in small series
neurological decline. The great majority of patients who present with and has not been verified in our experience (1, 2).
acute symptoms from these lesions will make a complete or near-com- We believe that this report provides additional data that support
plete recovery with conservative management and will not have recur- several options for cavernous malformation management. Perhaps a
rent problems. multicenter trial would be feasible. Patients with 2 or more bleeds
Robert A. Solomon could be randomized to observation or radiosurgery, provided that a
New York, New York microsurgical option is declined by the patient or is not feasible. Such
a prospective study might be performed by centers participating in
the North American Gamma Knife Consortium.
T he Northwestern University group presents their review of out-
comes related to various modalities for management of cavernous
malformations of the basal ganglia and thalamus. They emphasize sev-
L. Dade Lunsford
Pittsburgh, Pennsylvania
eral points that we fully agree with: 1) only patients with 2 or more
bleeding events (documented by new neurological signs or symptoms
and imaging confirmation of new blood products) warrant considera- 1. Hasegawa T, McInerney J, Kondziolka D, Lee JYK, Flickinger JC, Lunsford LD:
tion of a surgical or radiosurgical strategy; 2) malformations that pres- Long-term results after stereotactic radiosurgery for patients with cavernous
ent on a pial or ependymal surface are more amenable to surgical malformations. Neurosurgery 50:1190–1198, 2002.
approaches with less risk. The morbidity of removal of a cavernous 2. Kondziolka D, Lunsford LD, Kestle JRW: The natural history of cerebral cav-
malformation that is located in an area of deep or critical brain function ernous malformations. J Neurosurg 83:820–824, 1995.
NEUROSURGERY VOLUME 65 | NUMBER 1 | JULY 2009 | 19
You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Klinghardt Neurotoxin Elimination Protocol: Approved byDocument16 pagesThe Klinghardt Neurotoxin Elimination Protocol: Approved byNataša AndrićNo ratings yet
- Case HistoryDocument12 pagesCase HistoryEmmanuel Rojith Vaz0% (1)
- Notes in Ophthalmology: MCQ, Osce, SlidDocument21 pagesNotes in Ophthalmology: MCQ, Osce, SlidDrmhdh DrmhdhNo ratings yet
- 2.1 Medical Surgical Nursing - I Papers QPDocument15 pages2.1 Medical Surgical Nursing - I Papers QPAnju KarunakaranNo ratings yet
- ICO Clinical AssessmentDocument16 pagesICO Clinical AssessmentAmr AbdulradiNo ratings yet
- Neural Tube DefectDocument43 pagesNeural Tube DefectEllen AngelNo ratings yet
- Corynebacterium Diphtheria: Zainab A. AldhaherDocument41 pagesCorynebacterium Diphtheria: Zainab A. Aldhaherمروه عماد عيسىNo ratings yet
- Gram Positive Cocci Sem 1 1Document45 pagesGram Positive Cocci Sem 1 1Charmaine Corpuz Granil100% (1)
- AVM Pediatric LilleDocument9 pagesAVM Pediatric LilleZdravko HeinrichNo ratings yet
- Cerebral Cavernous Malformation, Familial - GeneReviews™ - NCBI BookshelfDocument22 pagesCerebral Cavernous Malformation, Familial - GeneReviews™ - NCBI BookshelfZdravko HeinrichNo ratings yet
- cavernomi-GK Contra OpDocument5 pagescavernomi-GK Contra OpZdravko HeinrichNo ratings yet
- CM PediatricsDocument8 pagesCM PediatricsZdravko HeinrichNo ratings yet
- Rainstem Avernous Alformations: ReviewsDocument14 pagesRainstem Avernous Alformations: ReviewsZdravko HeinrichNo ratings yet
- AVM Definition of The Key Target Volume in Radiosurgical PDFDocument10 pagesAVM Definition of The Key Target Volume in Radiosurgical PDFZdravko HeinrichNo ratings yet
- AVM Haemoorhage Managemnt After GKDocument6 pagesAVM Haemoorhage Managemnt After GKZdravko HeinrichNo ratings yet
- AVM Prior EmbolizationDocument10 pagesAVM Prior EmbolizationZdravko HeinrichNo ratings yet
- AVM GK Versus LinacDocument6 pagesAVM GK Versus LinacZdravko HeinrichNo ratings yet
- Brain Map MainDocument1 pageBrain Map MainUmar MajeedNo ratings yet
- AVM - RS To Reduce The Risk of First HaemorrhageDocument7 pagesAVM - RS To Reduce The Risk of First HaemorrhageZdravko HeinrichNo ratings yet
- Arteriovenous Malformations After Leksell Gamma.5Document12 pagesArteriovenous Malformations After Leksell Gamma.5Zdravko HeinrichNo ratings yet
- Angioarchitecture Determines Obliteration Rate.13Document9 pagesAngioarchitecture Determines Obliteration Rate.13Zdravko HeinrichNo ratings yet
- Anatomic Landmarks Vs Fiducials For Staged Gamma Knife RadioDocument1 pageAnatomic Landmarks Vs Fiducials For Staged Gamma Knife RadioZdravko HeinrichNo ratings yet
- A Practical Grading Scale For Predicting Outcome AfterDocument7 pagesA Practical Grading Scale For Predicting Outcome AfterZdravko HeinrichNo ratings yet
- Atlas of Approaches in Neurosurgery - J.FischerDocument7 pagesAtlas of Approaches in Neurosurgery - J.FischerZdravko HeinrichNo ratings yet
- January 1994, Volume 34, Number 1: Neurosurgery 1992-98 163 Intracranial Suprasellar AngiolipomaDocument8 pagesJanuary 1994, Volume 34, Number 1: Neurosurgery 1992-98 163 Intracranial Suprasellar AngiolipomaZdravko HeinrichNo ratings yet
- Microsurgical Anatomy Vertebral ArteryDocument9 pagesMicrosurgical Anatomy Vertebral ArteryZdravko HeinrichNo ratings yet
- Dynamic MR Digital Subtraction Angiography 1Document6 pagesDynamic MR Digital Subtraction Angiography 1Zdravko HeinrichNo ratings yet
- Angiofibroma GK BuffaloDocument5 pagesAngiofibroma GK BuffaloZdravko HeinrichNo ratings yet
- Anatomy Review For NeurosurgeryDocument7 pagesAnatomy Review For Neurosurgeryvasu_5ive100% (1)
- ICA Aneurism PDFDocument6 pagesICA Aneurism PDFTiger PowerNo ratings yet
- Gamma Knife Radiosurgery For Cerebellopontine Angle Epidermoid TumorsDocument11 pagesGamma Knife Radiosurgery For Cerebellopontine Angle Epidermoid TumorsZdravko HeinrichNo ratings yet
- Aneurizme KoreaDocument6 pagesAneurizme KoreaZdravko HeinrichNo ratings yet
- Neurology Shelf Exam Study Guide and Audio TranscriptDocument12 pagesNeurology Shelf Exam Study Guide and Audio TranscriptyogurtNo ratings yet
- GMMMG Dental Prescribing Guidelines February 2020 v1 0Document4 pagesGMMMG Dental Prescribing Guidelines February 2020 v1 0Erick GuanoluisaNo ratings yet
- Case StudyDocument2 pagesCase StudyClaire MachicaNo ratings yet
- Eurican Technicalsheet 12-08-2019Document2 pagesEurican Technicalsheet 12-08-2019dzulfikarfaizin romasNo ratings yet
- COLOUR PHOTO OF LIFE INSURANCE PROPOSALDocument10 pagesCOLOUR PHOTO OF LIFE INSURANCE PROPOSALRAKTIM PUJARINo ratings yet
- HLH 265 CH 1 Activity - ArtifactDocument2 pagesHLH 265 CH 1 Activity - Artifactapi-665749684No ratings yet
- Mini OSCE Surgery-Group A - Soul 2014Document18 pagesMini OSCE Surgery-Group A - Soul 2014Hasan H.No ratings yet
- Hepatitis BDocument3 pagesHepatitis Bkrishna chandrakani100% (1)
- PCR Test Shows Positive Result for COVID-19Document2 pagesPCR Test Shows Positive Result for COVID-19Kinuthia MathewNo ratings yet
- Preoperative Care of The Patient Undergoing Orthopedic SurgeryDocument26 pagesPreoperative Care of The Patient Undergoing Orthopedic SurgeryAbdul Gafoor CPNo ratings yet
- Drug StudyDocument7 pagesDrug Studykristen_ramos_3No ratings yet
- Understanding Addison Disease and Its SymptomsDocument18 pagesUnderstanding Addison Disease and Its SymptomsVanetNo ratings yet
- NCM 112 LEC Topic 2 Oxygenation Current Health History Physical Examination Normal Abnormal Breath Sounds Breathing PatternsDocument7 pagesNCM 112 LEC Topic 2 Oxygenation Current Health History Physical Examination Normal Abnormal Breath Sounds Breathing PatternsViviene Faye FombuenaNo ratings yet
- Lisinopril PDFDocument3 pagesLisinopril PDFHannaNo ratings yet
- Homelessness and Burns - Joan ChenDocument16 pagesHomelessness and Burns - Joan ChenJjoan ChchenNo ratings yet
- Second Periodical Test in ScienceDocument2 pagesSecond Periodical Test in ScienceLorraine lee100% (1)
- Pedia UST Blue BookDocument206 pagesPedia UST Blue BookMattNo ratings yet
- Medicine Viva Notes by Dr. VaidyaDocument57 pagesMedicine Viva Notes by Dr. VaidyaFariha AnsariNo ratings yet
- Quick and Easy Medical Terminology 8Th Edition Leonard Test Bank Full Chapter PDFDocument27 pagesQuick and Easy Medical Terminology 8Th Edition Leonard Test Bank Full Chapter PDFmathewsandersa13j100% (7)
- IN-VITRO ANALYSIS OF Moringa Oleifera Lam. LEAVES AND: Curcuma Longa Linn. Extract As A ManducableDocument92 pagesIN-VITRO ANALYSIS OF Moringa Oleifera Lam. LEAVES AND: Curcuma Longa Linn. Extract As A ManducableJerico CenizaNo ratings yet
- Eposter - Mental Health in The Greater Third WardDocument1 pageEposter - Mental Health in The Greater Third Wardapi-532700233No ratings yet
- Xeloda Tablets Description:: BioactivationDocument19 pagesXeloda Tablets Description:: BioactivationDrogoman MarianNo ratings yet