You might also like
- Cell Cycle Regulators: Namrata Sengupta Mds 1 Year Oral Pathology & MicrobiologyDocument33 pagesCell Cycle Regulators: Namrata Sengupta Mds 1 Year Oral Pathology & MicrobiologyMadhura ShekatkarNo ratings yet
- Dna Replication Worksheet 1Document2 pagesDna Replication Worksheet 1Lovryan Tadena AmilingNo ratings yet
- MTI Field Guide To Inspection of FRPDocument51 pagesMTI Field Guide To Inspection of FRPAndrés Franco67% (3)
- Polymer DegradationDocument5 pagesPolymer Degradationrehrifat2000No ratings yet
- 9701 w12 Ms 41Document11 pages9701 w12 Ms 41Matthew Vinodh RajNo ratings yet
- Mdds IjbDocument11 pagesMdds IjbpranshuNo ratings yet
- Mucoadhesive Drug Delivery SystemsDocument13 pagesMucoadhesive Drug Delivery SystemsSiddhi MehtaNo ratings yet
- International Journal of Pharma and Bio Sciences: ReviewDocument10 pagesInternational Journal of Pharma and Bio Sciences: ReviewRajesh KumarNo ratings yet
- Mucoadhesive Microspheres For Novel Drug Delivery System: A ReviewDocument19 pagesMucoadhesive Microspheres For Novel Drug Delivery System: A ReviewRavindra RawalNo ratings yet
- Muco AdhesiveDocument47 pagesMuco Adhesivemonika1983007No ratings yet
- Mucoadhesive Drug Delivery System PDFDocument42 pagesMucoadhesive Drug Delivery System PDFdrgdswNo ratings yet
- Bacterial Biofilm Under Flow First A Physical Struggle To Stay, Then A Matter of BreathingDocument24 pagesBacterial Biofilm Under Flow First A Physical Struggle To Stay, Then A Matter of BreathingWhite SpireNo ratings yet
- Resumen Segundo Corte.Document19 pagesResumen Segundo Corte.NELLYS ENITH MOGROBEJO ALVAREZ ESTUDIANTE ACTIVONo ratings yet
- INTRODUCTION:-Most of The Medicinal: Mucadhesiv AgentDocument21 pagesINTRODUCTION:-Most of The Medicinal: Mucadhesiv AgentShubham lodhi LodhiNo ratings yet
- Bayoudh09 XDLVODocument10 pagesBayoudh09 XDLVOJessica ChenNo ratings yet
- 5 Buccal Drug Delivery System A ReviewDocument14 pages5 Buccal Drug Delivery System A ReviewHely PatelNo ratings yet
- Muco AdhesiveDocument22 pagesMuco AdhesiveMaverickdeepakNo ratings yet
- Mechanisms of Action of DisinfectantsDocument8 pagesMechanisms of Action of DisinfectantsAlagu SolaimalaiNo ratings yet
- mAIN eDITEDDocument57 pagesmAIN eDITEDcity9848835243 cyberNo ratings yet
- Ultrasonics - Sonochemistry: SciencedirectDocument11 pagesUltrasonics - Sonochemistry: SciencedirectBreeze ChloeNo ratings yet
- Microneedle System For Transdermal Drug and Vaccine DeliveryDocument18 pagesMicroneedle System For Transdermal Drug and Vaccine Delivery郭先薈No ratings yet
- Mucoadhesive DDSDocument25 pagesMucoadhesive DDSShubhrajit MantryNo ratings yet
- Bacteria Adhesion CoatingDocument11 pagesBacteria Adhesion CoatingWilliam VenegasNo ratings yet
- Muco Ijprd PDFDocument12 pagesMuco Ijprd PDFpranshuNo ratings yet
- Katarina Mucoadhesion PDFDocument20 pagesKatarina Mucoadhesion PDFleNo ratings yet
- Docsity Mucoadhesive Drug Delivery SystemDocument16 pagesDocsity Mucoadhesive Drug Delivery SystemSahil SolankiNo ratings yet
- Mucoadhesive Microspheres: A Short Review: Asian Journal of Pharmaceutical and Clinical Research January 2012Document5 pagesMucoadhesive Microspheres: A Short Review: Asian Journal of Pharmaceutical and Clinical Research January 2012Indri AuraliaNo ratings yet
- Mucoadhesive Multiparticulate Drug Delivery Systems: An Extensive Review of PatentsDocument18 pagesMucoadhesive Multiparticulate Drug Delivery Systems: An Extensive Review of PatentsIndri AuraliaNo ratings yet
- A Brief Review Biomaterials and Their ApllicationDocument6 pagesA Brief Review Biomaterials and Their ApllicationaaliyaNo ratings yet
- Temporal Pressure Enhanced Topical Drug Delivery Through Micropore FormationDocument14 pagesTemporal Pressure Enhanced Topical Drug Delivery Through Micropore FormationMuhammadRomadonSyolehhudinNo ratings yet
- Occlusive vs. Non OcclusiveDocument7 pagesOcclusive vs. Non OcclusiveSara HussienNo ratings yet
- mAIN eDITEDDocument59 pagesmAIN eDITEDcity9848835243 cyberNo ratings yet
- Nanomaterials 12 00552 v2Document47 pagesNanomaterials 12 00552 v2Erika Joyce ValenzuelaNo ratings yet
- Adsorption Kinetics and Isotherm Models: A Review: ArticleDocument8 pagesAdsorption Kinetics and Isotherm Models: A Review: ArticleRahul PatwaNo ratings yet
- Polymers: Recent Advances in Tissue Adhesives For Clinical MedicineDocument22 pagesPolymers: Recent Advances in Tissue Adhesives For Clinical MedicineGonzalo MTNo ratings yet
- A Brief Review - Biomaterials and Their ApllicationDocument5 pagesA Brief Review - Biomaterials and Their ApllicationHammadiNo ratings yet
- Adsorption of Three Pesticides On Polyethylene Microplastics inDocument9 pagesAdsorption of Three Pesticides On Polyethylene Microplastics inTelma OliveiraNo ratings yet
- Chitosan Nanoparticles: A Promising System For Drug DeliveryDocument17 pagesChitosan Nanoparticles: A Promising System For Drug DeliveryUMY HABIBANo ratings yet
- 颊侧带蒂瓣 Clin Adv Periodontics - 2021 - Tabanella - Buccal Pedicle Flap Combined With Porcine Collagen Matrix A Follow‐Up of 2Document8 pages颊侧带蒂瓣 Clin Adv Periodontics - 2021 - Tabanella - Buccal Pedicle Flap Combined With Porcine Collagen Matrix A Follow‐Up of 2xiaoxin zhangNo ratings yet
- Mucosal Drug Delivery SystemDocument32 pagesMucosal Drug Delivery SystemROHIT SINGHNo ratings yet
- Fnano 03 753947 1Document21 pagesFnano 03 753947 1sakuraNo ratings yet
- Formulation and Evaluation of Floating Microspheres of Metformin HydrochlorideDocument10 pagesFormulation and Evaluation of Floating Microspheres of Metformin HydrochlorideBaru Chandrasekhar RaoNo ratings yet
- Ali - 2020 - Comp. - Methods - in - Biomech. - Biomedeical EngineeringDocument13 pagesAli - 2020 - Comp. - Methods - in - Biomech. - Biomedeical EngineeringMahmoodAliNo ratings yet
- WilliamDocument25 pagesWilliamGuilherme RomeroNo ratings yet
- How Do Bacteria Know They Are On A Surface and Regulate Their Response To An Adhering State?Document3 pagesHow Do Bacteria Know They Are On A Surface and Regulate Their Response To An Adhering State?shargunan11No ratings yet
- Multiwalled Carbon Nanotube-Doxorubicin Supramolecular Complexes For Cancer TherapeuticsDocument3 pagesMultiwalled Carbon Nanotube-Doxorubicin Supramolecular Complexes For Cancer TherapeuticsElena AnghelNo ratings yet
- Biosensors and Bioelectronics: A 1 B 1 A BDocument14 pagesBiosensors and Bioelectronics: A 1 B 1 A BHozefa DhilaNo ratings yet
- Mucosal Drug Delivery SystemDocument34 pagesMucosal Drug Delivery SystemDebjani Baidya100% (1)
- Recent Advances in Natural Polymer-Based Drug Delivery SystemsDocument18 pagesRecent Advances in Natural Polymer-Based Drug Delivery SystemsTelmoNo ratings yet
- CaoYaxin TRAC 117442Document19 pagesCaoYaxin TRAC 117442osadchyi47No ratings yet
- 2023 Article 1121Document18 pages2023 Article 1121Robert StryjakNo ratings yet
- 1 s2.0 S0144861722006920 MainDocument17 pages1 s2.0 S0144861722006920 MainDominic Estiven Sisaya SisayaNo ratings yet
- As Featured In:: Hybrid Composites of Xanthan and Magnetic Nanoparticles For Cellular UptakeDocument4 pagesAs Featured In:: Hybrid Composites of Xanthan and Magnetic Nanoparticles For Cellular UptakeSqual59No ratings yet
- 3708-Article Text-10469-1-10-20191111Document10 pages3708-Article Text-10469-1-10-20191111YunitaNo ratings yet
- Bio Medical Surface Science Foundations To FrontiersDocument33 pagesBio Medical Surface Science Foundations To FrontiersRoxana StoicaNo ratings yet
- The Biocompatibility Manifesto: Biocompatibility For The Twenty-First CenturyDocument5 pagesThe Biocompatibility Manifesto: Biocompatibility For The Twenty-First CenturyCaraman ConstantinNo ratings yet
- Molecular Dynamics Simulations Advances and ApplicationsDocument11 pagesMolecular Dynamics Simulations Advances and Applicationsbaotrann.dangngocNo ratings yet
- Silk Fibroinchitosanalginate Multilayer Membranes As A System For Controlled Drug Release in Wound HealingDocument9 pagesSilk Fibroinchitosanalginate Multilayer Membranes As A System For Controlled Drug Release in Wound HealingвикторNo ratings yet
- Acoustic Bubble Based Drug Manipulation Carrying Releasing and Penetrating For Targeted Drug Delivery Using MicrorobotDocument9 pagesAcoustic Bubble Based Drug Manipulation Carrying Releasing and Penetrating For Targeted Drug Delivery Using MicrorobotFurkan KolayNo ratings yet
- Bacterial Population Control With Macroscopic HKUST CrystalsDocument6 pagesBacterial Population Control With Macroscopic HKUST CrystalsLuisa Fernanda Munera GomezNo ratings yet
- Secretory Membrane Traffic in Plant Microbe InteractionsDocument7 pagesSecretory Membrane Traffic in Plant Microbe InteractionsAlberto MachoNo ratings yet
- Dissolvable Microneedle Arrays For Intradermal Delivery of Biologics: Fabrication and ApplicationDocument19 pagesDissolvable Microneedle Arrays For Intradermal Delivery of Biologics: Fabrication and ApplicationAndisheh ChoupaniNo ratings yet
- Pharmaceutics 14 00191Document26 pagesPharmaceutics 14 00191Kajal MIshraNo ratings yet
- Wang Et Al-2017-Frontiers in PhysiologyDocument3 pagesWang Et Al-2017-Frontiers in Physiologymaya yulindhiniNo ratings yet
- Liter Pembahasan AntosianinDocument7 pagesLiter Pembahasan AntosianinEndang SinamoNo ratings yet
- Karakterisasi Bahan Anti Browning Dari Ekstrak Air Buah Jambu Batu (Psidium Guajava Linn) Pada Buah Apel Malang (Malus Sylvestris (L.) Mill)Document8 pagesKarakterisasi Bahan Anti Browning Dari Ekstrak Air Buah Jambu Batu (Psidium Guajava Linn) Pada Buah Apel Malang (Malus Sylvestris (L.) Mill)Endang SinamoNo ratings yet
- Efektivitas Ekstrak Daging Buah Nanas (Ananas Comosus L.) Dalam Penurunan Indeks Browning Dari Umbi Kentang (Solanum TuberosumDocument7 pagesEfektivitas Ekstrak Daging Buah Nanas (Ananas Comosus L.) Dalam Penurunan Indeks Browning Dari Umbi Kentang (Solanum TuberosumMuti MainahNo ratings yet
- Kentang 2Document7 pagesKentang 2Galih Setia AdiNo ratings yet
- Gumerov 2019 IOP Conf. Ser.: Mater. Sci. Eng. 687 066064Document7 pagesGumerov 2019 IOP Conf. Ser.: Mater. Sci. Eng. 687 066064Endang SinamoNo ratings yet
- Frank2017 Article TransepithelialTransportOfCurcDocument6 pagesFrank2017 Article TransepithelialTransportOfCurcEndang SinamoNo ratings yet
- Rhodophyta SPDocument2 pagesRhodophyta SPEndang SinamoNo ratings yet
- Afa Reviewer ADocument28 pagesAfa Reviewer AJane CastroNo ratings yet
- Ketones ReviewDocument19 pagesKetones ReviewCamiloVerdugoNo ratings yet
- Spectroscopic Solutions of StructureDocument21 pagesSpectroscopic Solutions of StructureKassimNo ratings yet
- Tutorial 2Document10 pagesTutorial 2Ahmad WahideeNo ratings yet
- Ethers, Epoxides and Glycols: Loudon Chapter 11 ReviewDocument5 pagesEthers, Epoxides and Glycols: Loudon Chapter 11 ReviewxryceuNo ratings yet
- Es NotesDocument25 pagesEs NotesKESOCAKENo ratings yet
- Chemistry in Everyday Life Exercise PDFDocument8 pagesChemistry in Everyday Life Exercise PDFSamridh GuptaNo ratings yet
- Polyol Y-1537 Technical Data Sheet: Specifications Guide FormulationDocument1 pagePolyol Y-1537 Technical Data Sheet: Specifications Guide FormulationVaittianathan MahavapillaiNo ratings yet
- A1 Halogenoalkanes WS1Document15 pagesA1 Halogenoalkanes WS1chantellelimNo ratings yet
- Guidelines NaturaDocument16 pagesGuidelines NaturaAlizé BarangéNo ratings yet
- PsychrobacterDocument15 pagesPsychrobacterehab homoudNo ratings yet
- United States Patent: MG, Christopher Lbecke, (58) Field of Classification SearchDocument11 pagesUnited States Patent: MG, Christopher Lbecke, (58) Field of Classification SearchAkbarNo ratings yet
- Protocol - Gap PCR IthapediaDocument9 pagesProtocol - Gap PCR IthapediaAnh TranNo ratings yet
- Cylindrospermopsin SynthesisDocument8 pagesCylindrospermopsin SynthesisSơn Nguyễn KimNo ratings yet
- Sac 301 HighlightedDocument448 pagesSac 301 HighlightedKavin0% (1)
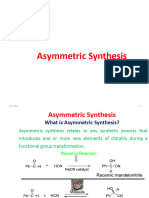
- Asymmetric SynthesisDocument29 pagesAsymmetric SynthesisM. ABDUR REHMANNo ratings yet
- Chemical Reactions-Multiple Choice Review: PSI ChemistryDocument15 pagesChemical Reactions-Multiple Choice Review: PSI Chemistrykatherine corveraNo ratings yet
- Acrylonitrile Butadiene Styrene - UV Stabilized and General Purpose, Heat StabilizedDocument7 pagesAcrylonitrile Butadiene Styrene - UV Stabilized and General Purpose, Heat StabilizedJefferson CruzNo ratings yet
- 02 Milk & Milk ProductsDocument24 pages02 Milk & Milk ProductsAlecsa RobertNo ratings yet
- Unit 10 EcosystemDocument13 pagesUnit 10 EcosystemDevang ParekhNo ratings yet
- Tutorial 1 Answers Q6-Q11Document6 pagesTutorial 1 Answers Q6-Q11A/P SUPAYA SHALININo ratings yet
- Purification of LipidDocument13 pagesPurification of LipidNurakmal SyuhAdaNo ratings yet
- GEOSYNTHETICDocument5 pagesGEOSYNTHETICAnas IaNo ratings yet
- 1st Midterm For Polymer Chemistry 11/20/2013 (Total:120 Points) Department of Materials Science and Engineering, NTUST Chapter 1,2,11Document2 pages1st Midterm For Polymer Chemistry 11/20/2013 (Total:120 Points) Department of Materials Science and Engineering, NTUST Chapter 1,2,11吳睿哲No ratings yet