You might also like
- Trifold Vaccine Card ENGLISHDocument2 pagesTrifold Vaccine Card ENGLISHGarrett GoldwaiteNo ratings yet
- BCCDC Adult Record CardDocument2 pagesBCCDC Adult Record CardYoj SaraNo ratings yet
- 5 Idol Ko Si Nanay Module 5Document48 pages5 Idol Ko Si Nanay Module 5Mash JumahariNo ratings yet
- 4 Idol Ko Si Nanay Module 4Document18 pages4 Idol Ko Si Nanay Module 4Mash JumahariNo ratings yet
- Narrative Report ShadowingDocument18 pagesNarrative Report ShadowingThriska Ravven Resurreccion100% (1)
- Lyiny inDocument11 pagesLyiny inSi Kaye100% (3)
- Notification of Vaccination Letter Template: Vaccines AdministeredDocument1 pageNotification of Vaccination Letter Template: Vaccines AdministeredJacob BuckNo ratings yet
- Recording Form1 Masterlist of Grade 1 StudentsDocument1 pageRecording Form1 Masterlist of Grade 1 StudentsSandra Nicole TorresNo ratings yet
- Vaccine Administration Record For Children and TeensDocument2 pagesVaccine Administration Record For Children and TeensGian Franco ApesNo ratings yet
- Adverse Events Following Immunization: Philippine Integrated DiseaseDocument2 pagesAdverse Events Following Immunization: Philippine Integrated DiseaseRex DoctoNo ratings yet
- Dosage Frequenc Ast Se A E As Ak G: / Y L Do T K N Re Onfort inDocument2 pagesDosage Frequenc Ast Se A E As Ak G: / Y L Do T K N Re Onfort inRachel DolanNo ratings yet
- Vaccination Records - AdultsDocument2 pagesVaccination Records - AdultsverumluxNo ratings yet
- Pregnancy Health RecordDocument28 pagesPregnancy Health Recordrg2r5gmqykNo ratings yet
- Immunization RecordDocument4 pagesImmunization RecordVin BitzNo ratings yet
- Appropriate Antibiotic Selection Draft 02Document2 pagesAppropriate Antibiotic Selection Draft 02Bryan MahendraNo ratings yet
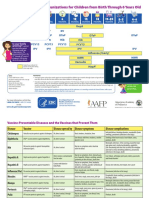
- Recommended Childhood Vaccine Schedule 2018Document2 pagesRecommended Childhood Vaccine Schedule 2018Saddam HussainNo ratings yet
- Vaccine Administration Record For AdultsDocument2 pagesVaccine Administration Record For AdultsAlfonso VincentNo ratings yet
- PHE Complete Immunisation Schedule Jun2020 05Document2 pagesPHE Complete Immunisation Schedule Jun2020 05GAnnNo ratings yet
- Immunization Record: Haemophilus InfluenzaeDocument2 pagesImmunization Record: Haemophilus InfluenzaeApshar MunnaNo ratings yet
- Cis 2018 PDFDocument3 pagesCis 2018 PDFTara Oliveros Dela CruzNo ratings yet
- History FormDocument5 pagesHistory FormYazeed AsrawiNo ratings yet
- Parent Ver SCH 0 6yrsDocument2 pagesParent Ver SCH 0 6yrsunmundoextranopodcastNo ratings yet
- School Immunization RecordsDocument1 pageSchool Immunization RecordsJean Francis ReyesNo ratings yet
- Record pneumococcal vaccinationDocument1 pageRecord pneumococcal vaccinationalfredtan6288No ratings yet
- PHE Complete Immunisation Schedule Jan2020 PDFDocument2 pagesPHE Complete Immunisation Schedule Jan2020 PDFJyotirmaya RajaNo ratings yet
- (LIST) Adult VaccinationsDocument4 pages(LIST) Adult VaccinationsLeslie MartinezNo ratings yet
- 2010 Adolescent Immunization Schedule Final 121709Document1 page2010 Adolescent Immunization Schedule Final 121709Dustin Van WilkesNo ratings yet
- S3 L16 FlaviviridaeDocument6 pagesS3 L16 Flaviviridae2013SecBNo ratings yet
- Hai Toolkit For LTCDocument82 pagesHai Toolkit For LTCShannaNo ratings yet
- Vaccination Records - Children and TeensDocument4 pagesVaccination Records - Children and TeensverumluxNo ratings yet
- Ontario Immunization Schedule ENDocument1 pageOntario Immunization Schedule ENMing XieNo ratings yet
- Vaccination ScheduleDocument1 pageVaccination ScheduleAmanda KamienNo ratings yet
- Deep Pathology LabDocument1 pageDeep Pathology LabSanjeev KatariaNo ratings yet
- PHE Complete Immunisation ScheduDocument2 pagesPHE Complete Immunisation ScheduJasminewai927No ratings yet
- Full Medical Alert ListDocument2 pagesFull Medical Alert ListCarlosDanielNo ratings yet
- Vaccination Certificate Edit1 (Patricia)Document1 pageVaccination Certificate Edit1 (Patricia)Marcella LuhulimaNo ratings yet
- 0 To 18yrs Combined Immunization ScheduleDocument8 pages0 To 18yrs Combined Immunization ScheduleNurses CommunityNo ratings yet
- Parent Ver SCH 0 6yrsDocument2 pagesParent Ver SCH 0 6yrsMatri SearchNo ratings yet
- InfluenzaDocument1 pageInfluenzaninzah wanzahNo ratings yet
- Ce Midw PDFDocument52 pagesCe Midw PDFMadhusudan SamantaNo ratings yet
- The Routine Immunisation Schedule: From Autumn 2018Document2 pagesThe Routine Immunisation Schedule: From Autumn 2018Adityo AriwibowoNo ratings yet
- Case Investigation Form for Serious AEFIDocument6 pagesCase Investigation Form for Serious AEFIVic KwanNo ratings yet
- Analitico ManualDocument2 pagesAnalitico ManuallissetemNo ratings yet
- Booster VaxCardDocument1 pageBooster VaxCardmarialagajino05No ratings yet
- EPI Formula SheetDocument4 pagesEPI Formula Sheet2rpghsjrsdNo ratings yet
- Form 3 - HPV Masterlistingv FormDocument1 pageForm 3 - HPV Masterlistingv Formeloisa mae malitaoNo ratings yet
- TN Immunization Certificate Sample PDFDocument2 pagesTN Immunization Certificate Sample PDFapi-381653951No ratings yet
- Health Care Professionals Refusal To Vaccinate Form English 3Document1 pageHealth Care Professionals Refusal To Vaccinate Form English 3Marshall FeatherNo ratings yet
- covidVaccinationCard 1643563Document1 pagecovidVaccinationCard 1643563Kelvin ChinNo ratings yet
- UKHSA 12706 Complete Immunisation Schedule September2023Document2 pagesUKHSA 12706 Complete Immunisation Schedule September2023Ebuwa AmadasunNo ratings yet
- Purposes Only Download and Print: Antenatal AssessmentDocument2 pagesPurposes Only Download and Print: Antenatal AssessmentHadiyasa JatmikaNo ratings yet
- CertificatDocument2 pagesCertificatnatalia.seremet79No ratings yet
- Massachusetts immunization certificate guideDocument1 pageMassachusetts immunization certificate guidePrecilla Janet RosarioNo ratings yet
- Case Investigation Form: Name of Disease Reporting Unit: I. Patient InformationDocument4 pagesCase Investigation Form: Name of Disease Reporting Unit: I. Patient Informationjuwan decastroNo ratings yet
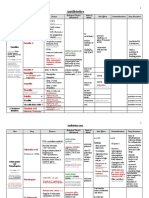
- Antimicrobial Drugs TableDocument19 pagesAntimicrobial Drugs TableLaylee ClareNo ratings yet
- Typhoid and Paratyphoid Fever Surveillance Report FormDocument1 pageTyphoid and Paratyphoid Fever Surveillance Report FormGFVNo ratings yet
- Immunization PPT - EditedDocument22 pagesImmunization PPT - EditedAlfred Mutua MutungaNo ratings yet
- Managing measles outbreaks in hospitalsDocument1 pageManaging measles outbreaks in hospitalsJose BritesNo ratings yet
- Panorama of Immunization in The Americas: Webinar: Covering COVID-19 Vaccines in A Responsible and Evidence-Based MannerDocument61 pagesPanorama of Immunization in The Americas: Webinar: Covering COVID-19 Vaccines in A Responsible and Evidence-Based MannerM. RodriguesNo ratings yet
- Baby Shots EngDocument2 pagesBaby Shots Engsunmo8217No ratings yet
- Evaluation of Diarrhea in ChildrenDocument21 pagesEvaluation of Diarrhea in ChildrenDagnachew kasayeNo ratings yet
- Pharmacology: Antiparasitic DrugsDocument3 pagesPharmacology: Antiparasitic DrugsKrizza Mae Camantiles ThompsonNo ratings yet
- Sepsis: Signs and SymptomsDocument5 pagesSepsis: Signs and SymptomssujithasNo ratings yet
- Pharmacology of Antiviral DrugsDocument1 pagePharmacology of Antiviral Drugssarah90222100% (1)
- Promising natural antimicrobial strategies for food biopreservationDocument10 pagesPromising natural antimicrobial strategies for food biopreservationTran Thach Uyen NhiNo ratings yet
- DenguDocument35 pagesDenguMahesh MohantaNo ratings yet
- Infection Prevention and Control at NICU Slide Deck 2.8.2018 PDFDocument134 pagesInfection Prevention and Control at NICU Slide Deck 2.8.2018 PDFRevathi DadamNo ratings yet
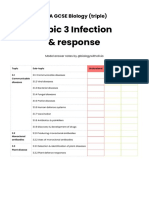
- FREE SAMPLE - Topic 3Document5 pagesFREE SAMPLE - Topic 3Alicia CarterNo ratings yet
- Anatomy, Causes, Symptoms and Treatment of Tongue CancerDocument21 pagesAnatomy, Causes, Symptoms and Treatment of Tongue CancerEunice RiveraNo ratings yet
- Viruses and Their PropertiesDocument7 pagesViruses and Their PropertiesJustin MirandoNo ratings yet
- SDB Communication Guidance For IHE PCD-01 DEC (HL7) 1.3.0Document27 pagesSDB Communication Guidance For IHE PCD-01 DEC (HL7) 1.3.0Jose Perez PerezNo ratings yet
- Phylum Aschelminthes - FormattedDocument30 pagesPhylum Aschelminthes - FormattedkingNo ratings yet
- Slide 14 Diseases of Salivary Glands IDocument67 pagesSlide 14 Diseases of Salivary Glands IJustDen09No ratings yet
- 00014Document5 pages00014Dauz ArashNo ratings yet
- AF SeedingDocument6 pagesAF SeedingdonkeyendutNo ratings yet
- Kato-Katz and Cellophane Thick Smear Techniques for Parasite DetectionDocument1 pageKato-Katz and Cellophane Thick Smear Techniques for Parasite DetectionKim G. SarongNo ratings yet
- ManimozhiDocument12 pagesManimozhiMohamad BasofiNo ratings yet
- Red Biotechnology ProjectDocument5 pagesRed Biotechnology ProjectNeveen Kandil100% (2)
- Unit Layanan High Risk High Cost High Volume N B N B NDocument12 pagesUnit Layanan High Risk High Cost High Volume N B N B Npkm.ngempit22No ratings yet
- Head and Neck CancersDocument41 pagesHead and Neck CancersskhananiNo ratings yet
- Communicable vs Non-Communicable DiseasesDocument8 pagesCommunicable vs Non-Communicable DiseasesSuvashreePradhanNo ratings yet
- Cancer Classification Agents Evidence Humans Volumes 112Document12 pagesCancer Classification Agents Evidence Humans Volumes 112Bruno ThiemeNo ratings yet
- BT 501 Current Final TermsDocument8 pagesBT 501 Current Final TermsSundus AwanNo ratings yet
- Q SofaDocument9 pagesQ SofadarlingcarvajalduqueNo ratings yet
- Contamination in CosmeticsDocument40 pagesContamination in CosmeticsJulianne MalongNo ratings yet
- Abstract ThesisDocument2 pagesAbstract Thesismail2mnkNo ratings yet
- Kindly Correlate With Clinical FindingsDocument2 pagesKindly Correlate With Clinical FindingsAaryaveer KatochNo ratings yet
- Chapter 2 History of MicrobiologyDocument39 pagesChapter 2 History of MicrobiologyChristian AbordoNo ratings yet
- Avoid Flu Shots, Take Vitamin D Instead by Donald W. Miller, JR., MDDocument11 pagesAvoid Flu Shots, Take Vitamin D Instead by Donald W. Miller, JR., MDmohankurianNo ratings yet
- MMR Vaccine Dosage, Administration, and Nursing ResponsibilitiesDocument2 pagesMMR Vaccine Dosage, Administration, and Nursing ResponsibilitiesErika Marie Calucab100% (2)