You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Status of BJMPDocument104 pagesStatus of BJMParlene palasico85% (13)
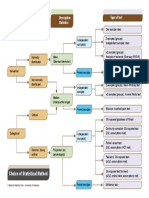
- Choice of Statistical Method Flow DiagramDocument1 pageChoice of Statistical Method Flow DiagramAhmed Adel RagabNo ratings yet
- Evaluating The Training Effects of Two Swallowing Rehabilitation Therapies Using Surface ElectromyographyDocument11 pagesEvaluating The Training Effects of Two Swallowing Rehabilitation Therapies Using Surface ElectromyographyTahysse Andrea Varela SilvaNo ratings yet
- Chin Tuck Against Resistance (CTAR) - New Method For Enhancing Suprahyoid Muscle Activity Using A Shaker-Type ExerciseDocument6 pagesChin Tuck Against Resistance (CTAR) - New Method For Enhancing Suprahyoid Muscle Activity Using A Shaker-Type ExerciseTahysse Andrea Varela SilvaNo ratings yet
- Dysphagia in The Elderly Ianessa A. Humbert, PhDa and JoAnne Robbins, PHDB, CDocument13 pagesDysphagia in The Elderly Ianessa A. Humbert, PhDa and JoAnne Robbins, PHDB, CTahysse Andrea Varela SilvaNo ratings yet
- Colocación de Los ElectrodosDocument8 pagesColocación de Los ElectrodosTahysse Andrea Varela SilvaNo ratings yet
- Aphasia and Aphasic Syndromes, Neurourology Rehabilitation PDFDocument19 pagesAphasia and Aphasic Syndromes, Neurourology Rehabilitation PDFTahysse Andrea Varela SilvaNo ratings yet
- Original Article: Influence of Nutritional Education On Hemodialysis Patients'Document6 pagesOriginal Article: Influence of Nutritional Education On Hemodialysis Patients'Annis FathiaNo ratings yet
- Artikel Jurnal AfifDocument7 pagesArtikel Jurnal AfifDiana Khoirunning TiasNo ratings yet
- Chapter 3Document7 pagesChapter 3Marvinel VinuyaNo ratings yet
- Unit 8 Infrential Statistics AnovaDocument10 pagesUnit 8 Infrential Statistics AnovaHafizAhmadNo ratings yet
- Impact of Maternal Employment On The Growth and Development Among Children at Selected Schools of KolhapurDocument7 pagesImpact of Maternal Employment On The Growth and Development Among Children at Selected Schools of KolhapurJankiNo ratings yet
- Using Background Music To Affect The Behavior of Supermarket ShoppersDocument7 pagesUsing Background Music To Affect The Behavior of Supermarket ShoppersIulian BogdanNo ratings yet
- Alarape and NassarDocument22 pagesAlarape and NassarAderemi AlarapeNo ratings yet
- Factors Affecting Students' Academic Performance in Mathematical Sciences Department in Tertiary Institutions in NigeriaDocument9 pagesFactors Affecting Students' Academic Performance in Mathematical Sciences Department in Tertiary Institutions in NigeriaEducationdavid100% (1)
- Camote Vinegar1Document19 pagesCamote Vinegar1EZLIN JETH PACPACONGNo ratings yet
- Impression ManagementDocument96 pagesImpression ManagementS.khanNo ratings yet
- Text RecountDocument4 pagesText Recountabtiar27No ratings yet
- Stat982 (Chap13) Q SetDocument27 pagesStat982 (Chap13) Q SetgauravNo ratings yet
- Spss Intro TasksDocument7 pagesSpss Intro TasksFrederick PatacsilNo ratings yet
- Nyabwanga Et Al 2013Document16 pagesNyabwanga Et Al 2013Robert Nyamao NyabwangaNo ratings yet
- Hypothesis Testing (Lecture) PDFDocument50 pagesHypothesis Testing (Lecture) PDFSour Wolf50% (2)
- Making Location Quotients More Relevant As A Policy Aid in Regional Spatial AnalysisDocument16 pagesMaking Location Quotients More Relevant As A Policy Aid in Regional Spatial Analysiswahyu wahyudiNo ratings yet
- Report FormatDocument2 pagesReport FormatYousouf Iqbal100% (1)
- Three-Dimensional Upper-Airway Assessment in Patients With Bronchial AsthmaDocument6 pagesThree-Dimensional Upper-Airway Assessment in Patients With Bronchial AsthmaAli mahieddine BoudiaNo ratings yet
- Tutorial Stata PDFDocument22 pagesTutorial Stata PDFRuslan UlanNo ratings yet
- Effect of Knowledge Management Systems On Operating Performance An Empirical Study of Hi Tech Companies Using The Balanced Scorecard ApproachDocument11 pagesEffect of Knowledge Management Systems On Operating Performance An Empirical Study of Hi Tech Companies Using The Balanced Scorecard Approachمهنوش جوادی پورفرNo ratings yet
- Farm Power and Machinery1Document108 pagesFarm Power and Machinery1Manish PandeyNo ratings yet
- PARAMETRIC TESTDocument49 pagesPARAMETRIC TESTsuganthi rajesh kannaNo ratings yet
- Kalasalingam Academy of Research and Education Office of The Controller of ExaminationsDocument87 pagesKalasalingam Academy of Research and Education Office of The Controller of ExaminationsifthisamNo ratings yet
- Lab RecordDocument59 pagesLab RecordRuban KumarNo ratings yet
- Kremelberg CH 1Document11 pagesKremelberg CH 1AsheleyNo ratings yet
- F DistributionDocument16 pagesF DistributionreviewamitNo ratings yet
- Guidance Needs of Nursing Students in Iloilo CityDocument13 pagesGuidance Needs of Nursing Students in Iloilo CityRyan Michael OducadoNo ratings yet
- Handbook For RC Research RevisedDocument346 pagesHandbook For RC Research RevisedFabio TullioNo ratings yet