You might also like
- 1 s2.0 S0094114X17302252 MainDocument23 pages1 s2.0 S0094114X17302252 MainKaviraj SenguntharNo ratings yet
- Bio-Inspired Design of A Self-Aligning, Lightweight, and Highly-Compliant Cable-Driven Knee ExoskeletonDocument14 pagesBio-Inspired Design of A Self-Aligning, Lightweight, and Highly-Compliant Cable-Driven Knee ExoskeletonJony WalkerNo ratings yet
- Chen 2017 A Wearable Exoskeleton Suit For MotDocument12 pagesChen 2017 A Wearable Exoskeleton Suit For MotJUAN RICARDO CASTAÑEDA BELTRANNo ratings yet
- Mechanical Design of Knee and Ankle Exoskeleton To Help Patients With Lower Limb DisabilitiesDocument12 pagesMechanical Design of Knee and Ankle Exoskeleton To Help Patients With Lower Limb Disabilitiesbetelhemterefe wondimagenihuNo ratings yet
- Micromachines 2544656 Peer Review v1Document21 pagesMicromachines 2544656 Peer Review v1Parvin AkterNo ratings yet
- Effectiveness of Robotic Exoskeletons For Improving Gait in Children With Cerebral Palsy - A Systematic ReviewDocument12 pagesEffectiveness of Robotic Exoskeletons For Improving Gait in Children With Cerebral Palsy - A Systematic ReviewAkim KbNo ratings yet
- 2020 Siviy Ieee Ral - Offline Assistance Optimization of A Soft Exosuit For Augmenting Ankle Power of Stroke Survivors During Walking PDFDocument8 pages2020 Siviy Ieee Ral - Offline Assistance Optimization of A Soft Exosuit For Augmenting Ankle Power of Stroke Survivors During Walking PDFSai AravindNo ratings yet
- 2016 Summary of Human AnkleDocument7 pages2016 Summary of Human AnkleJhon Michel Diaz LozanoNo ratings yet
- Journal of Biomechanics: Josh R. Baxter, Todd J. Hullfish, Wen ChaoDocument5 pagesJournal of Biomechanics: Josh R. Baxter, Todd J. Hullfish, Wen ChaoEma.diazNo ratings yet
- Limited Rotation of The 3-44Document6 pagesLimited Rotation of The 3-44HAKAN PARNo ratings yet
- State-Of-The-Art Research in Robotic Hip Exoskeletons A General ReviewDocument10 pagesState-Of-The-Art Research in Robotic Hip Exoskeletons A General Reviewahmad joharaNo ratings yet
- Reducing Circumduction and Hip Hiking During Hemiparetic Walking Through Targeted Assistance of The Paretic Limb Using A Soft Robotic ExosuitDocument8 pagesReducing Circumduction and Hip Hiking During Hemiparetic Walking Through Targeted Assistance of The Paretic Limb Using A Soft Robotic ExosuitExternalNo ratings yet
- Design and Control of A Wearable Active Knee Orthosis For Walking AssistanceDocument6 pagesDesign and Control of A Wearable Active Knee Orthosis For Walking AssistanceEpitácio FariasNo ratings yet
- Design and Control of A Lower Limb Exoskeleton For Robot-Assisted Gait TrainingDocument16 pagesDesign and Control of A Lower Limb Exoskeleton For Robot-Assisted Gait TrainingYalçın SabihaNo ratings yet
- Walking Simulation Model of Lower Limb Exoskeleton Robot DesignDocument11 pagesWalking Simulation Model of Lower Limb Exoskeleton Robot Designandersson benito herrera100% (1)
- Biomechanical Evaluation of Exoskeleton Use On Loading of The Lumbar SpineDocument8 pagesBiomechanical Evaluation of Exoskeleton Use On Loading of The Lumbar SpineJuan Carlos VelasquezNo ratings yet
- Analysis of The Gait Characteristics and Usability After Wearable Exoskeleton Robot Gait TrainingDocument10 pagesAnalysis of The Gait Characteristics and Usability After Wearable Exoskeleton Robot Gait TrainingAnis AnwasNo ratings yet
- Research Article: Pilot Study of A Powered Exoskeleton For Upper Limb Rehabilitation Based On The WheelchairDocument12 pagesResearch Article: Pilot Study of A Powered Exoskeleton For Upper Limb Rehabilitation Based On The WheelchairCostinel BogheanuNo ratings yet
- 1.exoskeletons For Gait Assistance and Training of The MotorImpaired 2007Document6 pages1.exoskeletons For Gait Assistance and Training of The MotorImpaired 2007Gullipalli Praveen Uday KiranNo ratings yet
- Journal of Neuroengineering and RehabilitationDocument16 pagesJournal of Neuroengineering and RehabilitationFikri DzakyNo ratings yet
- Preliminary Evaluation of A Powered Lower Limb Orthosis To Aid Walking in Paraplegic IndividualsDocument8 pagesPreliminary Evaluation of A Powered Lower Limb Orthosis To Aid Walking in Paraplegic IndividualsCarmen Cuerdo del RíoNo ratings yet
- Design and Control of A Parallel Robot For Ankle RehabilitationDocument14 pagesDesign and Control of A Parallel Robot For Ankle RehabilitationSushi RollNo ratings yet
- Granacheretal.2012 Gerontol CoreDocument9 pagesGranacheretal.2012 Gerontol CoreBaba DookNo ratings yet
- Protesis 13Document9 pagesProtesis 13ana márquezNo ratings yet
- Accepted ManuscriptDocument40 pagesAccepted ManuscriptDaniel CarcamoNo ratings yet
- 1 s2.0 S0921889022000392 MainDocument11 pages1 s2.0 S0921889022000392 MainNANDHINIK 19BM059No ratings yet
- Efficacy of A Hybrid Assistive Limb in Post-Stroke Hemiplegic Patients: A Preliminary ReportDocument6 pagesEfficacy of A Hybrid Assistive Limb in Post-Stroke Hemiplegic Patients: A Preliminary ReportJoão Pedro Lemos MoraisNo ratings yet
- Plagiarized First 1reportDocument39 pagesPlagiarized First 1reportAbdul RabbaniNo ratings yet
- Robot-Assisted Ankle Rehabilitation For The Treatment of Drop Foot: A Case StudyDocument5 pagesRobot-Assisted Ankle Rehabilitation For The Treatment of Drop Foot: A Case StudyIhsanNo ratings yet
- Exoskeletons and Orthoses: Classification, Design Challenges and Future DirectionsDocument10 pagesExoskeletons and Orthoses: Classification, Design Challenges and Future Directionspablo261992No ratings yet
- Exoskeleton Design For LegDocument8 pagesExoskeleton Design For LegGamini SureshNo ratings yet
- Role of Gait Kinematics in Lumbopelvic Exoskeleton Revieiw PaperDocument10 pagesRole of Gait Kinematics in Lumbopelvic Exoskeleton Revieiw PaperPranav karnNo ratings yet
- Applsci 11 03114 v2Document21 pagesApplsci 11 03114 v2IoNo ratings yet
- Actuators: Design and Implementation of A Robotic Hip Exoskeleton For Gait RehabilitationDocument20 pagesActuators: Design and Implementation of A Robotic Hip Exoskeleton For Gait Rehabilitationbetelhemterefe wondimagenihuNo ratings yet
- The Effects of Total Ankle Replacement On Ankle J - 2017 - Journal of Sport andDocument6 pagesThe Effects of Total Ankle Replacement On Ankle J - 2017 - Journal of Sport andSisi WeeraNo ratings yet
- Transitions Sit To Stand and Stand To Sit in Persons Post-Stroke Path of Centre of Mass, Pelvic and Limb Loading - A Pilot StudyDocument9 pagesTransitions Sit To Stand and Stand To Sit in Persons Post-Stroke Path of Centre of Mass, Pelvic and Limb Loading - A Pilot Studytorrischan199No ratings yet
- An Exploration of The Function of The Triceps Surae During Normal Gait Using Functional Electrical StimulationDocument7 pagesAn Exploration of The Function of The Triceps Surae During Normal Gait Using Functional Electrical StimulationValentinus Adi PamungkasNo ratings yet
- Application of Wearable Sensors in Actuation and Control of Powered Ankle Exoskeletons A Comprehensive Review - Sensors-22-02244Document5 pagesApplication of Wearable Sensors in Actuation and Control of Powered Ankle Exoskeletons A Comprehensive Review - Sensors-22-02244Generation GenerationNo ratings yet
- Kinematic and Kinetic Functional RequirementsgDocument28 pagesKinematic and Kinetic Functional RequirementsgMabel PNo ratings yet
- Koop Man 2014Document12 pagesKoop Man 2014Elizabeth CominaNo ratings yet
- Huysamenetal 2018passiveexofinalDocument8 pagesHuysamenetal 2018passiveexofinalTest channelNo ratings yet
- Applied SciencesDocument22 pagesApplied SciencesHamrah SiddiquiNo ratings yet
- Estimation of Two Wear Factors For Total Hip ArthrDocument8 pagesEstimation of Two Wear Factors For Total Hip ArthrMauricio MoncadaNo ratings yet
- Halonen 2016Document32 pagesHalonen 2016sina salehpourNo ratings yet
- Is There A Relationship Between Back Squat Depth, Ankle Flexibility, and Achilles Tendon Stiffness?Document15 pagesIs There A Relationship Between Back Squat Depth, Ankle Flexibility, and Achilles Tendon Stiffness?adindaNo ratings yet
- Experimental Evaluation of A Shoulder-Support Exoskeleton For Overhead Work: Influences of Peak Torque Amplitude, Task, and Tool MassDocument15 pagesExperimental Evaluation of A Shoulder-Support Exoskeleton For Overhead Work: Influences of Peak Torque Amplitude, Task, and Tool MassValentina PetkoffNo ratings yet
- 2018 Article 642Document14 pages2018 Article 642Faqih FathurrozanNo ratings yet
- PIIS2352344120300613Document5 pagesPIIS2352344120300613yu prdnyaNo ratings yet
- Novel Soft Bending Actuator-Based Power Augmentation Hand Exoskeleton Controlled by Human IntentionDocument22 pagesNovel Soft Bending Actuator-Based Power Augmentation Hand Exoskeleton Controlled by Human IntentionAlemeNo ratings yet
- Research On A New Rehabilitation Robot For Balance DisordersDocument10 pagesResearch On A New Rehabilitation Robot For Balance DisordersSyed MoinuddinNo ratings yet
- Eng VersionDocument10 pagesEng VersionShania BaraqbahNo ratings yet
- PANTOE 1-Biomechanical Design of Powered Ankle-Foot Prosthesis With Compliant Joints and Segmented FootDocument6 pagesPANTOE 1-Biomechanical Design of Powered Ankle-Foot Prosthesis With Compliant Joints and Segmented Footaufar syehanNo ratings yet
- Thebiomechanics of Fixed AnklefootorthosesDocument9 pagesThebiomechanics of Fixed AnklefootorthosesUshsbsNo ratings yet
- Epimuscular Myofascial Force Transmission Between The Levator ScapulaeDocument6 pagesEpimuscular Myofascial Force Transmission Between The Levator ScapulaeNadina WawrzykNo ratings yet
- Gravity-Balancing Leg Orthosis and Its PerformanceDocument13 pagesGravity-Balancing Leg Orthosis and Its Performancejose diazNo ratings yet
- 1 s2.0 S1350453322000790 MainDocument8 pages1 s2.0 S1350453322000790 MainNANDHINIK 19BM059No ratings yet
- Cureus 0013 00000014763Document10 pagesCureus 0013 00000014763aghniajolandaNo ratings yet
- Design and Simulation of Leg-Exoskeleton Suit For RehabilitationDocument8 pagesDesign and Simulation of Leg-Exoskeleton Suit For RehabilitationAlbert ArtandiNo ratings yet
- Powered Ankle Exoskeletons Existent Designs and Control SystemsDocument8 pagesPowered Ankle Exoskeletons Existent Designs and Control SystemsHeeralNo ratings yet
- Accepted Manuscript: Lelai Zhou Yibin Li Shaoping BaiDocument32 pagesAccepted Manuscript: Lelai Zhou Yibin Li Shaoping BaiZehra ÇİFCİBAŞINo ratings yet
- State-Of-The-Art and Future Directions For Lower Limb Robotic ExoskeletonsDocument20 pagesState-Of-The-Art and Future Directions For Lower Limb Robotic ExoskeletonsZehra ÇİFCİBAŞINo ratings yet
- Design and Preliminary Evaluation of A Passive Spine ExoskeletonDocument8 pagesDesign and Preliminary Evaluation of A Passive Spine ExoskeletonZehra ÇİFCİBAŞINo ratings yet
- Robotics and Autonomous Systems: Jafar Kazemi Sadjaad OzgoliDocument23 pagesRobotics and Autonomous Systems: Jafar Kazemi Sadjaad OzgoliZehra ÇİFCİBAŞINo ratings yet
- State of The Art Lower Limb Robotic Exoskeletons For Elderly AssistanceDocument12 pagesState of The Art Lower Limb Robotic Exoskeletons For Elderly AssistanceZehra ÇİFCİBAŞINo ratings yet
- Exoskeleton and End-Effector Robots For Upper and Lower Limbs Rehabilitation: Narrative ReviewDocument15 pagesExoskeleton and End-Effector Robots For Upper and Lower Limbs Rehabilitation: Narrative ReviewZehra ÇİFCİBAŞINo ratings yet
- Simulating Ideal Assistive Devices To Reduce The Metabolic Cost of Walking With Heavy LoadsDocument25 pagesSimulating Ideal Assistive Devices To Reduce The Metabolic Cost of Walking With Heavy LoadsZehra ÇİFCİBAŞINo ratings yet
- On The Kinematic Design of Anthropomorphic Lower Limb Exoskeletons and Their Matching MovementDocument9 pagesOn The Kinematic Design of Anthropomorphic Lower Limb Exoskeletons and Their Matching MovementZehra ÇİFCİBAŞINo ratings yet
- Design and Modeling of A Lightweight and Low Power Consumption Full-Scale Biped RobotDocument32 pagesDesign and Modeling of A Lightweight and Low Power Consumption Full-Scale Biped RobotZehra ÇİFCİBAŞINo ratings yet
- Kinematics Analysis of A 3dof Lower Limb Exoskeleton For Gait Rehabilitation: A Preliminary InvestigationDocument5 pagesKinematics Analysis of A 3dof Lower Limb Exoskeleton For Gait Rehabilitation: A Preliminary InvestigationZehra ÇİFCİBAŞINo ratings yet
- Biomechanics Analysis of Human Lower Limb During Walking For Exoskeleton DesignDocument13 pagesBiomechanics Analysis of Human Lower Limb During Walking For Exoskeleton DesignZehra ÇİFCİBAŞINo ratings yet
- Study On Structural Modeling and Kinematics Analysis of A Novel Wheel-Legged Rescue RobotDocument17 pagesStudy On Structural Modeling and Kinematics Analysis of A Novel Wheel-Legged Rescue RobotZehra ÇİFCİBAŞINo ratings yet
- The Most Compact and Fast Robot EverDocument2 pagesThe Most Compact and Fast Robot EverHADI FETSANo ratings yet
- Why The Future Doesn't Need Us?Document2 pagesWhy The Future Doesn't Need Us?Audrey RNo ratings yet
- Robotics (Edison) - ADocument2 pagesRobotics (Edison) - AAdam shakil0% (1)
- Tablas Mecanicas KR C2 PDFDocument10 pagesTablas Mecanicas KR C2 PDFarturoNo ratings yet
- Solar Floor Cleaner RobotDocument4 pagesSolar Floor Cleaner RobotIJRASETPublicationsNo ratings yet
- In This Lecture We Will Learn About: Module 2: Robots Mechanisms Lecture 5: Manipulators Mechanisms-I ObjectivesDocument3 pagesIn This Lecture We Will Learn About: Module 2: Robots Mechanisms Lecture 5: Manipulators Mechanisms-I ObjectivesNELWIN JONESNo ratings yet
- 03 Hand Rehabilitation of Stroke PatientsDocument6 pages03 Hand Rehabilitation of Stroke PatientsMd. Mizanur RahmanNo ratings yet
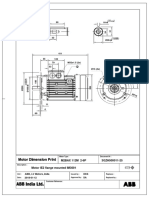
- M2bax112m B5 (3GZH500011-25)Document1 pageM2bax112m B5 (3GZH500011-25)dhanishlNo ratings yet
- Chapter 2 Industrial Robot ApplicationsDocument16 pagesChapter 2 Industrial Robot ApplicationsK T7No ratings yet
- Flower Knitting Machine: International Research Journal of Engineering and Technology (IRJET)Document3 pagesFlower Knitting Machine: International Research Journal of Engineering and Technology (IRJET)aruljeromeNo ratings yet
- Excersise 1Document3 pagesExcersise 1Gabriel Tomagos100% (1)
- Background:: Mind Mapperz and SAITMDocument4 pagesBackground:: Mind Mapperz and SAITMMohit SinghNo ratings yet
- 1.1. A Sense of HistoryDocument8 pages1.1. A Sense of HistoryCarlitos FerNo ratings yet
- 3hac032140 004Document2 pages3hac032140 004zuda.ahamdNo ratings yet
- Peralihan LP 7.10Document1 pagePeralihan LP 7.10MornisaNo ratings yet
- Interesting Inventions: Sophia - A Social Human RobotDocument1 pageInteresting Inventions: Sophia - A Social Human RobotKatinka VermeulenNo ratings yet
- Question Bank PDFDocument4 pagesQuestion Bank PDFOmar MahfouzNo ratings yet
- Smiles 3 Mod Test 1ADocument4 pagesSmiles 3 Mod Test 1ABiljana Nestorovska0% (1)
- Media Backgrounder On Artificial Intelligence in Robotics May 2018Document5 pagesMedia Backgrounder On Artificial Intelligence in Robotics May 2018Sree MahaNo ratings yet
- Instructional Module: Republic of The Philippines Nueva Vizcaya State University Bayombong, Nueva VizcayaDocument6 pagesInstructional Module: Republic of The Philippines Nueva Vizcaya State University Bayombong, Nueva VizcayaMia Pinkihan TayabanNo ratings yet
- Artificial IntelligenceDocument3 pagesArtificial IntelligenceshahNo ratings yet
- ENEE408I - Task DocumentDocument7 pagesENEE408I - Task DocumentpkrepkiyNo ratings yet
- Mothership - Fear Factory V (v1.1) (2020)Document24 pagesMothership - Fear Factory V (v1.1) (2020)Temp Email100% (1)
- Definition of Marketing AspectDocument5 pagesDefinition of Marketing AspectMojan VianaNo ratings yet
- The Article: More Free Lessons at 2Document8 pagesThe Article: More Free Lessons at 2Sonia Del Val CasasNo ratings yet
- Robotics and Automation Lecture PlanDocument1 pageRobotics and Automation Lecture PlanGitu ShivNo ratings yet
- Robotics: Ece 411: Robotics Engr. Lalaine Jean A. Ballais, EctDocument9 pagesRobotics: Ece 411: Robotics Engr. Lalaine Jean A. Ballais, Ecttsk2230No ratings yet
- GF - Robot Legions v2.12Document3 pagesGF - Robot Legions v2.12Tom MuscoNo ratings yet
- Fluid Systems SyllabusDocument2 pagesFluid Systems SyllabusGeetha Sai KumarNo ratings yet
- Peter CapstoneDocument25 pagesPeter Capstoneapi-572616300No ratings yet