You might also like
- The Desk Jockey's Manifesto: The Practical Guide for Modern Computer/Desk WorkerFrom EverandThe Desk Jockey's Manifesto: The Practical Guide for Modern Computer/Desk WorkerNo ratings yet
- Progress Test 3 (Units 5-6) : Name: - Date: - Section 1: VocabularyDocument3 pagesProgress Test 3 (Units 5-6) : Name: - Date: - Section 1: VocabularyPaulina CardinaleNo ratings yet
- VE EFN1 Tests ProgressTest03Document3 pagesVE EFN1 Tests ProgressTest03ivan.n.stanimirovicNo ratings yet
- Permanent Disability FormDocument4 pagesPermanent Disability FormTracey MitchellNo ratings yet
- Proton Beam Radiation Therapy Physician Worksheet: Provider InformationDocument3 pagesProton Beam Radiation Therapy Physician Worksheet: Provider InformationShNo ratings yet
- Abdominal Scar MassageDocument6 pagesAbdominal Scar MassageRekha Satheesan100% (1)
- MAPEH (P.E.) : Quarter 1 - Module 1: Sports Officiating: First Aid (Cramps, Sprains, and Strains)Document11 pagesMAPEH (P.E.) : Quarter 1 - Module 1: Sports Officiating: First Aid (Cramps, Sprains, and Strains)Albert Ian CasugaNo ratings yet
- Plastic Surgery Volunteer ApplicationDocument8 pagesPlastic Surgery Volunteer ApplicationKartika LilisantosaNo ratings yet
- Triage in Emergency Department Using ESi (5 Levels) Self Study 8.2015 in PDF Format For Email and PostingDocument52 pagesTriage in Emergency Department Using ESi (5 Levels) Self Study 8.2015 in PDF Format For Email and Postingdian prawita100% (1)
- CT Scan Ref-Brampton CivicDocument1 pageCT Scan Ref-Brampton CivicalikuniNo ratings yet
- UOI Diploma Admission DetailsDocument4 pagesUOI Diploma Admission DetailsHaason TzNo ratings yet
- 5 Senses Guide to Understanding How Humans Perceive WorldDocument20 pages5 Senses Guide to Understanding How Humans Perceive WorldCtea AMinaNo ratings yet
- RF Rizotomy-1Document4 pagesRF Rizotomy-1Deepu NairNo ratings yet
- Back Pain Follow-UpDocument3 pagesBack Pain Follow-Upbarros6No ratings yet
- Spine Questionnaire Weill CornellDocument8 pagesSpine Questionnaire Weill CornellroxieNo ratings yet
- UoI Certificate Joining Instruction 2020 21Document4 pagesUoI Certificate Joining Instruction 2020 21Haason TzNo ratings yet
- Assessment Performa Date of AssessmentDocument12 pagesAssessment Performa Date of AssessmentAtu KaushalNo ratings yet
- Migrant Health FormDocument5 pagesMigrant Health FormImelda Junaedi100% (3)
- Spep Orpington ScaleDocument1 pageSpep Orpington ScaleM Isyhaduul IslamNo ratings yet
- Client Initial Assessment Worksheet: How Did You Here About Us or Who Referred You?Document5 pagesClient Initial Assessment Worksheet: How Did You Here About Us or Who Referred You?api-335005776No ratings yet
- 600 - ICD-10-CM Medical Diagnostic Coding - R - 2021Document3 pages600 - ICD-10-CM Medical Diagnostic Coding - R - 2021balumthomasNo ratings yet
- Tèm Ko Moun FinalDocument9 pagesTèm Ko Moun FinalFleury FenoldNo ratings yet
- Community Health Nursing Case Study: 2-Year-Old Boy with Fever and RashDocument5 pagesCommunity Health Nursing Case Study: 2-Year-Old Boy with Fever and RashIsaiah RabangNo ratings yet
- PTAP Practical Exam SOAP NoteDocument3 pagesPTAP Practical Exam SOAP NotelycanwarsNo ratings yet
- Cellular Respiration ActivityDocument4 pagesCellular Respiration Activitylamouna.lamittaNo ratings yet
- Claim Form DentalDocument2 pagesClaim Form DentalChloe MirandaNo ratings yet
- Dole/BWC/HSD/OH-47-A Annual Medical Report FormDocument5 pagesDole/BWC/HSD/OH-47-A Annual Medical Report FormHR ZMCNo ratings yet
- Data Collection Sheets For SIGN Online Surgical DatabaseDocument6 pagesData Collection Sheets For SIGN Online Surgical Databaseasi basseyNo ratings yet
- IMCI Form2Document18 pagesIMCI Form2Cristina Bantilan MontenegroNo ratings yet
- Kathryn Rossi-MBT-T Group ProtocolDocument1 pageKathryn Rossi-MBT-T Group ProtocolMona DiezmiltaoNo ratings yet
- NEW General Immunization FormDocument3 pagesNEW General Immunization FormLuisa PataganNo ratings yet
- Appendix 2: Evaluation Form For The Acquired Monocular Vision PatientDocument2 pagesAppendix 2: Evaluation Form For The Acquired Monocular Vision PatientEvelyn SepulvedaNo ratings yet
- PT Initial EvaluationDocument11 pagesPT Initial EvaluationSumbul JakhuraNo ratings yet
- EMDR WORKSHEET GUIDEDocument3 pagesEMDR WORKSHEET GUIDEKONSELOR SMAGLORIA2No ratings yet
- EM Coding GuidelinesDocument2 pagesEM Coding Guidelineskar883100% (2)
- HEAS Head To Toe Reassessment 2021Document3 pagesHEAS Head To Toe Reassessment 2021Gracia MungalaNo ratings yet
- Diabetic Evaluation (Adults Only) : Form To Be Completed by StudentDocument2 pagesDiabetic Evaluation (Adults Only) : Form To Be Completed by StudentNabeel ShahzadNo ratings yet
- 1 Module 1 q1 General Physics 1Document17 pages1 Module 1 q1 General Physics 1ChandaNo ratings yet
- Newsletter - Rob S Vol 4 April 2015Document7 pagesNewsletter - Rob S Vol 4 April 2015api-323491985No ratings yet
- Shoulder Pain and Disability Index (SPADI)Document2 pagesShoulder Pain and Disability Index (SPADI)RizkiA.BinandraPutraNo ratings yet
- Shoulder Pain Index for Assessing DisabilityDocument2 pagesShoulder Pain Index for Assessing DisabilityLindaPramusintaNo ratings yet
- Study Group MFM: Motor Function Measure For Neuromuscular DisordersDocument10 pagesStudy Group MFM: Motor Function Measure For Neuromuscular DisordersReny Wahyu SariNo ratings yet
- Or Checklist of RequirementsDocument4 pagesOr Checklist of RequirementsJulianne MagtunaoNo ratings yet
- Cervical AssesmentDocument3 pagesCervical Assesmentahmadkiblawi884No ratings yet
- Outpatient Rehab Adult Physical Therapy Medical HistoryDocument2 pagesOutpatient Rehab Adult Physical Therapy Medical HistorySid Ki AnuNo ratings yet
- Frog Dissection Pre Lab 2Document4 pagesFrog Dissection Pre Lab 2bondwilderNo ratings yet
- Intake Form 2020 OctDocument7 pagesIntake Form 2020 Octapi-277069774No ratings yet
- UOI Medical FormDocument2 pagesUOI Medical FormHaason TzNo ratings yet
- Rapid3 FormatoDocument2 pagesRapid3 FormatoVioleta Madrigal PérezNo ratings yet
- Providence WC Clinic Referral FormDocument3 pagesProvidence WC Clinic Referral FormlisamaurerNo ratings yet
- MRI Safety FormDocument2 pagesMRI Safety Formpep pepeNo ratings yet
- Mohindra Retinoscopy LabDocument1 pageMohindra Retinoscopy LabJoseph NayfachNo ratings yet
- P7 - Lab 5 Muscular Strength and Endurance: ObjectiveDocument10 pagesP7 - Lab 5 Muscular Strength and Endurance: ObjectiveSarn Yung-HonNo ratings yet
- Orthopedic Clerking TemplateDocument4 pagesOrthopedic Clerking TemplateNur Liyana Ahmad ZakiNo ratings yet
- Pineda, Dona Ysabel - BAPS 1-2Document6 pagesPineda, Dona Ysabel - BAPS 1-2Dys MatiasNo ratings yet
- 05-NIH Stroke ScaleDocument11 pages05-NIH Stroke ScaleMus TikaNo ratings yet
- Free Medical Coding Course PDFDocument7 pagesFree Medical Coding Course PDFSrinivasa Reddy Reddys75% (4)
- Nano ImplantsDocument13 pagesNano ImplantsBraulio MenezesNo ratings yet
- Knee Clinic Intake Forms 2013Document4 pagesKnee Clinic Intake Forms 2013Dr. Dale MacdonaldNo ratings yet
- Angela Roll-Up Pencil CaseDocument5 pagesAngela Roll-Up Pencil CaseNeptune ShellNo ratings yet
- Curatorcoloringbook PDFDocument14 pagesCuratorcoloringbook PDFNeptune ShellNo ratings yet
- Treetop Savers Rewards Colour PDFDocument1 pageTreetop Savers Rewards Colour PDFNeptune ShellNo ratings yet
- 39 Storey Treehouse Activity Pack PDFDocument11 pages39 Storey Treehouse Activity Pack PDFNeptune Shell0% (3)
- Color+Jupiter A+Swirling+Storm PDFDocument1 pageColor+Jupiter A+Swirling+Storm PDFNeptune ShellNo ratings yet
- Scar Release Therapy Brochure April 25 2018 PDFDocument8 pagesScar Release Therapy Brochure April 25 2018 PDFNeptune ShellNo ratings yet
- Fibromyalgia Fact Sheet PDFDocument1 pageFibromyalgia Fact Sheet PDFShahada DeeNo ratings yet
- FibrobookletDocument24 pagesFibrobookletNeptune ShellNo ratings yet
- Soc C115 and Public Health C155 Syllabus and Schedule Spring 14Document8 pagesSoc C115 and Public Health C155 Syllabus and Schedule Spring 14Neptune ShellNo ratings yet
- Dolphin Neurostim Brochure Professional Web PDFDocument2 pagesDolphin Neurostim Brochure Professional Web PDFNeptune ShellNo ratings yet
- CNT 0023993 01 PDFDocument4 pagesCNT 0023993 01 PDFNeptune ShellNo ratings yet
- Scar Release Therapy Brochure April 25 2018 PDFDocument8 pagesScar Release Therapy Brochure April 25 2018 PDFNeptune ShellNo ratings yet
- Patient Consent Form for E-Stim TreatmentDocument1 pagePatient Consent Form for E-Stim TreatmentNeptune ShellNo ratings yet
- MPS Concussion Flip Book April 12 2018Document7 pagesMPS Concussion Flip Book April 12 2018Neptune ShellNo ratings yet
- Dolphin Neurostim Brochure Patient Web PDFDocument2 pagesDolphin Neurostim Brochure Patient Web PDFNeptune ShellNo ratings yet
- MPS Therapy Flyer April 10 2018Document8 pagesMPS Therapy Flyer April 10 2018Neptune ShellNo ratings yet
- Tōhō Project and Its Connections With Classical Aspects of Folklore and Culture of JapanDocument66 pagesTōhō Project and Its Connections With Classical Aspects of Folklore and Culture of JapanChiaki HiraiNo ratings yet
- Biography PDFDocument1 pageBiography PDFNeptune ShellNo ratings yet
- Fibromyalgia PDFDocument85 pagesFibromyalgia PDFNeptune ShellNo ratings yet
- Biography PDFDocument1 pageBiography PDFNeptune ShellNo ratings yet
- Biography PDFDocument1 pageBiography PDFNeptune ShellNo ratings yet
- District Wise List of Colleges Under The Juridiction of MRSPTU BathindaDocument13 pagesDistrict Wise List of Colleges Under The Juridiction of MRSPTU BathindaGurpreet SandhuNo ratings yet
- Agilent Cool On-Column Operation ManualDocument42 pagesAgilent Cool On-Column Operation Manualdmcevoy1965No ratings yet
- Ek Pardesi Mera Dil Le Gaya Lyrics English Translation - Lyrics GemDocument1 pageEk Pardesi Mera Dil Le Gaya Lyrics English Translation - Lyrics Gemmahsa.molaiepanahNo ratings yet
- K230F Equipment ManualsDocument166 pagesK230F Equipment ManualsHui ChenNo ratings yet
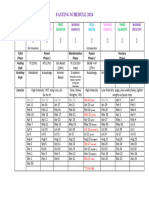
- Moon Fast Schedule 2024Document1 pageMoon Fast Schedule 2024mimiemendoza18No ratings yet
- Abbreviation Meaning Notes: Cibo ("With Food")Document4 pagesAbbreviation Meaning Notes: Cibo ("With Food")TantriNo ratings yet
- mcs2019 All PDFDocument204 pagesmcs2019 All PDFRheydel BartolomeNo ratings yet
- Icelandic Spells and SigilsDocument16 pagesIcelandic Spells and SigilsSimonida Mona Vulić83% (6)
- Design & Construction of Substation 16P Painting System ComplianceDocument103 pagesDesign & Construction of Substation 16P Painting System ComplianceRamil LazNo ratings yet
- 20ME901 Automobile Engineering Unit 3Document74 pages20ME901 Automobile Engineering Unit 36044 sriramNo ratings yet
- Service Positioning and DesignDocument3 pagesService Positioning and DesignSaurabh SinhaNo ratings yet
- Eagle Test ReportDocument25 pagesEagle Test ReportMuhammad FahadNo ratings yet
- PAPERBOARD QUALITYDocument8 pagesPAPERBOARD QUALITYaurelia carinaNo ratings yet
- The Interview: P F T IDocument14 pagesThe Interview: P F T IkkkkccccNo ratings yet
- PedigreesDocument5 pagesPedigreestpn72hjg88No ratings yet
- 2010 HSC Exam PhysicsDocument42 pages2010 HSC Exam PhysicsVictor345No ratings yet
- DCAD OverviewDocument9 pagesDCAD OverviewSue KimNo ratings yet
- Athenaze 1 Chapter 7a Jun 18th 2145Document3 pagesAthenaze 1 Chapter 7a Jun 18th 2145maverickpussNo ratings yet
- Pure and Applied Analysis Problems Solved Step-by-StepDocument8 pagesPure and Applied Analysis Problems Solved Step-by-Stepalpha2122No ratings yet
- SeparatorDocument2 pagesSeparatormmk111No ratings yet
- ClientsDocument7 pagesClientsLiane PanahacNo ratings yet
- Copy Resit APLC MiniAssignmentDocument5 pagesCopy Resit APLC MiniAssignmentChong yaoNo ratings yet
- Cyber Security 2017Document8 pagesCyber Security 2017Anonymous i1ClcyNo ratings yet
- Lecture 29: Curl, Divergence and FluxDocument2 pagesLecture 29: Curl, Divergence and FluxKen LimoNo ratings yet
- Reversing a String in 8086 Micro Project ReportDocument4 pagesReversing a String in 8086 Micro Project ReportOm IngleNo ratings yet
- OPHTHALDocument8 pagesOPHTHALVarun ChandiramaniNo ratings yet
- Class 7thDocument24 pagesClass 7thPriyaNo ratings yet
- 99th Indian Science Congress (Bhubaneshwar)Document95 pages99th Indian Science Congress (Bhubaneshwar)Aadarsh DasNo ratings yet
- Siga-Cc1 12-22-2010Document6 pagesSiga-Cc1 12-22-2010Felipe LozanoNo ratings yet
- Evolution Packet FinalDocument24 pagesEvolution Packet FinalJoaquinNo ratings yet