You might also like
- Terapia Dirigida Por Metas en Cirugía Cardíaca Lobdell2020Document10 pagesTerapia Dirigida Por Metas en Cirugía Cardíaca Lobdell2020Juan Guillermo BuitragoNo ratings yet
- Tasa de Mortalidad en COVID19Document4 pagesTasa de Mortalidad en COVID19Juan Guillermo BuitragoNo ratings yet
- Supresiòn de SARScoV2 en La Municipalidad de Vo Lavezzo2020Document19 pagesSupresiòn de SARScoV2 en La Municipalidad de Vo Lavezzo2020Juan Guillermo BuitragoNo ratings yet
- Sìndrome de Dificultad Respiratoria Aguda Por Coronavirus Jasper Chan Journal MicrobiologyDocument58 pagesSìndrome de Dificultad Respiratoria Aguda Por Coronavirus Jasper Chan Journal MicrobiologyJuan Guillermo BuitragoNo ratings yet
- Embarazo Infección Viral y COVID 2020Document12 pagesEmbarazo Infección Viral y COVID 2020Juan Guillermo BuitragoNo ratings yet
- Embrazo en La ERA COVID 2020Document25 pagesEmbrazo en La ERA COVID 2020Juan Guillermo BuitragoNo ratings yet
- ExpertConsensus ResuscitationAfterCardiacSurgery PDFDocument16 pagesExpertConsensus ResuscitationAfterCardiacSurgery PDFJuan Guillermo BuitragoNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5796)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- C Outline Drawing: Powerex, Inc., 200 Hillis Street, Youngwood, Pennsylvania 15697-1800 (724) 925-7272Document4 pagesC Outline Drawing: Powerex, Inc., 200 Hillis Street, Youngwood, Pennsylvania 15697-1800 (724) 925-7272lgrome73No ratings yet
- BMEF17M001 ICE Assignment 2Document9 pagesBMEF17M001 ICE Assignment 2Muhammad Javed IqbalNo ratings yet
- Marketing Plan TomgutsDocument9 pagesMarketing Plan TomgutsPinky DaisiesNo ratings yet
- CIVE378 Exam1 ReviewDocument2 pagesCIVE378 Exam1 ReviewJoshtion ShahNo ratings yet
- 2009 Annual Flood Report of FFCDocument44 pages2009 Annual Flood Report of FFCshadi khanNo ratings yet
- Bridging The Gap How Community Health Workers Promote The Health of ImmigrantsDocument257 pagesBridging The Gap How Community Health Workers Promote The Health of ImmigrantsNidaUlfahNo ratings yet
- 3 - PorphyriasDocument14 pages3 - PorphyriasHamzehNo ratings yet
- OK 67.70 ESAB 309moDocument1 pageOK 67.70 ESAB 309moSadashiva sahooNo ratings yet
- GCQRI Lit ReviewDocument18 pagesGCQRI Lit ReviewgcqriNo ratings yet
- The Factories Act, 1948Document60 pagesThe Factories Act, 1948Pavan RaiNo ratings yet
- Laporan Case Mix Gabungantgl 27-12-2023Document191 pagesLaporan Case Mix Gabungantgl 27-12-2023Adhita Septianty ningrumNo ratings yet
- IS Code Based-QuestionsDocument27 pagesIS Code Based-QuestionsGURIJALA UJWAL KUMARNo ratings yet
- ProdrugDocument26 pagesProdrugJittu ReddyNo ratings yet
- South 4Document24 pagesSouth 4LariNo ratings yet
- Código de Erro Statim G4Document5 pagesCódigo de Erro Statim G4Rafael OliveiraNo ratings yet
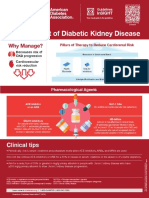
- Management of Diabetic Kidney Disease Updated 0Document1 pageManagement of Diabetic Kidney Disease Updated 0Jia-PeiWuNo ratings yet
- Taste and SmellDocument22 pagesTaste and SmellabdirizakNo ratings yet
- Roman Catholic: Lucena City, PHDocument4 pagesRoman Catholic: Lucena City, PHJennet RiveraNo ratings yet
- 7 Days of Defining Moments: Chip Heath & Dan HeathDocument10 pages7 Days of Defining Moments: Chip Heath & Dan Heaththeowensgroup100% (1)
- Design & Fabrication of Bio Fertilizer Making Machine Using Agricultural WasteDocument2 pagesDesign & Fabrication of Bio Fertilizer Making Machine Using Agricultural WasteInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- ISSF The Ferritic Solution EnglishDocument68 pagesISSF The Ferritic Solution EnglishdhurushaNo ratings yet
- Blue Mind - The Surprising Science That Shows How Being Near, In, On, or Under Water Can Make You Happier, Healthier, More Connected, and Better at What You Do (PDFDrive)Document246 pagesBlue Mind - The Surprising Science That Shows How Being Near, In, On, or Under Water Can Make You Happier, Healthier, More Connected, and Better at What You Do (PDFDrive)Saddam Akbar100% (5)
- Pelaez Gabriella M5A1Document3 pagesPelaez Gabriella M5A1Gabriella PelaezNo ratings yet
- Executive: Carbonated Soft Drinks: Incl Impact of Covid-19Document7 pagesExecutive: Carbonated Soft Drinks: Incl Impact of Covid-19Aasish MuchalaNo ratings yet
- Energy Sav HVAC SystemDocument16 pagesEnergy Sav HVAC SystemrapidSHVNo ratings yet
- Seminar Kimia SPM Mmu 2017 CG Adura Jawapan Kertas 2 PDFDocument48 pagesSeminar Kimia SPM Mmu 2017 CG Adura Jawapan Kertas 2 PDFNoorleha Mohd YusoffNo ratings yet
- Falling Water: Concrete and Rough Stones On Frank Llyod Wright'S Kaufman HouseDocument7 pagesFalling Water: Concrete and Rough Stones On Frank Llyod Wright'S Kaufman HouseSophia Nicole ReytosNo ratings yet
- 2 - 1D Conduction Eq.Document88 pages2 - 1D Conduction Eq.AhmedNo ratings yet
- PC 1 FlowAssurance PDFDocument21 pagesPC 1 FlowAssurance PDFAlvaro VelardeNo ratings yet
- TONIC Literature Review in NICE Expert Paper 1 Current Provision and Future Issues Opportunities and Difficulties For Commissioning PDF 4368786157Document5 pagesTONIC Literature Review in NICE Expert Paper 1 Current Provision and Future Issues Opportunities and Difficulties For Commissioning PDF 4368786157TONICNo ratings yet