You might also like
- The Duty for Sponor Oversight in Clinical Trials: Practical Guide: 2nd Edition Clinical Data ReviewFrom EverandThe Duty for Sponor Oversight in Clinical Trials: Practical Guide: 2nd Edition Clinical Data ReviewNo ratings yet
- SITE GEN-001 01 - SOP On Site ActivitiesDocument17 pagesSITE GEN-001 01 - SOP On Site ActivitiesCR Professionals IndiaNo ratings yet
- Data Integrity and Compliance: A Primer for Medical Product ManufacturersFrom EverandData Integrity and Compliance: A Primer for Medical Product ManufacturersNo ratings yet
- NIDCR Guidelines for Levels of Clinical Site MonitoringDocument5 pagesNIDCR Guidelines for Levels of Clinical Site MonitoringJosef BreuerNo ratings yet
- Onsite Monitoring2Document9 pagesOnsite Monitoring2feawefNo ratings yet
- CLN-20 00 Investigational Product HandlingDocument4 pagesCLN-20 00 Investigational Product Handlingpopatlilo2No ratings yet
- Site FDA inspection checklistDocument9 pagesSite FDA inspection checklistsreeraj.guruvayoorNo ratings yet
- Introduction Clinical TrialsDocument22 pagesIntroduction Clinical TrialsSharadNo ratings yet
- Works For Sanofi AventisDocument6 pagesWorks For Sanofi AventisMohit AroraNo ratings yet
- Ethics Resolution Assignment 1Document4 pagesEthics Resolution Assignment 1api-517780146No ratings yet
- Summary of HIPPA Privacy RuleDocument25 pagesSummary of HIPPA Privacy Rulesuluclac100% (3)
- Automated Signal DetectionDocument7 pagesAutomated Signal DetectionSutirtho MukherjiNo ratings yet
- Privacy Notice en 29-06-16Document12 pagesPrivacy Notice en 29-06-16Roya BahzadNo ratings yet
- Sop Title: SOP Version No: 01 Date:: Reviewing and Obtaining Informed ConsentDocument12 pagesSop Title: SOP Version No: 01 Date:: Reviewing and Obtaining Informed ConsentMadhan MohanNo ratings yet
- Audit Findings in Clinical TrialsDocument21 pagesAudit Findings in Clinical TrialsMohit SinghNo ratings yet
- WWORTH SOP10ProjectManagementV2.2 140507Document21 pagesWWORTH SOP10ProjectManagementV2.2 140507Fery Alapola100% (1)
- RCT Methodology ChecklistDocument2 pagesRCT Methodology ChecklistMuhammad IqbalNo ratings yet
- Confidentiality PolicyDocument26 pagesConfidentiality PolicyKulkarni LaboratoryNo ratings yet
- Hipaa Privacy3 09Document3 pagesHipaa Privacy3 09Jennifer WalkerNo ratings yet
- Global Drug Safety Regulations and Reporting RequirementsDocument75 pagesGlobal Drug Safety Regulations and Reporting RequirementsSony M Nidhiry100% (1)
- SOP 302 SiteQualificationVisitDocument3 pagesSOP 302 SiteQualificationVisitna sarvaNo ratings yet
- Discrepancy ManagementDocument34 pagesDiscrepancy Managementnikunj_patel_4367% (6)
- Patient Intake and Consent FormsDocument13 pagesPatient Intake and Consent FormsSam EmekaNo ratings yet
- Standard Operating Procedure Trial Master File and 421 Main Evidence in TheDocument33 pagesStandard Operating Procedure Trial Master File and 421 Main Evidence in Theahmed.bouchenakNo ratings yet
- TgaDocument33 pagesTgavarun rajNo ratings yet
- Clinical Trial ChecklistDocument3 pagesClinical Trial ChecklistIzzi FekratNo ratings yet
- Site Close-Out Visit: Standard Operating Procedures For Clinical Research at Kent State UniversityDocument4 pagesSite Close-Out Visit: Standard Operating Procedures For Clinical Research at Kent State Universityna sarvaNo ratings yet
- SOP 02 Delegation of ResponsibilitiesDocument5 pagesSOP 02 Delegation of ResponsibilitiesAdi PrasetyoNo ratings yet
- Current Trends in PharmacovigilanceDocument5 pagesCurrent Trends in PharmacovigilanceSutirtho MukherjiNo ratings yet
- The Research ProtocolDocument8 pagesThe Research Protocollil assNo ratings yet
- RACI Matrix Peds Clinical Trial Pre-Award DS 2-27-2017Document3 pagesRACI Matrix Peds Clinical Trial Pre-Award DS 2-27-2017alfaroq_almsryNo ratings yet
- Screening and Enrollment: Standard Operating Procedures For Clinical Research at Kent State UniversityDocument6 pagesScreening and Enrollment: Standard Operating Procedures For Clinical Research at Kent State UniversityAlberio CygnusNo ratings yet
- Joint Research Arrangements SOPDocument9 pagesJoint Research Arrangements SOPmo2bioNo ratings yet
- Audit Manual Clinical TrialDocument22 pagesAudit Manual Clinical TrialnikjadhavNo ratings yet
- Ethical Issues in Clinical ResearchDocument33 pagesEthical Issues in Clinical ResearchSenthil ThyagarajanNo ratings yet
- MEDDRA, PVPI, PVMF, PsMF-1Document28 pagesMEDDRA, PVPI, PVMF, PsMF-1Nitin Shah100% (1)
- Hipaa Information and Consent FormDocument1 pageHipaa Information and Consent FormJake HennemanNo ratings yet
- Annex IV To Guidance For The Conduct of GCP Inspections - Sponsor and Cro en PDFDocument7 pagesAnnex IV To Guidance For The Conduct of GCP Inspections - Sponsor and Cro en PDFMarcM77No ratings yet
- ScientificDocument4 pagesScientificNarendar ReddyNo ratings yet
- Regulatory Binder ChecklistDocument4 pagesRegulatory Binder ChecklistOscar Pompa MeraNo ratings yet
- Clinical Research AssociateDocument2 pagesClinical Research AssociatepalkybdNo ratings yet
- Hipaa FormDocument1 pageHipaa FormAskDoctorPontonNo ratings yet
- FDA Medical Device Inspections GuideDocument31 pagesFDA Medical Device Inspections GuideTomasz WojteraNo ratings yet
- Pharmaceutical Compliance and Enforcement: Answer BookDocument62 pagesPharmaceutical Compliance and Enforcement: Answer BookBellNo ratings yet
- Sop Title: Assessing Protocol Feasibility: Sop No: Effective DateDocument7 pagesSop Title: Assessing Protocol Feasibility: Sop No: Effective Datetiara rengganis100% (1)
- Clinical Scientist or Clinical Project Manager or Data Project MDocument4 pagesClinical Scientist or Clinical Project Manager or Data Project Mapi-78033598No ratings yet
- Postmarketing Drug Safety and Inspection ReadinessDocument57 pagesPostmarketing Drug Safety and Inspection Readinesssthug25No ratings yet
- MHRA - Guidance List - FinalDocument21 pagesMHRA - Guidance List - FinalAnand UbheNo ratings yet
- Essentail Documents For Conduct of A Clinical TrialDocument26 pagesEssentail Documents For Conduct of A Clinical TrialFarah Aman KhanNo ratings yet
- Human Research Protection Program Informed Consent ProcessDocument6 pagesHuman Research Protection Program Informed Consent ProcessNurul KurniawatiNo ratings yet
- Organizational Management Personnel: FDA Inspection ChecklistDocument2 pagesOrganizational Management Personnel: FDA Inspection Checklistregina dela cruzNo ratings yet
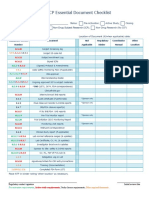
- ICH GCP Essential Document ChecklistDocument2 pagesICH GCP Essential Document ChecklistMohammed Yousffi50% (2)
- Protocol Designing in CTDocument5 pagesProtocol Designing in CTSushma Reddy VNo ratings yet
- Sop Informed ConsentDocument4 pagesSop Informed ConsentWelzha Meturan-kadmaerubunNo ratings yet
- The Monitoring ProcessDocument10 pagesThe Monitoring Processapi-3810976100% (2)
- Phases of Clinical TrialsDocument17 pagesPhases of Clinical Trialselsaveradqp100% (1)
- GCP Inspection Checklist: I. GeneralDocument10 pagesGCP Inspection Checklist: I. Generalsuhas lavhekarNo ratings yet
- Cra GuideDocument17 pagesCra Guidebitterlemon01No ratings yet
- Standard Operating Procedure for Source DocumentationDocument29 pagesStandard Operating Procedure for Source DocumentationSreeraj Guruvayoor SNo ratings yet
- Guide To Clinical Trial Protocol Content and FormatDocument8 pagesGuide To Clinical Trial Protocol Content and FormatRohit Manakchand ZawarNo ratings yet
- Varini CourseDocument1 pageVarini CourseMichael BonettNo ratings yet
- MAR 019 - International Enquiry - REV2Document2 pagesMAR 019 - International Enquiry - REV2Michael BonettNo ratings yet
- Ss CleanboxiiDocument1 pageSs CleanboxiiMichael BonettNo ratings yet
- GDP Mapping Template 0.1Document81 pagesGDP Mapping Template 0.1Michael BonettNo ratings yet
- AML Annual Report 2021Document12 pagesAML Annual Report 2021Kareem StaytiehNo ratings yet
- Keywords AML AssignmentDocument2 pagesKeywords AML AssignmentMichael BonettNo ratings yet
- Set List MetallicaDocument1 pageSet List MetallicaMichael BonettNo ratings yet
- Root Cause AnalysisDocument23 pagesRoot Cause AnalysisMichael BonettNo ratings yet
- Tutor MMDocument1 pageTutor MMMichael BonettNo ratings yet
- The Unique Jazz Pedagogy of Dennis SandoleDocument26 pagesThe Unique Jazz Pedagogy of Dennis SandoleMichael Bonett100% (1)
- Qualified Person Good Practice Guide Update 2023 v01Document94 pagesQualified Person Good Practice Guide Update 2023 v01Michael BonettNo ratings yet
- Invoice 268802 Hamcor LTD - Two Poster Folders 23.88 GBPDocument1 pageInvoice 268802 Hamcor LTD - Two Poster Folders 23.88 GBPMichael BonettNo ratings yet
- Track and Trace - Royal Mail ParcelsDocument3 pagesTrack and Trace - Royal Mail ParcelsMichael BonettNo ratings yet
- Track and Trace - Royal Mail ParcelsDocument3 pagesTrack and Trace - Royal Mail ParcelsMichael BonettNo ratings yet
- India - Projected Monthly Income After Tax DeductionsDocument1 pageIndia - Projected Monthly Income After Tax DeductionsMichael BonettNo ratings yet
- 4 13 Book BeatlesDocument1 page4 13 Book BeatlesMichael BonettNo ratings yet
- Invoice PaymentsDocument1 pageInvoice PaymentsMichael BonettNo ratings yet
- Eu and Local Legislation and GuidelinesDocument1 pageEu and Local Legislation and GuidelinesMichael BonettNo ratings yet
- Dec 2022 deliveries: Pedals, headphones, books & moreDocument1 pageDec 2022 deliveries: Pedals, headphones, books & moreMichael BonettNo ratings yet
- Russian Music Theory Reserach Dec 2022Document3 pagesRussian Music Theory Reserach Dec 2022Michael BonettNo ratings yet
- Finest RalDocument1 pageFinest RalMichael BonettNo ratings yet
- Guitar Symmetry ExplainedDocument4 pagesGuitar Symmetry ExplainedMichael BonettNo ratings yet
- Root Cause AnalysisDocument23 pagesRoot Cause AnalysisMichael BonettNo ratings yet
- Transformational Theory ExplainedDocument1 pageTransformational Theory ExplainedMichael BonettNo ratings yet
- Symmetrical Elements in Music Theory: Minor Seventh, Dorian Mode, Octatonic ScaleDocument1 pageSymmetrical Elements in Music Theory: Minor Seventh, Dorian Mode, Octatonic ScaleMichael BonettNo ratings yet
- Set List MetallicaDocument1 pageSet List MetallicaMichael BonettNo ratings yet
- Crammit 1.4.4 User GuideDocument13 pagesCrammit 1.4.4 User GuideMichael BonettNo ratings yet
- Tonal Pitch SpaceDocument1 pageTonal Pitch SpaceMichael BonettNo ratings yet
- CAPA DefinitonDocument1 pageCAPA DefinitonMichael BonettNo ratings yet
- CAPA Definiton - RecognizedDocument1 pageCAPA Definiton - RecognizedMichael BonettNo ratings yet
- Joint Analysis Handbook 3rd EditionDocument122 pagesJoint Analysis Handbook 3rd EditionΣταύρος ΜυγιάκηςNo ratings yet
- Teacher's Perceptions Related To Principals' Creative Leadership Practices Towards School EffectivenessDocument13 pagesTeacher's Perceptions Related To Principals' Creative Leadership Practices Towards School EffectivenessKEE POH LEE MoeNo ratings yet
- STAN5 JCI AccreditationDocument57 pagesSTAN5 JCI AccreditationYulinur FirdausNo ratings yet
- Colwell-Chanthaphonh TEMA 2Document17 pagesColwell-Chanthaphonh TEMA 2'Lautaro Lopez GeronazzoNo ratings yet
- Manual Che301Document53 pagesManual Che301fitashah2634No ratings yet
- StatisticsDocument9 pagesStatisticsJennilyn Paguio CastilloNo ratings yet
- A Comparison Study of Mainstream Sustainable-Green Building Rating Tools in The WorldDocument5 pagesA Comparison Study of Mainstream Sustainable-Green Building Rating Tools in The WorldTracy HnilNo ratings yet
- Extent of The Relationship Between Burnout Syndrome and Resilience On Factors Implicit To The Teaching Profession. A Systematic Review 2021Document24 pagesExtent of The Relationship Between Burnout Syndrome and Resilience On Factors Implicit To The Teaching Profession. A Systematic Review 2021Eugen Neculai GazziNo ratings yet
- Last ApdataDocument6 pagesLast Apdataقاسم سليمانNo ratings yet
- Principles of Linguistic Change - Fatores InternosDocument674 pagesPrinciples of Linguistic Change - Fatores InternosGermana Rodrigues100% (1)
- Research Paper On The Lost Colony of RoanokeDocument4 pagesResearch Paper On The Lost Colony of Roanokeafeayaczb100% (1)
- The Effectiveness of Trunk Training On Trunk Control, Sitting and Standing Balance and Mobility Post-Stroke: A Systematic Review and Meta-AnalysisDocument11 pagesThe Effectiveness of Trunk Training On Trunk Control, Sitting and Standing Balance and Mobility Post-Stroke: A Systematic Review and Meta-AnalysisMarcela NunesNo ratings yet
- Technical Note: Developing Results FrameworksDocument11 pagesTechnical Note: Developing Results FrameworksJaps HattaNo ratings yet
- Solu 8Document35 pagesSolu 8Basil Aziz TinahNo ratings yet
- Comic Strips in Teaching English Among Grade 11 Learners of Dr. Juan A. Pastor Memorial National High SchoolDocument18 pagesComic Strips in Teaching English Among Grade 11 Learners of Dr. Juan A. Pastor Memorial National High SchoolDonnaValdezNo ratings yet
- Trauma Informed Care: A Commentary and Critique: Lucy Berliner and David J. KolkoDocument5 pagesTrauma Informed Care: A Commentary and Critique: Lucy Berliner and David J. KolkoJohn BitsasNo ratings yet
- Bay 2012Document13 pagesBay 2012Sixto Gutiérrez SaavedraNo ratings yet
- Full Download Ebook PDF Shortell and Kaluznys Healthcare Management Organization Design and Behavior 7th Edition PDFDocument41 pagesFull Download Ebook PDF Shortell and Kaluznys Healthcare Management Organization Design and Behavior 7th Edition PDFroland.montez89697% (33)
- CH 2-IIOEDocument22 pagesCH 2-IIOEAnonymous WCWjddjCcNo ratings yet
- Introduction of Team Work: Green and Baron Define A Team As "A Group Whose Members HaveDocument17 pagesIntroduction of Team Work: Green and Baron Define A Team As "A Group Whose Members HavemonzyansNo ratings yet
- Flipping College Calculus: Case Study on Achievement & PreparationDocument12 pagesFlipping College Calculus: Case Study on Achievement & PreparationShreyas ChaturvediNo ratings yet
- Critical Thinking References List PDFDocument12 pagesCritical Thinking References List PDFIhda Nuria Afidah100% (1)
- Legal Drafting-I: Fourth Year - Semester - IDocument5 pagesLegal Drafting-I: Fourth Year - Semester - IUzma Sheikh100% (1)
- Webley, Qualitative Approaches To Empirical Legal ResearchDocument21 pagesWebley, Qualitative Approaches To Empirical Legal ResearchPhilip BremnerNo ratings yet
- PMG Note Chapter 4Document6 pagesPMG Note Chapter 4Nur Alisa FatinNo ratings yet
- Point Estimate of Population MeanDocument2 pagesPoint Estimate of Population MeanJeff LacasandileNo ratings yet
- What Is The McKinsey 7s ModelDocument5 pagesWhat Is The McKinsey 7s ModelTilahun MogesNo ratings yet
- Course Applied MSC Economics For DevelopmentDocument3 pagesCourse Applied MSC Economics For DevelopmentELISHA KIPLANGATNo ratings yet
- 2 Symposium On Lift and Escalator Technologies: Lutfi Al-Sharif, Ahmad M. Abu Alqumsan, Osama F. Abdel AalDocument7 pages2 Symposium On Lift and Escalator Technologies: Lutfi Al-Sharif, Ahmad M. Abu Alqumsan, Osama F. Abdel AalfreddyjoertyNo ratings yet
- Module 1 G7 Science Q1 Wk1Document24 pagesModule 1 G7 Science Q1 Wk1Paris Azarcon TajanlangitNo ratings yet