You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5807)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (346)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Students Hand Book 2021-22Document123 pagesStudents Hand Book 2021-22DR. SP RAONo ratings yet
- Standardised Drug Infusion ConcentrationsDocument16 pagesStandardised Drug Infusion Concentrationsnot here 2make friends sorryNo ratings yet
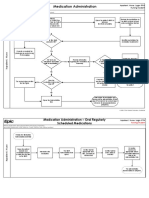
- Medication Administration-Held MedicationsDocument5 pagesMedication Administration-Held MedicationsRawad JamaleddineNo ratings yet
- Long Case O&G-placenta PraeviaDocument24 pagesLong Case O&G-placenta Praeviasaifulhusni100% (2)
- Invitation Letter RabiesDocument6 pagesInvitation Letter RabiessamNo ratings yet
- Dr. Sergio Paguio: AutopsyDocument3 pagesDr. Sergio Paguio: AutopsyZazaNo ratings yet
- Emerys Elements of Medical Genetics E Book Turnpenny Full ChapterDocument51 pagesEmerys Elements of Medical Genetics E Book Turnpenny Full Chapterchristopher.hurd779100% (6)
- CDC Report: "Antibiotic Resistance Threats in The United States"Document148 pagesCDC Report: "Antibiotic Resistance Threats in The United States"Patrick CrozierNo ratings yet
- Calculous Biliary Disease: Current DiagnosisDocument5 pagesCalculous Biliary Disease: Current DiagnosisFernanda Copete YolianisNo ratings yet
- Ruth Bempah Resume FinalDocument2 pagesRuth Bempah Resume Finalapi-510417475No ratings yet
- Herpes Zoster Ophthalmicus Clinical Presentation and Risk Factors For Loss of VisionDocument7 pagesHerpes Zoster Ophthalmicus Clinical Presentation and Risk Factors For Loss of VisionWTF AttaNo ratings yet
- TaniaDocument14 pagesTaniaOm SharmaNo ratings yet
- News Letter: Dealing With Grief and LossDocument10 pagesNews Letter: Dealing With Grief and LossMandy LeDrewNo ratings yet
- Submission SummaryDocument4 pagesSubmission SummaryAmos OnhanNo ratings yet
- Placenta PreviaDocument19 pagesPlacenta Previarosekatekate929No ratings yet
- Avian Metapneumovirus ClassificationDocument7 pagesAvian Metapneumovirus ClassificationRezaNo ratings yet
- T T 29225 Healthy Body and Mind Powerpoint Activity Ver 8Document11 pagesT T 29225 Healthy Body and Mind Powerpoint Activity Ver 8Ma. Luiza GeliNo ratings yet
- Temporary Crown InstructionsDocument1 pageTemporary Crown InstructionsGhostOperativeNo ratings yet
- Providing Oral CareDocument54 pagesProviding Oral CareErcel ArellanoNo ratings yet
- Choanalatresia PDFDocument38 pagesChoanalatresia PDFSyahnidel FitaNo ratings yet
- ATS Menjawab Soal UKN Maret 2021 HQQDocument18 pagesATS Menjawab Soal UKN Maret 2021 HQQanton suponoNo ratings yet
- Simon Magne Mockup 2008Document8 pagesSimon Magne Mockup 2008George PapaemmanouilNo ratings yet
- WHO 2019 NCoV Vaccine Deployment 2020Document89 pagesWHO 2019 NCoV Vaccine Deployment 2020jadwongscribdNo ratings yet
- Benefit Manual Group Health Insurance - CMSDocument35 pagesBenefit Manual Group Health Insurance - CMSUmang WarudkarNo ratings yet
- GGPO Palliative Care ShortVersion 2.2Document192 pagesGGPO Palliative Care ShortVersion 2.2Alexander Benavides RamirezNo ratings yet
- Advisory On The Complete Suspension of Internship ProgramDocument2 pagesAdvisory On The Complete Suspension of Internship ProgramLeandro SalazarNo ratings yet
- Access To Maternity Healthcare Service in Rural Bangladesh. A Study Area Sariakandi Upazila of Bogura DistrictDocument13 pagesAccess To Maternity Healthcare Service in Rural Bangladesh. A Study Area Sariakandi Upazila of Bogura DistrictSajibNo ratings yet
- Antiphospholipid SyndromeDocument8 pagesAntiphospholipid SyndromeVijeyachandhar DorairajNo ratings yet
- Nursing Management of Nasogastric Tube Feeding in Adult PatientsDocument56 pagesNursing Management of Nasogastric Tube Feeding in Adult PatientsUlfa WidiyaNo ratings yet
- Art 3Document16 pagesArt 3Carol LozanoNo ratings yet