You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5810)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (346)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Terminology, Abbreviations, and Symbols Avera Education & Staffing Solutions Medication Aide Training ProgramDocument11 pagesTerminology, Abbreviations, and Symbols Avera Education & Staffing Solutions Medication Aide Training ProgramAnalizaNo ratings yet
- CardiomyopathyDocument23 pagesCardiomyopathyDefyna Dwi LestariNo ratings yet
- IABP Learning PackageDocument35 pagesIABP Learning Packagekingjoon 78100% (1)
- Basic ECG Interpretation Practice Test: DIRECTIONS: The Following Test Consists of 20 QuestionsDocument10 pagesBasic ECG Interpretation Practice Test: DIRECTIONS: The Following Test Consists of 20 Questionsmihaela_bondocNo ratings yet
- Ch-13 Drugs Used in Heart FailureDocument49 pagesCh-13 Drugs Used in Heart FailureShabrin SadikhNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Antiarrhythmic Drugs-Test-1-QuestionsDocument7 pagesAntiarrhythmic Drugs-Test-1-QuestionsDrishya Bioplannet100% (2)
- Cvs McqsDocument22 pagesCvs McqsShahabuddin Shaikh0% (1)
- ARMAN: Born: 12/15/1985 (Male 32) Test Date: 4/16/2018 8:39:25 AM Puskesmas KampalaDocument3 pagesARMAN: Born: 12/15/1985 (Male 32) Test Date: 4/16/2018 8:39:25 AM Puskesmas KampalaAkram KastiranNo ratings yet
- Answer Key Circulatory System QuizDocument6 pagesAnswer Key Circulatory System Quizapi-534129744No ratings yet
- Syncope PPT (Sample)Document21 pagesSyncope PPT (Sample)Bayushi Eka Putra100% (1)
- Drugs Acting On Cardiovascular SystemDocument18 pagesDrugs Acting On Cardiovascular SystemIbrahem AlNo ratings yet
- SSS Forms Employment ReportDocument3 pagesSSS Forms Employment ReportAnalizaNo ratings yet
- SSSForms ER RegistrationDocument3 pagesSSSForms ER RegistrationAnalizaNo ratings yet
- Biodata SampleDocument2 pagesBiodata SampleAnalizaNo ratings yet
- Bir Form 1905Document2 pagesBir Form 1905AnalizaNo ratings yet
- Acamprosate: Disulfiram (Antabuse)Document6 pagesAcamprosate: Disulfiram (Antabuse)AnalizaNo ratings yet
- Art AppreciationTake Home AcivitiesDocument9 pagesArt AppreciationTake Home AcivitiesAnalizaNo ratings yet
- S&J Caleon Marketing Inc.: Mark Joseph A. FernandezDocument1 pageS&J Caleon Marketing Inc.: Mark Joseph A. FernandezAnalizaNo ratings yet
- Answer Sheet Grade 1 PeriodicalDocument4 pagesAnswer Sheet Grade 1 PeriodicalAnalizaNo ratings yet
- Food Poisoning AntidotesDocument1 pageFood Poisoning AntidotesAnalizaNo ratings yet
- Jurisprudence Activity#2 MidtermDocument1 pageJurisprudence Activity#2 MidtermAnalizaNo ratings yet
- S & J Caleon Marketing Inc. Bambang BranchDocument2 pagesS & J Caleon Marketing Inc. Bambang BranchAnalizaNo ratings yet
- Application LetterDocument1 pageApplication LetterAnalizaNo ratings yet
- Authorization LetterDocument1 pageAuthorization LetterAnalizaNo ratings yet
- 450 - 82235 - RESEARCH DESIGN Module 5Document44 pages450 - 82235 - RESEARCH DESIGN Module 5AnalizaNo ratings yet
- Complete List of Drugs PDFDocument21 pagesComplete List of Drugs PDFAnalizaNo ratings yet
- Bayombong, Nueva Vizcaya: Saint Mary's UniversityDocument3 pagesBayombong, Nueva Vizcaya: Saint Mary's UniversityAnalizaNo ratings yet
- Bayombong, Nueva Vizcaya: Saint Mary's UniversityDocument3 pagesBayombong, Nueva Vizcaya: Saint Mary's UniversityAnalizaNo ratings yet
- Different Kinds of Commercial ArtsDocument6 pagesDifferent Kinds of Commercial ArtsAnalizaNo ratings yet
- Principles of Blood Pressure Measurement - Current Techniques, Office Vs Ambulatory Blood Pressure MeasurementDocument12 pagesPrinciples of Blood Pressure Measurement - Current Techniques, Office Vs Ambulatory Blood Pressure MeasurementindahNo ratings yet
- Cardiac Cycle CardiodynamicsDocument29 pagesCardiac Cycle Cardiodynamicseverforyou2023No ratings yet
- Heart Sounds:: The Third Sound Is Caused by Vibrations During Passive Filling of The Ventricles With The BloodDocument2 pagesHeart Sounds:: The Third Sound Is Caused by Vibrations During Passive Filling of The Ventricles With The BloodShmuel BarshalomNo ratings yet
- Essential HypertensionDocument13 pagesEssential HypertensionIvan KurniadiNo ratings yet
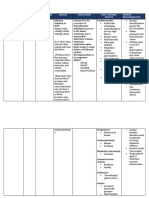
- Drug Name Brand Name Classification Dosage Indications Side/ Adverse Effects Nursing ResponsibilitiesDocument2 pagesDrug Name Brand Name Classification Dosage Indications Side/ Adverse Effects Nursing ResponsibilitiesRonald BurkeNo ratings yet
- Fiziologie Valori Normale PDFDocument1 pageFiziologie Valori Normale PDFStaicu GabrielNo ratings yet
- Exercise 1Document2 pagesExercise 1April Mergelle LapuzNo ratings yet
- Chapter 11 JK PDFDocument50 pagesChapter 11 JK PDFMichael Jove AblazaNo ratings yet
- Normal Sinus RhythmDocument97 pagesNormal Sinus RhythmNatasha LiberisNo ratings yet
- Cardiac Cycle & Heart Sounds Flashcards - QuizletDocument11 pagesCardiac Cycle & Heart Sounds Flashcards - QuizletRadijska Postaja KoprivnicaNo ratings yet
- Blood Pressure ChartDocument4 pagesBlood Pressure ChartSaleem KhanNo ratings yet
- 2015 Akutni Koronarni SindromDocument98 pages2015 Akutni Koronarni SindromIvanMihailovicNo ratings yet
- AneurysmDocument11 pagesAneurysmNashrah HusnaNo ratings yet
- ACLS Megacode Checklist For StudentsDocument3 pagesACLS Megacode Checklist For StudentsKhrisha Anne DavilloNo ratings yet
- Pengaruh Larutan Madu Terhadap Tekanan Darah Lanjut Usia HipertensiDocument10 pagesPengaruh Larutan Madu Terhadap Tekanan Darah Lanjut Usia HipertensiNopita SariNo ratings yet
- Myocardial InfarctionDocument17 pagesMyocardial InfarctionJoshua ReyesNo ratings yet
- McMurray (2015) ESC Modes of Death in HFDocument8 pagesMcMurray (2015) ESC Modes of Death in HFerza jeiel garcesNo ratings yet
- Instruction Manual: M7 Intelli IT (HEM-7361T-EBK) X7 Smart (HEM-7361T-ESL)Document132 pagesInstruction Manual: M7 Intelli IT (HEM-7361T-EBK) X7 Smart (HEM-7361T-ESL)zabbizzoNo ratings yet
- PIIS109491942200007XDocument22 pagesPIIS109491942200007X60'041 Kanin TianbudNo ratings yet
- KROK 2-CardioDocument12 pagesKROK 2-CardioberdaderagaNo ratings yet