You might also like
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Manual de Usuario Airvo2 PDFDocument150 pagesManual de Usuario Airvo2 PDFjhon edison rojas villada100% (1)
- NHF For Copd Feb 2016Document58 pagesNHF For Copd Feb 2016paionenseNo ratings yet
- AIRVO v2.5 Disinfection Manual UI-185048125 - DDocument14 pagesAIRVO v2.5 Disinfection Manual UI-185048125 - DpaionenseNo ratings yet
- Growth Factors: BIT 230 Walsh Chapter 7Document35 pagesGrowth Factors: BIT 230 Walsh Chapter 7paionenseNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Magnetic Field of A SolenoidDocument5 pagesMagnetic Field of A SolenoidKang Yuan ShingNo ratings yet
- Case StudyDocument4 pagesCase Studyadil rangoonNo ratings yet
- Soiling Rates of PV Modules vs. Thermopile PyranometersDocument3 pagesSoiling Rates of PV Modules vs. Thermopile PyranometersAbdul Mohid SheikhNo ratings yet
- Safe Bearing Capacity of Soil - Based On Is: 6403 Sample CalculationDocument1 pageSafe Bearing Capacity of Soil - Based On Is: 6403 Sample CalculationSantosh ZunjarNo ratings yet
- LCS21 - 35 - Polar PlotsDocument14 pagesLCS21 - 35 - Polar Plotsgosek16375No ratings yet
- Vensim User ManualDocument34 pagesVensim User ManualMahdan LondoNo ratings yet
- SOFARSOLAR ModBus-RTU Communication ProtocolDocument22 pagesSOFARSOLAR ModBus-RTU Communication ProtocolВячеслав ЛарионовNo ratings yet
- EXCEL - How To Write Perfect VLOOKUP and INDEX and MATCH FormulasDocument29 pagesEXCEL - How To Write Perfect VLOOKUP and INDEX and MATCH Formulasgerrydimayuga100% (1)
- Refining Corrosion Technologist NACE-RCT-001: NACE Cathodic Protection Technician (CP 2) Written ExamDocument16 pagesRefining Corrosion Technologist NACE-RCT-001: NACE Cathodic Protection Technician (CP 2) Written Examshoaib1985100% (1)
- Module 1 Engineering ScienceDocument38 pagesModule 1 Engineering ScienceLogan JesseNo ratings yet
- Helmholtz Resonance - Wikipedia, The Free EncyclopediaDocument4 pagesHelmholtz Resonance - Wikipedia, The Free Encyclopediahamidah1963No ratings yet
- 3 Perform Industry CalculationsDocument90 pages3 Perform Industry CalculationsRobinson ConcordiaNo ratings yet
- Mathematics GR 11 Paper 2Document13 pagesMathematics GR 11 Paper 2ora mashaNo ratings yet
- Signal Integrity Modeling and Measurement of TSV in 3D ICDocument4 pagesSignal Integrity Modeling and Measurement of TSV in 3D IC張志榮No ratings yet
- UMTS Optimization GuidelineDocument84 pagesUMTS Optimization GuidelineEvelio Sotolongo100% (3)
- Number Patterns and SequencesDocument10 pagesNumber Patterns and SequencesMohamed Hawash80% (5)
- FP 3000 PDFDocument1 pageFP 3000 PDFClaudio Godoy ZepedaNo ratings yet
- 1 - Introduction - Derivatives GreeksDocument50 pages1 - Introduction - Derivatives GreeksThomas GallantNo ratings yet
- Ra 6938Document2 pagesRa 6938GaryNo ratings yet
- Assignment - 1 Introduction of Machines and Mechanisms: TheoryDocument23 pagesAssignment - 1 Introduction of Machines and Mechanisms: TheoryAman AmanNo ratings yet
- Calculus 1: CONTINUITYDocument56 pagesCalculus 1: CONTINUITYMa Lorraine PerezNo ratings yet
- Dbms-Lab Assignment - 1: Name - VIKAS SINGH Roll No - 4257Document3 pagesDbms-Lab Assignment - 1: Name - VIKAS SINGH Roll No - 4257Vikas SinghNo ratings yet
- Configuration A: Unloaded BJT Transistor AmplifiersDocument3 pagesConfiguration A: Unloaded BJT Transistor AmplifiersdasdNo ratings yet
- Switching Power Supply DesignDocument21 pagesSwitching Power Supply DesignSamuel mutindaNo ratings yet
- IS4242 W3 Regression AnalysesDocument67 pagesIS4242 W3 Regression Analyseswongdeshun4No ratings yet
- V1 N2 1980 RabenhorstDocument6 pagesV1 N2 1980 Rabenhorstraa2010No ratings yet
- 1 s2.0 0304386X9190055Q MainDocument32 pages1 s2.0 0304386X9190055Q MainJordan Ulloa Bello100% (1)
- Engg Mechanics Ques BankDocument68 pagesEngg Mechanics Ques BankUtkalNo ratings yet
- 30 - MACRS DepreciationDocument4 pages30 - MACRS Depreciationidriwal mayusdaNo ratings yet
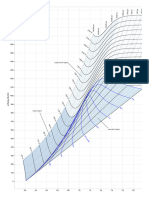
- Mollier Enthalpy Entropy Chart For Steam - US UnitsDocument1 pageMollier Enthalpy Entropy Chart For Steam - US Unitslin tongNo ratings yet