You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Intro To EugenicsDocument16 pagesIntro To EugenicsJesus LivesNo ratings yet
- Lesson 2 Prepare Cereal and StarchDocument25 pagesLesson 2 Prepare Cereal and StarchLieybeem Vergara50% (2)
- Congestive Heart Failure Pathophysiology Schematic DiagramDocument3 pagesCongestive Heart Failure Pathophysiology Schematic DiagramJasleen KaurNo ratings yet
- Statistical EstimationDocument37 pagesStatistical EstimationAmanuel MaruNo ratings yet
- Power Plant IndiaDocument8 pagesPower Plant Indiameet dodhiwalaNo ratings yet
- Hazops Should Be Fun - The Stream-Based HazopDocument77 pagesHazops Should Be Fun - The Stream-Based HazopHector Tejeda100% (1)
- Summarized Report of Gujrat Visit: Party Name AddressDocument10 pagesSummarized Report of Gujrat Visit: Party Name Addressmeet dodhiwalaNo ratings yet
- 3-PHAP vs. Secretary of Health (Domer)Document5 pages3-PHAP vs. Secretary of Health (Domer)Arnel ManalastasNo ratings yet
- Kathwada Industry ListDocument14 pagesKathwada Industry Listmeet dodhiwalaNo ratings yet
- Pharma Directory 2020 SampleDocument9 pagesPharma Directory 2020 Samplemeet dodhiwalaNo ratings yet
- Steels CallsDocument25 pagesSteels Callsmeet dodhiwalaNo ratings yet
- Account Statement From 1 Oct 2020 To 9 Dec 2020: TXN Date Value Date Description Ref No./Cheque No. Debit Credit BalanceDocument4 pagesAccount Statement From 1 Oct 2020 To 9 Dec 2020: TXN Date Value Date Description Ref No./Cheque No. Debit Credit Balancemeet dodhiwalaNo ratings yet
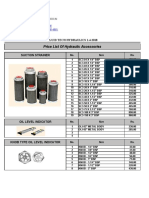
- Price List of Hydraulic Accessories: Fluid Tech Hydraulics 1-4-2018Document1 pagePrice List of Hydraulic Accessories: Fluid Tech Hydraulics 1-4-2018meet dodhiwalaNo ratings yet
- Ingersoll Rand t30 Series Tune Up KitDocument1 pageIngersoll Rand t30 Series Tune Up Kitmeet dodhiwalaNo ratings yet
- INDIAMARTDocument21 pagesINDIAMARTmeet dodhiwalaNo ratings yet
- 1 Vadilal 2 Ratnamani Steels 3 Jagdish Techno Cast 4: SR - No Company NameDocument3 pages1 Vadilal 2 Ratnamani Steels 3 Jagdish Techno Cast 4: SR - No Company Namemeet dodhiwalaNo ratings yet
- Anand Filters BrochureDocument5 pagesAnand Filters Brochuremeet dodhiwalaNo ratings yet
- Amendment To Purchase Manual (Issue 3 - 2013) (As Approved at 299 MC Meeting)Document13 pagesAmendment To Purchase Manual (Issue 3 - 2013) (As Approved at 299 MC Meeting)meet dodhiwalaNo ratings yet
- Marketing Record HemDocument3 pagesMarketing Record Hemmeet dodhiwalaNo ratings yet
- Our Valuale Customer 1Document3 pagesOur Valuale Customer 1meet dodhiwalaNo ratings yet
- TenderPDF1 - NIT - 255Document19 pagesTenderPDF1 - NIT - 255meet dodhiwalaNo ratings yet
- Subject-Industrial Oem and Compressors Filters Respected Sir/Ma'amDocument2 pagesSubject-Industrial Oem and Compressors Filters Respected Sir/Ma'ammeet dodhiwalaNo ratings yet
- Oem - High Performance Screw Compressor Lubricants: OEM Oem Description Oem Part NoDocument23 pagesOem - High Performance Screw Compressor Lubricants: OEM Oem Description Oem Part Nomeet dodhiwalaNo ratings yet
- Marketing Env Add.Document15 pagesMarketing Env Add.meet dodhiwalaNo ratings yet
- ProductDocument14 pagesProductMahendra ShahNo ratings yet
- Max Medic Plan 2Document1 pageMax Medic Plan 2Premkumar NadarajanNo ratings yet
- Sps8 Q1mod1 Skill Related Parameters Noel Rullan Bgo v2Document20 pagesSps8 Q1mod1 Skill Related Parameters Noel Rullan Bgo v2RandyNo ratings yet
- Communication in Palliative CareDocument7 pagesCommunication in Palliative CareIhsan NudinNo ratings yet
- Terminology For Implant Prostheses PDFDocument5 pagesTerminology For Implant Prostheses PDFHugoMoralesTecnicoDentalNo ratings yet
- Goat MeatDocument14 pagesGoat MeatCAPRINOS BAJA CALIFORNIA SUR, MEXICONo ratings yet
- Eric Liou Contributions PDFDocument8 pagesEric Liou Contributions PDFteju patneediNo ratings yet
- A Beauty 671-680Document29 pagesA Beauty 671-680YollyNo ratings yet
- 33 Pol BRF Food Models enDocument36 pages33 Pol BRF Food Models enthuyetnnNo ratings yet
- Effect of A Physiotherapy Program in Women With Primary DysmenorrheaDocument6 pagesEffect of A Physiotherapy Program in Women With Primary DysmenorrheaPaula RangelNo ratings yet
- X Ray Diffraction Safety InformationDocument48 pagesX Ray Diffraction Safety Informationrenjith2017100% (1)
- The WTO and Developing Countries: The Missing: Link of International Distributive JusticeDocument395 pagesThe WTO and Developing Countries: The Missing: Link of International Distributive JusticeMuhammad SajidNo ratings yet
- IOT Based Health Monitoring SystemDocument3 pagesIOT Based Health Monitoring SystemInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Real-Time Health Care Monitoring System Using Iot: International Journal of Engineering & TechnologyDocument5 pagesReal-Time Health Care Monitoring System Using Iot: International Journal of Engineering & TechnologyShaik JunaidNo ratings yet
- Wa0094.Document9 pagesWa0094.lider vigilanciaNo ratings yet
- Gratitude EssayDocument2 pagesGratitude EssaycensoredlasagnaNo ratings yet
- DM 2020-0187 - Must Know Covid IssuancesDocument18 pagesDM 2020-0187 - Must Know Covid IssuancesFranchise AlienNo ratings yet
- Altius Annual Leave Policy Wef 1st January 2012 Ver 1.1Document11 pagesAltius Annual Leave Policy Wef 1st January 2012 Ver 1.1Mudassar HakimNo ratings yet
- Sample Speech Blood Drive PDFDocument5 pagesSample Speech Blood Drive PDFNil PunadiyaNo ratings yet
- A Report - Noise Pollution in Urban AreasDocument14 pagesA Report - Noise Pollution in Urban AreasArjita SinghNo ratings yet
- Format OpnameDocument21 pagesFormat OpnamerestutiyanaNo ratings yet
- PN 1Document1 pagePN 1Florin Eugen ConstantinescuNo ratings yet
- Annual Investment Plan: Municipality of JAGNADocument17 pagesAnnual Investment Plan: Municipality of JAGNA39mtn7No ratings yet
- Ang Among English ThesisDocument12 pagesAng Among English ThesisKai PesquiraNo ratings yet
- School Form 2 (SF2) Daily Attendance Report of LearnersDocument4 pagesSchool Form 2 (SF2) Daily Attendance Report of LearnersRyan A. CabalidaNo ratings yet