You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Video Stroke - Nadya Irena HabibDocument39 pagesVideo Stroke - Nadya Irena HabibtesaNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- International Journal of Gerontology: Gwo-Chi Hu, Yi-Min ChenDocument5 pagesInternational Journal of Gerontology: Gwo-Chi Hu, Yi-Min Chenluthfia ayu az zahraNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Risk Factors For Aneurysmal Subarachnoid Haemorrhage: The Tromsø StudyDocument4 pagesRisk Factors For Aneurysmal Subarachnoid Haemorrhage: The Tromsø StudytesaNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Post Stroke Dementia: Ade Wijaya, MD - February 2019Document15 pagesPost Stroke Dementia: Ade Wijaya, MD - February 2019tesaNo ratings yet
- Post-Stroke Dementia - A Comprehensive ReviewDocument12 pagesPost-Stroke Dementia - A Comprehensive ReviewtesaNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Nimodipine For The Prevention of Cerebral VasospasmDocument18 pagesNimodipine For The Prevention of Cerebral VasospasmtesaNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Drug Treatment of Cerebral Vasospasm AfterDocument8 pagesDrug Treatment of Cerebral Vasospasm AftertesaNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Reversible Visual Loss After Shunt Malfunction: WenzelDocument3 pagesReversible Visual Loss After Shunt Malfunction: WenzeltesaNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Link Yutub FREE CLASS MEDIKO PSIKIATRI DRDocument1 pageLink Yutub FREE CLASS MEDIKO PSIKIATRI DRtesaNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Using Nimodipine For Patients With Aneurysmal Subarachnoid HemorrhageDocument1 pageUsing Nimodipine For Patients With Aneurysmal Subarachnoid HemorrhagetesaNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Link Yutub FREE CLASS MEDIKO PSIKIATRI DRDocument1 pageLink Yutub FREE CLASS MEDIKO PSIKIATRI DRtesaNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Tepas 1987Document12 pagesTepas 1987IipAlqadrieNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Current Options For The ManagementDocument22 pagesCurrent Options For The ManagementtesaNo ratings yet
- Controlled Trial of Nimodipine in Patients With Subarachnoid HemorrhageDocument6 pagesControlled Trial of Nimodipine in Patients With Subarachnoid HemorrhagetesaNo ratings yet
- ADA GAMBAR PEMERIKSAAN EAGAN - Post-Stroke-Dementia - FINALDocument43 pagesADA GAMBAR PEMERIKSAAN EAGAN - Post-Stroke-Dementia - FINALtesaNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Subarachnoid Haemorrhage, Lancet, 1-07Document13 pagesSubarachnoid Haemorrhage, Lancet, 1-07Luciana RafaelNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Free PPT Template S: Insert The Title of Your Presentation HereDocument37 pagesFree PPT Template S: Insert The Title of Your Presentation HeretesaNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Post-Stroke Dementia - A Comprehensive ReviewDocument12 pagesPost-Stroke Dementia - A Comprehensive ReviewtesaNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Medical Jeopardy by SlidesgoDocument45 pagesMedical Jeopardy by SlidesgotesaNo ratings yet
- Video Stroke - Nadya Irena HabibDocument39 pagesVideo Stroke - Nadya Irena HabibtesaNo ratings yet
- CBT Ipd DM 1Document50 pagesCBT Ipd DM 1tesaNo ratings yet
- AJMseries HeadacheDocument9 pagesAJMseries HeadachetesaNo ratings yet
- Clinical CaseDocument46 pagesClinical CaseMahes WNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Medical Thesis by SlidesgoDocument32 pagesMedical Thesis by SlidesgotesaNo ratings yet
- Clinical CaseDocument46 pagesClinical CaseMahes WNo ratings yet
- Coronavirus Breakthrough by SlidesgoDocument44 pagesCoronavirus Breakthrough by SlidesgotesaNo ratings yet
- Journal Rosacea Report Lain PDFDocument5 pagesJournal Rosacea Report Lain PDFtesaNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Jurnal Cutaneous Larva MigransDocument5 pagesJurnal Cutaneous Larva MigranstesaNo ratings yet
- Medical Thesis by SlidesgoDocument32 pagesMedical Thesis by SlidesgotesaNo ratings yet
- Biomedica Manikins CatalogDocument64 pagesBiomedica Manikins CatalogRahul KashyapNo ratings yet
- Evaluation and Diagnosis of Multiple Sclerosis in Adults - UpToDateDocument45 pagesEvaluation and Diagnosis of Multiple Sclerosis in Adults - UpToDatespritdummyNo ratings yet
- Molecular Basis of Cancer 2021 - RikaDocument58 pagesMolecular Basis of Cancer 2021 - RikaHenry Wijaya100% (1)
- First Quarterly Exam Personal DevelopmentDocument4 pagesFirst Quarterly Exam Personal DevelopmentCrystal Renz TibayanNo ratings yet
- Spinal Cord TumoursDocument15 pagesSpinal Cord TumoursSakshi NegiNo ratings yet
- Interstitial Lung DiseaseDocument14 pagesInterstitial Lung DiseaseAzkaZulfiqarNo ratings yet
- Buerger's Disease (Thromboangiitis Obliterans)Document6 pagesBuerger's Disease (Thromboangiitis Obliterans)Mikaela Eris CortelloNo ratings yet
- Centralretinalarteryocclusion 150821150708 Lva1 App6891 PDFDocument50 pagesCentralretinalarteryocclusion 150821150708 Lva1 App6891 PDFDhivya SekarNo ratings yet
- Perineural Invasion Molecular MechanismsDocument21 pagesPerineural Invasion Molecular MechanismsgangligonNo ratings yet
- I. Learning Objective:: /endocrine-System-Lesson-Plan-Final-Na-FinalDocument10 pagesI. Learning Objective:: /endocrine-System-Lesson-Plan-Final-Na-FinalGabilan Rose JeanNo ratings yet
- 12 rules for life by Dr. Jordan Peterson analyzedDocument12 pages12 rules for life by Dr. Jordan Peterson analyzedTamo Mujiri100% (1)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Endocrine SystemDocument7 pagesEndocrine Systemfumiko.cruzNo ratings yet
- Krok2 - Medicine - 2013Document28 pagesKrok2 - Medicine - 2013ashighaNo ratings yet
- Cerebral MalariaDocument6 pagesCerebral MalariaIrsanti sasmitaNo ratings yet
- Production of Growth Factors, Cytokines, and ChemokinesDocument16 pagesProduction of Growth Factors, Cytokines, and ChemokinesNina TrươngNo ratings yet
- Occupational Therapy in Oncology and Palliative CareDocument10 pagesOccupational Therapy in Oncology and Palliative CareSenthil KumarNo ratings yet
- Tetraparesis, Hemiparesis, and Ataxia: Lesion LocalizationDocument1 pageTetraparesis, Hemiparesis, and Ataxia: Lesion Localizationibnu annafiNo ratings yet
- Motor Impairments Following StrokeDocument31 pagesMotor Impairments Following StrokeFrancess LeveauNo ratings yet
- Ultrasound in Obstet Gyne - 2022 - PaladiniDocument8 pagesUltrasound in Obstet Gyne - 2022 - PaladiniKarim Muñoz NiñoNo ratings yet
- Proton TherapyDocument21 pagesProton Therapytrieu leNo ratings yet
- BrainDocument3 pagesBrainWidiya BudiNo ratings yet
- Piriformis Syndrome ReviewDocument6 pagesPiriformis Syndrome Reviewismael wandikboNo ratings yet
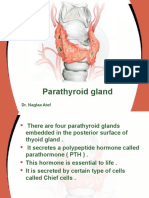
- Parathyroid Gland Controls Calcium LevelsDocument24 pagesParathyroid Gland Controls Calcium LevelsReem 10No ratings yet
- Critical & Sensitive Periods: Concept History MethodsDocument21 pagesCritical & Sensitive Periods: Concept History MethodsLhara CampolloNo ratings yet
- Body Fluids Analysis LectureDocument17 pagesBody Fluids Analysis LectureAsd Asd100% (1)
- Optic Disk Drusen in ChildrenDocument14 pagesOptic Disk Drusen in ChildrenPriscila VerduzcoNo ratings yet
- Featured Review Central Retinal Artery Occlusion: Sohan Singh HayrehDocument11 pagesFeatured Review Central Retinal Artery Occlusion: Sohan Singh HayrehCoco Silva VereauNo ratings yet
- Nursing Roles in Male and Female Reproductive HealthDocument43 pagesNursing Roles in Male and Female Reproductive HealthKisses Joyce AlmazarNo ratings yet
- Wilkins Clinical Assessment in Respiratory Care 7th Edition Heuer Test BankDocument10 pagesWilkins Clinical Assessment in Respiratory Care 7th Edition Heuer Test Bankanthelioncingulumgvxq100% (21)
- Complications Following Head InjuryDocument6 pagesComplications Following Head InjuryKiran ShelkeNo ratings yet
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (14)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 3.5 out of 5 stars3.5/5 (2)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)