You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- 2007 AP Statistics Multiple Choice ExamDocument17 pages2007 AP Statistics Multiple Choice ExamJalaj SoodNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Open Delta Purpose in EFDocument2 pagesOpen Delta Purpose in EFnmanikandanNo ratings yet
- Ca 800Document83 pagesCa 800Pablo CzNo ratings yet
- Ca 800Document83 pagesCa 800Pablo CzNo ratings yet
- Boroscope Inspection Procedure 7th Stage StatorDocument15 pagesBoroscope Inspection Procedure 7th Stage StatorAPU SHOP BTH MS100% (2)
- F 2394 - 04Document11 pagesF 2394 - 04Pablo CzNo ratings yet
- Sample Emg/Ncv Report - Normal StudyDocument5 pagesSample Emg/Ncv Report - Normal StudyPhysiotherapist AliNo ratings yet
- Enzyme Review Mcqs (From The Official Biochemistry Study Guide)Document5 pagesEnzyme Review Mcqs (From The Official Biochemistry Study Guide)Mrs Rehan100% (1)
- Astm F-1185Document3 pagesAstm F-1185Pablo Cz100% (1)
- Chapter 8 Sensation and PerceptionDocument66 pagesChapter 8 Sensation and Perceptionapi-726122866No ratings yet
- Medical Devices RegulationsDocument59 pagesMedical Devices RegulationsPablo CzNo ratings yet
- 9 Bibliographic ReferencesDocument1 page9 Bibliographic ReferencesPablo CzNo ratings yet
- ASTM F748 Selecting Biological Test MethodsDocument33 pagesASTM F748 Selecting Biological Test MethodsPablo CzNo ratings yet
- Surgical Treatment of Isolated Zygomatic FractureDocument7 pagesSurgical Treatment of Isolated Zygomatic FracturePablo CzNo ratings yet
- Artículo Integral Fixation Titanium Polyetheretherketone-1-4Document4 pagesArtículo Integral Fixation Titanium Polyetheretherketone-1-4Pablo CzNo ratings yet
- RDC 185 2001 Classification and Registration Requirements of Medical Products 0Document17 pagesRDC 185 2001 Classification and Registration Requirements of Medical Products 0Karina GonzalezNo ratings yet
- Mechanical Properties of Alumina-Zirconia CompositDocument7 pagesMechanical Properties of Alumina-Zirconia CompositPablo CzNo ratings yet
- CT-800A IEC60601-1-2 - Unlocked PDFDocument61 pagesCT-800A IEC60601-1-2 - Unlocked PDFPablo CzNo ratings yet
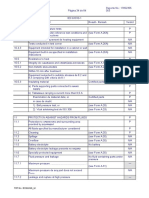
- Clearance Creepágina Distances Enclosures: TRF No. IEC61010 - 1JDocument73 pagesClearance Creepágina Distances Enclosures: TRF No. IEC61010 - 1JPablo CzNo ratings yet
- 15 User ManualDocument3 pages15 User ManualPablo CzNo ratings yet
- A 53 - A 53m - 00 QtuzltawDocument7 pagesA 53 - A 53m - 00 QtuzltawPablo CzNo ratings yet
- F 921 - 85Document4 pagesF 921 - 85Pablo CzNo ratings yet
- F981-04-2016 Biocompatibilidad de Materiales en Músculo y Hueso PDFDocument5 pagesF981-04-2016 Biocompatibilidad de Materiales en Músculo y Hueso PDFPablo CzNo ratings yet
- A 53 - A 53M - 00 Qtuzltaw PDFDocument21 pagesA 53 - A 53M - 00 Qtuzltaw PDFRony AgistaNo ratings yet
- A 105 - A 105M - 03 Qtewns9bmta1tqDocument5 pagesA 105 - A 105M - 03 Qtewns9bmta1tqLuis Armando Palacios VargasNo ratings yet
- CT-1 Accessory ListDocument1 pageCT-1 Accessory ListPablo CzNo ratings yet
- Tissue Engineered Medical Products: Standard Terminology Relating ToDocument6 pagesTissue Engineered Medical Products: Standard Terminology Relating ToPablo CzNo ratings yet
- F 2319 - RjizmtkDocument13 pagesF 2319 - Rjizmtkmohan chand mulpuriNo ratings yet
- TRC NW8FDocument5 pagesTRC NW8FPablo CzNo ratings yet
- ExpeDocument1 pageExpePablo CzNo ratings yet
- Auxin TransportDocument6 pagesAuxin TransportPablo CzNo ratings yet
- Diesel Engine Lab ReportDocument27 pagesDiesel Engine Lab ReportParadoodleNo ratings yet
- 9 F 957375 B 361250 FB 704Document15 pages9 F 957375 B 361250 FB 704api-498018677No ratings yet
- Emergency Response Plan and PreparednessDocument7 pagesEmergency Response Plan and Preparednessradha krishnaNo ratings yet
- Air Compressor: TopicDocument17 pagesAir Compressor: TopicManuel GuerreroNo ratings yet
- Green Rating System - Ritik JainDocument6 pagesGreen Rating System - Ritik Jainmayuresh barbarwarNo ratings yet
- Resume - Niloofar MojaradDocument2 pagesResume - Niloofar Mojaradmohammadrezahajian12191No ratings yet
- Early Theories On The Origin of Life On Earth: Creation TheoryDocument1 pageEarly Theories On The Origin of Life On Earth: Creation TheoryAngel Elizaga IINo ratings yet
- Left Side View: Electrical System G3516A and G3516B EngineDocument2 pagesLeft Side View: Electrical System G3516A and G3516B EngineAM76100% (1)
- Bcba CourseworkDocument8 pagesBcba Courseworkafjwoamzdxwmct100% (2)
- Experiment-3: Study of Microstructure and Hardness Profile of Mild Steel Bar During Hot Rolling (Interrupted) 1. AIMDocument5 pagesExperiment-3: Study of Microstructure and Hardness Profile of Mild Steel Bar During Hot Rolling (Interrupted) 1. AIMSudhakar LavuriNo ratings yet
- The Company - MicroDocument2 pagesThe Company - MicroMai Hương QuỳnhNo ratings yet
- Transmission Line BOQ VIMPDocument72 pagesTransmission Line BOQ VIMPkajale_shrikant2325No ratings yet
- RNA and Protein Synthesis Problem SetDocument6 pagesRNA and Protein Synthesis Problem Setpalms thatshatterNo ratings yet
- DGMS Final ReportDocument15 pagesDGMS Final ReportMaverickNo ratings yet
- 2023-24 SR - Super60 (Incoming) STERLING Batch CHEMISTRY Teaching & Test Schedule Code@03!04!2023Document16 pages2023-24 SR - Super60 (Incoming) STERLING Batch CHEMISTRY Teaching & Test Schedule Code@03!04!2023K R I S H100% (1)
- Sex Education in The PhilippinesDocument3 pagesSex Education in The PhilippinesChinchin CañeteNo ratings yet
- Steri - Cycle I 160 New GenDocument16 pagesSteri - Cycle I 160 New GenLEO AROKYA DASSNo ratings yet
- LMA An. I-Sem 1-Engleza LEC-The Category of Aspect & Aspect 3-Reedited OnDocument4 pagesLMA An. I-Sem 1-Engleza LEC-The Category of Aspect & Aspect 3-Reedited OnIlie IonelNo ratings yet
- Lecture 16 - Bleeding Tendency DiseasesDocument64 pagesLecture 16 - Bleeding Tendency Diseasesapi-3703352100% (1)
- Employee Turnover ReportDocument10 pagesEmployee Turnover ReportDon83% (6)
- شيتات محطات كهربية PDFDocument8 pagesشيتات محطات كهربية PDFhazem saeidNo ratings yet
- Assessment of Reading Comprehension 2Document8 pagesAssessment of Reading Comprehension 2Kutu DemangNo ratings yet
- Developments in Injection Moulding 3Document331 pagesDevelopments in Injection Moulding 3Salah HammamiNo ratings yet
- Electron Configurations of The Elements (Data Page) - WikipediaDocument25 pagesElectron Configurations of The Elements (Data Page) - WikipediaAlex OmungaNo ratings yet