You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5814)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Kami Export - Jaden Marquez - Health Career Internet Scavenger Hunt Student Fillable UPDATED PDFDocument2 pagesKami Export - Jaden Marquez - Health Career Internet Scavenger Hunt Student Fillable UPDATED PDFjaden13% (8)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Detal Insturments Set Up PDFDocument45 pagesDetal Insturments Set Up PDFKapinya FruzsinaNo ratings yet
- Classification of Malocclusion Angle PDFDocument17 pagesClassification of Malocclusion Angle PDFAndrea Tokumoto100% (1)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Basic Mechanisms in Craniofacial GrowthDocument9 pagesBasic Mechanisms in Craniofacial GrowthFabian BarretoNo ratings yet
- Correlations of Alkaline Phosphatase Expression With Osteoblast Number During Orthodontic Tooth MovementDocument9 pagesCorrelations of Alkaline Phosphatase Expression With Osteoblast Number During Orthodontic Tooth MovementFila RachmadNo ratings yet
- Ijed 2022 03 s0340CracksGerdolleBrowetDocument17 pagesIjed 2022 03 s0340CracksGerdolleBrowetkhaled emadNo ratings yet
- Diagnosis and Treatment Plan of An Edentulous MouthDocument53 pagesDiagnosis and Treatment Plan of An Edentulous MouthKayode Ibitoye100% (5)
- 10.1007/978 3 642 28994 1 PDFDocument198 pages10.1007/978 3 642 28994 1 PDFDrMohamed AssadawyNo ratings yet
- Kim Regenerative EndodonticsDocument51 pagesKim Regenerative Endodonticsrasagna reddyNo ratings yet
- Dental Trauma Professional PamphletDocument3 pagesDental Trauma Professional Pamphletnona aryan50% (2)
- Papillary Bleeding Index in Public Health Service On Gingival in Ammation Ratna Nurlia Alfiandini 1, Chiquita Prahasanti 2, Poernomo Agoes WibisonoDocument5 pagesPapillary Bleeding Index in Public Health Service On Gingival in Ammation Ratna Nurlia Alfiandini 1, Chiquita Prahasanti 2, Poernomo Agoes WibisonoDiana Choiro WNo ratings yet
- En PeriimplantitaDocument312 pagesEn PeriimplantitaDan Țăruș100% (1)
- Gingival Inflammation in Mouth Breathing PatientsDocument5 pagesGingival Inflammation in Mouth Breathing PatientsCamiLunaNo ratings yet
- Infection Control BDADocument15 pagesInfection Control BDAMariam WaseemNo ratings yet
- Research Essay Final DraftDocument9 pagesResearch Essay Final Draftapi-670223407No ratings yet
- Presentation On: By:-Swati Nishant Tanuja Namrata Jitender RahulDocument38 pagesPresentation On: By:-Swati Nishant Tanuja Namrata Jitender RahulRahul PrakashNo ratings yet
- Inicet Nov 23 - QPDocument47 pagesInicet Nov 23 - QPPradeep SagarNo ratings yet
- Key Points: Silver Diamine FluorideDocument12 pagesKey Points: Silver Diamine FluorideFFDFNo ratings yet
- Complaints Handling - May 16Document11 pagesComplaints Handling - May 16Aainaa KhairuddinNo ratings yet
- Association Between Odontogenic Conditions and Maxillary Sinus Disease: A Study Using Cone-Beam Computed TomographyDocument7 pagesAssociation Between Odontogenic Conditions and Maxillary Sinus Disease: A Study Using Cone-Beam Computed TomographyPriliNo ratings yet
- Repair and Regeneration in Endodontics. Lin, Rosenberg. 2011Document19 pagesRepair and Regeneration in Endodontics. Lin, Rosenberg. 2011AlvaroBenítezCraveroNo ratings yet
- The Medical Technology Industry in GermanyDocument16 pagesThe Medical Technology Industry in Germanylisa braffNo ratings yet
- SDCEP Drug Prescribing Ed 3 Update June 2017Document1 pageSDCEP Drug Prescribing Ed 3 Update June 2017Mahmoud EladawyNo ratings yet
- Endodontic Considerations in The Elderly: ReviewarticleDocument10 pagesEndodontic Considerations in The Elderly: ReviewarticleYasmine SalsabilaNo ratings yet
- E InjuriesDocument15 pagesE InjuriesBasmaNo ratings yet
- Odontogenic Cysts An Update 2017 PDFDocument6 pagesOdontogenic Cysts An Update 2017 PDFFadly RasyidNo ratings yet
- 2016 Shading Concepts and Layering Techniques To Master Direct Anterior Composite Restorations An UpdateDocument8 pages2016 Shading Concepts and Layering Techniques To Master Direct Anterior Composite Restorations An Updatemaroun ghalebNo ratings yet
- Prostho Sheet 23Document13 pagesProstho Sheet 23seif nimerNo ratings yet
- 8th Seminar-Diseases of PulpDocument81 pages8th Seminar-Diseases of PulpSriya Saatwika ReddyNo ratings yet
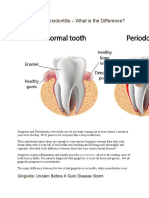
- Gingivitis Vs PeriodontitisDocument2 pagesGingivitis Vs Periodontitisandreas kevinNo ratings yet