You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Multiple SclerosisDocument4 pagesMultiple SclerosisnasibdinNo ratings yet
- Activity DesignDocument2 pagesActivity DesignRhu New Lucena90% (20)
- Handbook of Diabetes Technology 2019 PDFDocument125 pagesHandbook of Diabetes Technology 2019 PDFPradeep100% (1)
- Paediatrics Fracture 1. Physeal Injury 2. Supracondylar of Humerus Fracture 3. Paediatric AbuseDocument42 pagesPaediatrics Fracture 1. Physeal Injury 2. Supracondylar of Humerus Fracture 3. Paediatric AbuseamaniNo ratings yet
- What Is The Rate For Performing Chest Compressions For A Victim of Any Age A-30 Compressions Per Minute B - 50 Compressions Per Minute C - 80 Compressions Per MinuteDocument7 pagesWhat Is The Rate For Performing Chest Compressions For A Victim of Any Age A-30 Compressions Per Minute B - 50 Compressions Per Minute C - 80 Compressions Per MinuteHassan Shehri100% (2)
- Neonatal Intestinal ObstructionDocument21 pagesNeonatal Intestinal ObstructionShahzad Bashir ShamsNo ratings yet
- Vaccum Delivery FinalDocument31 pagesVaccum Delivery Finalsanthiyasandy75% (4)
- Ambiguous Genitalia: Comparative Role of Pelvic Ultrasonography and GenitographyDocument6 pagesAmbiguous Genitalia: Comparative Role of Pelvic Ultrasonography and GenitographyEni Maria SiscaNo ratings yet
- Pentoxyfilin Antioxi VaricoceleDocument4 pagesPentoxyfilin Antioxi VaricoceleEni Maria SiscaNo ratings yet
- Congenttal Bilateral Anorchia in Childhood: A Clinical, Endocrine and Therapeutic Evaluation Twenty-One CasesDocument11 pagesCongenttal Bilateral Anorchia in Childhood: A Clinical, Endocrine and Therapeutic Evaluation Twenty-One CasesEni Maria SiscaNo ratings yet
- Disgust Reading AssignmentDocument47 pagesDisgust Reading AssignmentEni Maria SiscaNo ratings yet
- Review Hormonal Treatment of Male Infertility: Promises and PitfallsDocument18 pagesReview Hormonal Treatment of Male Infertility: Promises and PitfallsEni Maria SiscaNo ratings yet
- Evidence-Based Approach To Unexplained Infertility: A Systematic ReviewDocument10 pagesEvidence-Based Approach To Unexplained Infertility: A Systematic ReviewEni Maria SiscaNo ratings yet
- Genetic Causes of Male Infertility: Plaseska-Karanfilska D, Noveski P, Plaseski T, Maleva I, Madjunkova S, Moneva ZDocument4 pagesGenetic Causes of Male Infertility: Plaseska-Karanfilska D, Noveski P, Plaseski T, Maleva I, Madjunkova S, Moneva ZEni Maria SiscaNo ratings yet
- Presetation37 MCQDocument16 pagesPresetation37 MCQBishoy Emile100% (2)
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Document2 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)gopimicroNo ratings yet
- Faktor-Faktor Risiko Hipertensi Intrahemodialisis Pada Pasien Gagal Ginjal Kronis Stadium 5 Di RSUD Al-Ihsan BandungDocument6 pagesFaktor-Faktor Risiko Hipertensi Intrahemodialisis Pada Pasien Gagal Ginjal Kronis Stadium 5 Di RSUD Al-Ihsan BandungmayyfajrianiiNo ratings yet
- What Is CardiomyopathyDocument8 pagesWhat Is CardiomyopathysakuraleeshaoranNo ratings yet
- Quotation ENHANCED 2 - PLAN 4 - Essential AafiyaDocument24 pagesQuotation ENHANCED 2 - PLAN 4 - Essential AafiyaMelody PacardoNo ratings yet
- Journal of Dental Research: Regional Anesthesia in Dental and Oral Surgery: A Plea For Its StandardizationDocument15 pagesJournal of Dental Research: Regional Anesthesia in Dental and Oral Surgery: A Plea For Its StandardizationFerdina NidyasariNo ratings yet
- Appendix 2: List of High Alert MedicationDocument7 pagesAppendix 2: List of High Alert MedicationhanselMDNo ratings yet
- Elisee 350 Product Brochure EngDocument4 pagesElisee 350 Product Brochure EngWidad Mardin Mas JayaNo ratings yet
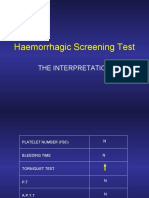
- Haemorrhagic Screening Test: The InterpretationDocument40 pagesHaemorrhagic Screening Test: The InterpretationAngel 冯晓君No ratings yet
- Claim Form-MD IndiaDocument5 pagesClaim Form-MD IndiaMusycal FynncNo ratings yet
- SahodayaQP Psychology Set1 Term2Document3 pagesSahodayaQP Psychology Set1 Term2Nishtha JainNo ratings yet
- AHM Black White Boost FlexiDocument10 pagesAHM Black White Boost FlexiDani Kirky Ylagan100% (1)
- Schizophrenia Research PaperDocument12 pagesSchizophrenia Research Paperapi-534301945No ratings yet
- 2 Wilkes1989Document9 pages2 Wilkes1989LAURA MARCELA BARRENECHE CALLENo ratings yet
- NCP - OsteomyelitisDocument2 pagesNCP - OsteomyelitisGave gonzalesNo ratings yet
- Galvanic Current: Avanianban Chakkarapani K 342 30.01.2015 11.00 Am To 12.00 PMDocument22 pagesGalvanic Current: Avanianban Chakkarapani K 342 30.01.2015 11.00 Am To 12.00 PMLoganathan ChandrasekarNo ratings yet
- Cassava Manioc HydroxiCoumarin - Scopoletin Suppresses Activation of Dendritic Cells and Pathogenesis of Experimental Autoimmune Encephalomyelitis by Inhibiting NF-κB SignalingDocument14 pagesCassava Manioc HydroxiCoumarin - Scopoletin Suppresses Activation of Dendritic Cells and Pathogenesis of Experimental Autoimmune Encephalomyelitis by Inhibiting NF-κB SignalingMiguel AngelNo ratings yet
- Basic ECG InterpretationDocument62 pagesBasic ECG Interpretationmohannadalkwiese3No ratings yet
- 06 - Lec - Stress ReactionsDocument2 pages06 - Lec - Stress Reactionsericka abasNo ratings yet
- Liver Fibrosis A Compilation On The Biomarkers StaDocument17 pagesLiver Fibrosis A Compilation On The Biomarkers Stamy accountNo ratings yet
- Management TTPDocument14 pagesManagement TTPSutirtho MukherjiNo ratings yet
- 1.10 Decision Making in Pelvic Fractures When To Conserve or OperateDocument65 pages1.10 Decision Making in Pelvic Fractures When To Conserve or OperateThế Kiên PhạmNo ratings yet
- Medicine IMM SyllabusDocument53 pagesMedicine IMM SyllabusAamir HamaadNo ratings yet