You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Sensory Analysis v2 2Document16 pagesSensory Analysis v2 2Alyssa BalverdeNo ratings yet
- Laban - Sub Kamal Salman Mahmoud Jaber Mustafa: Done byDocument40 pagesLaban - Sub Kamal Salman Mahmoud Jaber Mustafa: Done byKool Kaish100% (1)
- 2 Neurophysiology of Somatic Sensations 2012Document6 pages2 Neurophysiology of Somatic Sensations 2012Nephritery Joy Espiritu JimenezNo ratings yet
- Visual Acuity: Noeh O. Fernandez JR., OD, MatsDocument46 pagesVisual Acuity: Noeh O. Fernandez JR., OD, MatsJan IrishNo ratings yet
- Science 1stQ Lesson 1 - Sense Organs (Eyes and Ears)Document23 pagesScience 1stQ Lesson 1 - Sense Organs (Eyes and Ears)Veronica RayosNo ratings yet
- Color Wheel Cheat SheetDocument1 pageColor Wheel Cheat SheetRhiannon MorseNo ratings yet
- Sub - Medical Surgical Nursing: Assignment On Neurological AssessmentDocument11 pagesSub - Medical Surgical Nursing: Assignment On Neurological Assessmentkamini Choudhary100% (1)
- Sensory PhysiologyDocument57 pagesSensory PhysiologyeryxspNo ratings yet
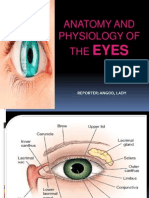
- Anatomy and Physiology of The EyesDocument20 pagesAnatomy and Physiology of The EyesLaidy Aizahlyn Indoc Angod100% (2)
- The Five Human SensesDocument17 pagesThe Five Human SensesAntonio Gonzalez100% (1)
- Anatomy of Ear 1Document18 pagesAnatomy of Ear 1VikrantNo ratings yet
- Tastes FlashcardsDocument4 pagesTastes FlashcardsBiel Isern Ubach100% (2)
- Clinical Tests For Binocular Vision: John Lee and Ann McintyreDocument4 pagesClinical Tests For Binocular Vision: John Lee and Ann McintyreRaissaNo ratings yet
- The Haas EffectDocument2 pagesThe Haas EffectIzzy BlaoNo ratings yet
- KMY4013 LU4 Sensory PerceptionDocument31 pagesKMY4013 LU4 Sensory PerceptionimanNo ratings yet
- PBS Band 6 - ScienceDocument9 pagesPBS Band 6 - ScienceDienta Alias100% (6)
- STRABISMDocument30 pagesSTRABISMCindy ChristensenNo ratings yet
- 2 5 Applications of SoundDocument9 pages2 5 Applications of SoundjemwesleyNo ratings yet
- Physics of The EyeDocument3 pagesPhysics of The EyePhilip MooreNo ratings yet
- Color Wheel For KidsDocument2 pagesColor Wheel For KidsSabrina CancroNo ratings yet
- Colour Theory by Sai Prasad PoojariDocument41 pagesColour Theory by Sai Prasad PoojariSaiprasad PoojariNo ratings yet
- Consumer Perception and PositioningDocument2 pagesConsumer Perception and PositioningVivek RawatNo ratings yet
- Sensing and Perceiving: Sensation PerceptionDocument33 pagesSensing and Perceiving: Sensation PerceptionmarioNo ratings yet
- ENT Basics Corectat 2Document322 pagesENT Basics Corectat 2Ioana RastianNo ratings yet
- Cataract SenilisDocument54 pagesCataract Senilismayo djitroNo ratings yet
- Colour Difference Formulae Past Present and FutureDocument3 pagesColour Difference Formulae Past Present and FutureeonerNo ratings yet
- Structure and Function of The Human EyeDocument10 pagesStructure and Function of The Human EyeSyed MujtabaNo ratings yet
- ENT AyaSalahEldeenDocument147 pagesENT AyaSalahEldeenFatma ShnewraNo ratings yet
- 53 1002059 01 German RegStmntDocument10 pages53 1002059 01 German RegStmntHam ZaNo ratings yet
- MS1907192314 - Balamurugan Annamalai - Second ProofDocument17 pagesMS1907192314 - Balamurugan Annamalai - Second Proofdebojyoti0% (1)