Professional Documents
Culture Documents
AJGP163Gitlin TAP
AJGP163Gitlin TAP
Uploaded by
Tung Wah CollegeOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
AJGP163Gitlin TAP
AJGP163Gitlin TAP
Uploaded by
Tung Wah CollegeCopyright:
Available Formats
See discussions, stats, and author profiles for this publication at: https://www.researchgate.
net/publication/24406365
The Tailored Activity Program to Reduce Behavioral Symptoms in Individuals
With Dementia: Feasibility, Acceptability, and Replication Potential
Article in The Gerontologist · July 2009
DOI: 10.1093/geront/gnp087 · Source: PubMed
CITATIONS READS
121 3,650
7 authors, including:
Laura N Gitlin Tracey Vause Earland
Drexel University Thomas Jefferson University
462 PUBLICATIONS 13,670 CITATIONS 17 PUBLICATIONS 295 CITATIONS
SEE PROFILE SEE PROFILE
E Adel Herge Nancy L Chernett
Thomas Jefferson University Thomas Jefferson University
19 PUBLICATIONS 196 CITATIONS 19 PUBLICATIONS 496 CITATIONS
SEE PROFILE SEE PROFILE
Some of the authors of this publication are also working on these related projects:
The Power of Communication: Evaluating a Communication Training Program in a Skilled Nursing Facility View project
WeCareAdvisor™ View project
All content following this page was uploaded by Laura N Gitlin on 26 May 2014.
The user has requested enhancement of the downloaded file.
Tailored Activities to Manage
Neuropsychiatric Behaviors in Persons
With Dementia and Reduce Caregiver
Burden: A Randomized Pilot Study
Laura N. Gitlin, Ph.D., Laraine Winter, Ph.D.,
Janice Burke, Ph.D., OTR/L, FAOTA, Nancy Chernett, MPH,
Marie P. Dennis, Ph.D., Walter W. Hauck, Ph.D.
Objective: To test whether the Tailored Activity Program (TAP) reduces dementia-related
neuropsychiatric behaviors, promotes activity engagement, and enhances caregiver well-
being. Design: Prospective, two-group (treatment, wait-list control), randomized, con-
trolled pilot study with 4 months as main trial endpoint. At 4 months, controls received
the TAP intervention and were reassessed 4 months later. Setting: Patients’ homes.
Participants: Sixty dementia patients and family caregivers. Intervention: The eight-
session occupational therapy intervention involved neuropsychological and functional
testing, selection, and customization of activities to match capabilities identified in
testing, and instruction to caregivers in use of activities. Measurements: Behavioral
occurrences, activity engagement, and quality of life in dementia patients; objective and
subjective burden and skill enhancement in caregivers. Results: At 4 months, compared
with controls, intervention caregivers reported reduced frequency of problem behaviors,
and specifically for shadowing and repetitive questioning, and greater activity engage-
ment including the ability to keep busy. Fewer intervention caregivers reported agitation
or argumentation. Caregiver benefits included fewer hours doing things and being on
duty, greater mastery, self-efficacy, and skill enhancement. Wait-list control participants
following intervention showed similar benefits for reductions in behavioral frequency
and caregiver hours doing things for the patient and mastery. Caregivers with depressed
symptoms derived treatment benefits similar to nondepressed caregivers. Conclusions:
Tailoring activities to the capabilities of dementia patients and training families in
activity use resulted in clinically relevant benefits for patients and caregivers. Treatment
minimized trigger behaviors for nursing home placement and reduced objective care-
giver burden. Noteworthy is that depressed caregivers effectively engaged in and bene-
fited from the intervention. (Am J Geriatr Psychiatry 2008; 16:229 –239)
Key Words: Dementia caregiving, activity engagement, disruptive behaviors
Received April 23, 2007; revised September 27, 2007; accepted October 19, 2007. From the Center for Applied Research on Aging and Health
(CARAH) (LNG, LW, NC, MPD); School of Health Professions (JB) and the Department of Occupational Therapy (JB), Thomas Jefferson University,
Philadelphia, Pennsylvania; Sycamore Consulting, LLC, New Hope, Pennsylvania (WWH). Research reported in this article was supported in part
by funds from the National Institute of Mental Health (grant no. R21 MH069425). The authors acknowledge the significant contributions of
consultants, Dr. Cameron Camp and Ms. Adel Herge, MS, OTR/L, the interventionists Geri Shaw, OTR/L, Tracey Vause-Earland, MS, OTR/L;
Michele Rifkin, MS, OTR/L; Catherine Piersol, MS, OTR/L; and Lauren Young Lapin, MS, OTR/L and the interviewing staff. Clinical Trials ID#
NCT00259467. Send correspondence and reprint requests to Laura N. Gitlin, Ph.D., Director, Center for Applied Research on Aging and Health,
Thomas Jefferson University, 130 S.9th Street, Suite 513, Philadelphia, PA 19107. e-mail: laura.gitlin@jefferson.edu
© 2008 American Association for Geriatric Psychiatry
Am J Geriatr Psychiatry 16:3, March 2008 229
Tailored Activity Program for Persons With Dementia
M ore than 5.1 million Americans have dementia,
a progressive and irreversible neurodegenera-
tive disorder, with this number expected to increase
wait-list controls received the TAP intervention and
were retested 4 months later (8 months from base-
line). This allowed for estimation of effect sizes using
to more than 14 million by 2050.1 Neuropsychiatric a randomized two-group design at 4 months, confir-
behaviors such as apathy, depressed affect, lability, mation of treatment gains for wait-listed participants
agitation, and aggressiveness are common, with (4 – 8 months), and evaluation of program acceptabil-
most patients manifesting behaviors with disease ity for all 60 dyads. We hypothesized that relative to
progression.2– 4 Behaviors are the most challenging controls at 4 months, intervention caregivers would
aspect of caregiving, contributing to caregiver dis- report reduced behavioral occurrences and enhanced
tress, depression, increased care costs, and risk for activity engagement for dementia patients, and re-
nursing home placement.5– 8 Few studies test inter- duced caregiver burden, enhanced mastery, confi-
ventions to minimize behavioral occurrences, and dence, and skill. We predicted similar benefits for
recent research suggests that pharmacologic ap- wait-list controls at 8 months.
proaches are not effective and may cause harm.9 –11
Only a few interventions targeting caregivers report
behavioral benefits in patients,12–14 whereas most
studies do not examine15 or find symptom reduc-
METHODS
tions.16 Developing and testing nonpharmacologic
approaches to manage behaviors remains an impor- Study Sample and Procedures
tant public health priority.17,18
One promising approach is activity. Research Participants were recruited between 2005 and 2006
shows that purposeful activity results in reductions through media announcements and social service
of depressive and agitated-type behaviors.19 –21 How- mailings. Interested caregivers contacted the re-
ever, this research involves nursing home residents, search office, were explained study procedures, and
small sample sizes, and nonexperimental designs, administered a telephone eligibility screening test.
and it has not evaluated systematic approaches to Dementia patients were English-speaking, had a phy-
developing activities. The paucity of research with sician diagnosis or Mini-Mental State Examination
community-living patients is significant given that the (MMSE) score ⬍24,22 and were able to feed self and
home is the primary care setting for this population. participate in at least two self-care activities (e.g.,
This controlled pilot study evaluated the Tailored bathing, dressing). Patients were excluded if they
Activity Program (TAP), which was designed to re- had schizophrenia, bipolar disorder, or dementia
duce behavioral disturbances by identifying patients’ secondary to head trauma, had an MMSE score ⫽ 0
preserved capabilities and previous roles and inter- and were bed-bound (confined to bed or chair) or
ests, and devising activities that build on them. The nonresponsive (unable to understand short com-
trial also tested whether tailored activities en- mands). Caregivers were English-speaking, ⱖ21
hanced patient engagement, reduced caregiver years of age, lived with the patient, provided ⱖ4
burden, and improved caregiver mastery, self-effi- hours of daily care, and reported dementia patient’s
cacy, and use of effective communication and sim- boredom, sadness, anxiety, agitation, restlessness, or
plification strategies. Because TAP is based on ac- trouble focusing on a task. Caregivers involved in
tive involvement of caregivers, it may be overwhelming another study, seeking nursing home placement, ter-
for distressed caregivers. Thus, we examined whether minally ill, in active cancer treatment, or with three
depressed caregivers benefited less than nonde- or more hospitalizations in the past year were ex-
pressed caregivers by testing moderating effects of cluded.
caregiver depressive symptoms on study outcomes. Of 84 caregivers screened by telephone, 65 (77%)
Using a two-group parallel design, 60 dyads (de- were eligible, and 60 (92%) were willing to partici-
mentia patients and caregivers) were randomly as- pate. Within 48 hours of baseline, dyads were ran-
signed to treatment or wait-list control. Treatment domized using random permuted blocks to control
group participants received TAP, and all dyads were for possible changes in subject mix over time. The
reassessed at 4 months from baseline. At that point, blocking number, developed by the project statisti-
230 Am J Geriatr Psychiatry 16:3, March 2008
Gitlin et al.
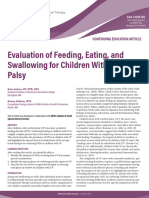
FIGURE 1. Consort Flow Chart of Subject Recruitment and Attrition
No. Screened for Eligibility
(N = 84)
Eligible Ineligible
(N = 65) (N = 19)
Unwilling Randomized
(N = 5) (N = 60)
Intervention Control
(N = 30) (N = 30)
Lost to Included in Lost to Included in
Follow-up 4-month analysis Follow-up 4-month
(N = 3) (N = 27) (N = 1) analysis
(N = 29)
cian, remained unknown to others. All dyads were ing, placemat task, sensory-based tests).27–29 Three
interviewed at 4 months by interviewers masked to activities per patient were developed based on as-
group assignment and with no intervention role. Of sessments that identified cognitive capacities in areas
60 dyads at baseline, four (7%) terminated because of of memory, language, conceptualization, attention,
patient death (Fig. 1). construction, and initiation, and also evaluated cue-
ing requirements, ability to follow directions and
Intervention Group problem solve, and prior interests and roles (e.g.,
homemaker, carpenter). The interventionist devel-
TAP is based on the environmental vulnerability
oped a brief written plan (Activity Prescription)
or reduced stress-threshold model, positing that with
specifying patient capabilities, the target activity
disease progression, dementia patients become in-
(e.g., completing a puzzle form board) and goal (e.g.,
creasingly vulnerable to their environment and ex-
engage in activity 20 minutes daily after breakfast),
perience lower thresholds for tolerating stimuli.23,24
and implementation techniques (see Appendix). Ac-
The intervention addressed vulnerability by devel-
oping activities that matched performance capabili- tivities ranged in complexity from multistep (making
ties and decreasing environmental demands to facil- salad, simple woodworking) to one-to-two step (sort-
itate participation. ing beads, bean toss game), to sensory-oriented
TAP involved six 90-minute home visits and two (viewing videos, listening to music). Caregivers, and
15-minute telephone contacts by occupational thera- when appropriate dementia patients, chose one ac-
pists over 4 months. Interventionists met with care- tivity prescription to implement initially. The pre-
givers, introduced intervention goals, used a semi- scription was reviewed and the activity introduced
structured clinical interview and the Pleasant Event through role play or direct demonstration with pa-
Schedule25 to identify previous and current activity tients. Caregivers were instructed in stress-reducing
interests, observed dyadic communication and home techniques (deep breathing) to establish a calm emo-
environmental features, and assessed dementia pa- tional tone. Once an activity was mastered, another
tients using the Dementia Rating Scale26 and Allen’s was introduced. In each session, prescriptions were
observational craft-based assessments (leather lac- reviewed and modified if necessary. As caregivers
Am J Geriatr Psychiatry 16:3, March 2008 231
Tailored Activity Program for Persons With Dementia
mastered activity use, interventionists generalized present; 1 ⫽ present; 2 ⫽ severe) of caregiver and
strategies to care problems and instructed them on patient. Scores represented the sum of composite
how to downgrade activities for future declines. scores (Cronbach ␣ ⫽ 0.76 for this sample).
Activity engagement was measured using a five-
Measures item, investigator-developed index of caregiver re-
port of patient in past 2 weeks (“Enjoyed doing
Background characteristics of dyads included age, activities”; “Showed signs of pleasure or enjoyment”)
income, education, and years providing care mea- from 1 ⫽ “Never” to 3 ⫽ “Often.” Scores represented
sured as continuous variables. Gender, dyadic rela- mean ratings across five items (with one reverse
tionship (spouse or nonspouse), race (white or non- coded), with higher scores indicating greater engage-
white), and marital status (currently married or not ment (␣ ⫽ 0.54).
married) were measured as dichotomous variables. We used the well-established 12-item Quality of
Life-AD scale to assess caregiver perceptions of life
Dementia Patient Outcomes quality in dementia patients.33 Responses ranged
from 1 ⫽ “Poor” to 4 ⫽ “Excellent.” We examined
The primary outcome was frequency of occurrence
item-level scores for one item in particular, ability to
of 24 behaviors: 16 from the Agitated Behaviors in
keep busy, and overall mean response, with higher
Dementia Scale,30 2 (repetitive questioning, hiding or
scores indicating better life quality (␣ ⫽ 0.72).
hoarding) from the Revised Memory and Behavior
Problem Checklist,31 4 (wandering, incontinent inci-
dents, shadowing, boredom) from previous research
Caregiver Outcomes
showing these behaviors as common and distressful,13
and 2 “others” identified by families that could not We used psychometrically sound measures for
be coded elsewhere. For each behavior, caregivers mastery,34 a five-item Likert (1 ⫽ never to 5 ⫽ al-
indicated occurrence (yes or no) and, if yes, fre- ways) scale (␣ ⫽ 0.70); subjective burden, measured
quency in past month. Two indices were created: as upset with behaviors (1 ⫽ no upset to 8 ⫽ extreme
number of behaviors occurring (␣ ⫽ 0.86) and mean upset);35 and the 10-item Zarit Burden Scale36 (␣ ⫽
frequency of occurrence (main study endpoint). Be-
0.89); objective burden, measured by caregiver esti-
haviors reported by caregivers as occurring “con-
mate of real time spent “on duty” and “doing things”
stantly” (repetitive questioning) were assigned a
for dementia patients.37
score of 300, representing the largest number of re-
Caregiver depression was measured by the 20-
ported occurrences across all subjects and behaviors
item CES-D scale38 with symptoms rated as occur-
(except for one subject who specified “600” times for
ring in the past week (0 ⫽ less than 1 day to 3 ⫽ 5–7
one behavior). Two caregivers reported one or more
days). Scores represented summed responses, with
behaviors as “constant” at baseline and seven did so
higher scores indicating greater symptomatology
at 4 months. We tested other coding schemes for the
“constant” value including recoding the 600 score to (␣ ⫽ 0.91).
300, and in separate analyses, recoding all “con- Confidence using activities during the past
stants” to 600. Because outcomes were similar re- month (0 ⫽ not confident to 10 ⫽ very confident)
gardless of coding, we report results for the original was measured by five investigator-developed
coding described above. A secondary outcome was items. Scores were averaged across items, with
the proportion of caregivers reporting occurrence higher mean ratings indicating greater confidence
(yes or no) of each behavior. (␣ ⫽ 0.72).
We used the 19-item Cornell Scale for Depression Skill enhancement was measured using the 19-
in Dementia to rate depressive symptoms.32 The Cor- item Task Management Strategy Index.39 Caregivers
nell Scale for Depression in Dementia was adminis- indicated frequency of strategy (cueing, simplifying
tered to dementia patients and caregivers, each of routines) use (1 ⫽ never to 5 ⫽ always). A mean
whom responded independently. Composite scores strategy use score was calculated, with high scores
per item were based on combined ratings (0 ⫽ not indicating greater use (␣ ⫽ 0.80).
232 Am J Geriatr Psychiatry 16:3, March 2008
Gitlin et al.
Treatment Documentation a similar analytic strategy as for main effect models
(ANCOVAs with same covariates as described
For each session, interventionists documented
above). We then added an interaction term (treat-
time spent, who participated (caregiver, patient), and
ment group by baseline CES-D score).
number of activities introduced. After the final ses-
To evaluate whether control group participants
sion, interventionists rated the extent to which pa-
derived similar benefits to the experimental group
tients appeared agitated (not at all, somewhat, very
after receiving TAP, we compared 4 (T2) to 8 (T3)
much), resisted participation, demonstrated plea-
month scores of controls to baseline (T1) to 4 (T2)
sure, and extent to which caregivers demonstrated
month scores of experimental group participants on
understanding of strategies, viewed the intervention
statistically significant outcomes from main analyses,
as useful, and reported strategy benefits (benefit, no
using the methods described above. We anticipated
difference or made matters worse).
that the magnitude of the difference between exper-
imental and control group treatment effects would
Data Analysis be similar and thus, not statistically significant. SPSS
version 15.0 was used with a significance level of
Descriptive data included sociodemographic 0.05. All analyses were two-sided. Analyses followed
characteristics (age, gender, race, education, rela- intention-to-treat such that all subjects providing
tionship), health conditions, self-rated health, eco- data were included in analyses regardless of study
nomic well-being, cognitive status, depressive participation level.
symptoms, ADL/IADL functioning, and treatment
characteristics. 2 and Mann-Whitney tests were
used to compare experimental and control dyads
on characteristics. Means, standard deviations, and RESULTS
ranges for outcome measures and treatment char-
Dementia patients were primarily male (57%) and
acteristics were computed.
white (77%), with a mean age of 79 years. On average
Main treatment effects for patient behavior and
they had a MMSE score of 11.6, were dependent in
caregiver outcomes at 4 months were examined us-
eight instrumental and five basic activities of living.
ing analysis of covariance (ANCOVA). To increase
Caregivers were primarily female (88%), white
precision of treatment comparisons, baseline values,
(77%), high school graduates (56%), and spouses
cognitive status and number of patient functional
(62%) with a mean age of 65 (Table 1).
dependencies, caregiver age, gender, education, and
relationship to patient were selected a priori as co-
Treatment Implementation
variates based on previous research showing signif-
icant associations between these factors and out- Consistent with intervention intent, nearly eight
comes. Cohen’s d was determined as a measure of contacts were completed, with approximately six
effect size. sessions face-to-face and two by telephone. Average
The distribution of residuals from the ANCOVAs time spent was 1 hour per home visit and 15 minutes
was examined for outcomes and found to be skewed for telephone contacts. Most home contacts (mean:
for overall behavior frequency, frequency of five be- 5.13, SD: 1.36) involved patients and caregivers, and
haviors (agitation, refusing care, repetitive question- an average of 2.4 (SD: 1.1) activities were introduced.
ing, hoarding, and shadowing), and objective burden Wait-list controls had similar implementation pro-
(hours doing things; hours on duty). Log transfor- files. An average of $70 per participant was spent
mations improved distributions. (range: $0 –129) for materials (e.g., activity boards,
Additional analyses examined the proportion of beads, organizing bins).
caregivers reporting each behavior (occurrence or no
occurrence), using logistic regression with covariates Four Month Patient Outcomes
described above.
To evaluate differential effects at 4 months based We found a treatment effect for frequency of behav-
on caregiver baseline depressive symptoms, we used ioral occurrences overall, F(1,41) ⫽ 7.58, Cohen’s d ⫽
Am J Geriatr Psychiatry 16:3, March 2008 233
Tailored Activity Program for Persons With Dementia
TABLE 1. Demographic Characteristics of Sample
Wait-list Control Experimental Total
Characteristics (n ⴝ 30) (n ⴝ 30) (n ⴝ 60) Range 2 Zd p
Dementia patient
Age, Mean (SD)a 80.8 (9.5) 78.0 (9.2) 79.4 (9.4) 56.0–96.2 ⫺1.30 0.192
Gender (%) 1.07 0.297
Male 63.3 50.0 56.7
Female 36.7 50.0 43.3
Race (%) 1.16 0.559
White 80.0 73.3 76.7
African American 20.0 23.3 21.7
Other 0.0 3.3 1.6
Education (%)b 1.16 0.559
⬍HS 60.7 48.3 54.4
⬍College 25.0 37.9 31.6
Graduate degree 14.3 13.8 14.0
MMSE, Mean (SD)c 12.2 (8.8) 11.0 (7.3) 11.6 (8.1) 0.0–27.0 ⫺0.72 0.473
CSDD, Mean (SD) 8.1 (4.5) 9.2 (5.1) 8.7 (4.8) 1.0–20.0 ⫺0.68 0.495
ADL 4.37 (2.1) 4.6 (2.3) 4.5 (2.2) 0.0–7.0 ⫺0.63 0.529
IADL 7.4 (1.2) 7.8 (.5) 7.6 (.9) 3.0–8.0 ⫺0.84 0.401
Self-rated health 3.2 (1.0) 3.2 (.9) 3.2 (.9) 1.0–5.0 ⫺0.23 0.815
Caregiver
Age, Mean (SD) 67.9 (10.6) 62.8 (11.3) 65.4 (11.1) 47.2–89.7 ⫺1.99 0.047
Gender (%) 1.46 0.228
Male 6.7 16.7 11.7
Female 93.3 83.3 88.3
Race (%) 1.16 0.559
White 80.0 73.4 76.7
African American 20.0 23.3 21.7
Other 0.0 3.3 1.6
Education (%)a .263 0.877
⬍HS 24.2 30.0 27.2
⬍College 58.6 53.3 55.9
Graduate degree 17.2 16.7 16.9
Relationship to Patient (%) 1.76 0.184
Spouse 70.0 53.3 61.7
Nonspouse 30.0 46.7 38.3
Financial Difficulty, Mean (SD) 2.0 (1.0) 1.7 (.8) 1.9 (.9) 1.0–4.0 ⫺1.30 0.195
Health, Mean (SD)
Self-rated health 9.0 (2.0) 1.7 (.8) 9.0 (2.3) 3.0–12.0 ⫺0.33 0.742
Health behaviors 3.0 (1.5) 2.8 (1.7) 2.9 (1.6) 0.0–5.0 ⫺0.49 0.625
Notes: MMSE: Mini-Mental Status Examination; CSDD: Cornell Scale for Depression in Dementia; ADL: Activities of Daily Living; IADL:
Instrumental ADL.
a
N ⫽ 59; bN ⫽ 57; cN ⫽ 58; dMann-Whitney test.
0.72 (Table 2), and two behaviors specifically, shadow- difference did not reach statistical significance. We
ing, F(1,4) ⫽ 58.9, p ⫽ 0.003, Cohen’s d ⫽ 3.10 and did find statistically significant reductions in the
repetitive questioning, F(1,22) ⫽ 5.94, p ⫽ 0.023, Co- number of TAP caregivers reporting agitation, Wald
hen’s d ⫽1.22, reaching statistical significance (not 2(1) ⫽ 6.0, Cohen’s d ⫽ 0.75, and argumentation,
shown in Table 2) for the 13 and 31 caregivers, respec- Wald 2(1) ⫽ 6.6, Cohen’s d ⫽ 0.77, compared with
tively, reporting these two behaviors. Experimental controls.
caregivers reported greater activity engagement,
F(1,43) ⫽ 5.1, Cohen’s d ⫽ 0.61, and ability to keep Four Month Caregiver Outcomes
busy, F(1,43) ⫽ 6.2, Cohen’s d ⫽ 0.71. No effects were
found for depressed mood or overall life quality. Experimental group caregivers reported fewer
Whereas overall number of behaviors reported to hours doing things for patients, F(1,42) ⫽ 8.8, Co-
occur increased for control patients, the number de- hen’s d ⫽ 1.14, approximately 1 hour less, whereas
creased slightly for TAP participants, although this control group caregivers reported 2 hours more by 4
234 Am J Geriatr Psychiatry 16:3, March 2008
Gitlin et al.
TABLE 2. Outcomes for Experimental and Wait List Control Group Dementia Patients at Four Months (N ⴝ 56)a
Experimental (N ⴝ 27), Control (N ⴝ 29), Adjusted Mean
Mean (SD) Mean (SD) Effect at 4
Dependent Variable Baseline 4 Months Baseline 4 Months Monthse p 95% CI d
Behavioral Occurrences 30.5 (30.3) 18.8 (17.6) 41.5 (70.5) 60.8 (85.3) ⫺0.32b 0.009 ⫺0.55, ⫺0.09 0.72
Number of behaviors 8.0 (3.8) 7.2 (4.1) 7.5 (4.5) 7.7 (3.7) ⫺0.98 0.249 ⫺2.67, 0.71
CSDD 9.2 (5.1) 9.0 (4.6) 8.1 (4.5) 8.7 (4.7) ⫺1.10 0.340 ⫺3.39, 1.19
Activity engagement 2.1 (0.4) 2.3 (0.3) 1.9 (0.4) 2.0 (0.4) 0.22 0.029 0.02, 0.41 0.61
Pleasure in recreation 2.4 (0.6) 2.6 (0.5) 2.2 (0.7) 2.1 (0.7) 0.38 0.045 0.01, 0.74 0.64
Quality of Life Scale 2.2 (0.3) 2.4 (0.4) 2.0 (0.4) 2.1 (0.5) 0.18 0.095 ⫺0.03, 0.40
Ability to keep busy 1.6 (0.9) 2.2 (0.7) 1.7 (0.8) 1.6 (0.9) 0.56 0.017 0.11, 1.01 0.71
Specific Behaviorsc % B SE Wald 2 Exp (B) p 95% CI for Exp (B) d
Agitatedd 30.4 ⫺2.89 1.18 6.00 0.06 0.014 0.01, 0.56 0.75
Arguingd 44.6 ⫺2.51 0.98 6.55 0.08 0.010 0.01, 0.56 0.77
Notes: CSDD: Cornell Scale for Depression in Dementia.
a
All analyses were adjusted for baseline value, care recipient cognitive status (MMSE) and number of ADL dependencies, caregiver age, gender,
education, relationship to the care recipient. bAdjusted mean effect and confidence intervals are based on log transformed values. cBinary logistic
regressions were used to analyze the behavior data; values are for main effects of treatment. dHosmer and Lemeshow test of goodness of fit ⫽
0.685 and 0.638, respectively. eANCOVA.
months. Experimental caregivers also reported fewer (CES-D ⱖ16; 36.7% of sample), and nondepressed
hours on duty, F(1,42) ⫽ 15.8, Cohen’s d ⫽ 1.01, (CES-D ⬍16) caregivers benefited similarly on ma-
approximately 5 hours less, whereas control partici- jor outcomes.
pants reported 2 hours more. Also, experimental
caregivers reported greater mastery, F(1,43) ⫽ 6.7,
Control Group Outcomes Following Treatment
Cohen’s d ⫽ 0.55, enhanced self-efficacy using activ-
ities, F(1,43) ⫽ 7.1, Cohen’s d ⫽ 0.74, and greater use A comparison of adjusted mean effects between
of simplification techniques, F(1,43) ⫽ 5.5, Cohen’s experimental (T1–T2) and wait-list controls (T2–T3)
d ⫽ 0.71, compared with controls (Table 3). We did showed similar benefits for behavior frequency,
not find a statistically significant treatment effect for F(1,42) ⫽ 2.7, p ⬍0.105 (adjusted mean effect: ⫺0.25,
subjective burden. CI [confidence interval]: ⫺0.42 to ⫺0.08), and care-
Caregiver baseline depressive symptom scores giver hours doing things for patients, F(1,37) ⫽ 0.4,
did not moderate treatment outcomes. Depressed p ⬍0.547 (adjusted mean effect: ⫺0.04, CI: ⫺0.16 –
TABLE 3. Outcomes for Experimental and Wait List Control Group Caregivers at 4 Months (N ⴝ 56)a
Experimental (N ⴝ 27), Control (N ⴝ 29), Adjusted Mean
Mean (SD) Mean (SD) Effect at 4
Dependent Variable Baseline 4 Months Baseline 4 Months Monthsc p 95% CI d
Subjective burden
Behavior upset 4.5 (1.9) 4.5 (1.8) 4.6 (3.0) 4.8 (2.5) ⫺0.01 0.984 ⫺1.21, 1.18
Burden 21.0 (9.0) 20.3 (8.8) 21.3 (9.2) 20.6 (10.4) 0.75 0.715 ⫺3.36, 4.85
CES-D 14.6 (11.0) 13.1 (9.4) 13.2 (9.6) 14.3 (10.2) ⫺0.74 0.676 ⫺4.31, 2.82
Objective burden
Hours doing for patient 6.3 (4.3) 5.4 (2.5) 6.2 (3.3) 8.6 (5.7) ⫺0.22b 0.005 ⫺0.36, ⫺0.07 1.14
Hours feel on duty 18.2 (7.3) 13.4 (7.6) 15.5 (7.7) 17.6 (7.1) ⫺0.25b 0.001 ⫺0.37, ⫺0.12 1.01
Caregiver skill
Mastery 3.4 (.5) 3.7 (.6) 3.7 (.6) 3.7 (.6) 0.34 0.013 0.08, 0.60 0.55
Confidence using activities 5.4 (1.9) 7.4 (1.9) 6.2 (1.7) 6.4 (2.5) 1.67 0.011 0.41, 2.94 0.74
Task simplification use 3.0 (.6) 3.2 (.5) 2.8 (.5) 2.9 (.6) 0.25 0.023 0.04, 0.46 0.71
Notes: CES-D: Center for Epidemiological Scale for Depression.
a
All analyses were adjusted for baseline value, care recipient cognitive status (MMSE), number of ADL dependencies, caregiver age, gender,
education, and relationship to the care recipient. bAdjusted mean effect and confidence intervals are based on log transformed values. cANCOVA.
Am J Geriatr Psychiatry 16:3, March 2008 235
Tailored Activity Program for Persons With Dementia
0.07), and mastery, F(1,38) ⫽ 1.4, p ⬍0.244 (adjusted an intervention targeting subjective well-being may
mean effect: 0.17, CI: ⫺0.07– 0.41). Compared with 4 complement TAP. Additional caregiver benefits in-
month outcomes for the experimental group, control cluded enhancements in skills, mastery, and confi-
group participants showed no benefits in activity dence using activities.
engagement, caregiver hours on duty, confidence, or Equally important is that TAP was well tolerated
strategy use. by patients and caregivers as suggested by interven-
tionists’ ratings of engagement in treatment sessions.
Although interventionists’ ratings are potentially bi-
Acceptability of TAP
ased, low attrition and high session participation
For all dyads (N ⫽ 60), interventionists reported rates testify to intervention acceptability. Further-
that 69.6% of patients were engaged “very much,” more, depressed caregivers benefited similarly as
with 30.4% engaging “somewhat,” 67% expressing or nondepressed caregivers, suggesting that although
showing pleasure very much, 30.4% showing plea- TAP was behaviorally demanding, distressed care-
sure somewhat and only 2.2% showing no pleasure. givers could participate, learn to use activities, and
Only 6.5% of patients refused participation, 2.2% benefit.
appeared agitated and 2.2% appeared upset in one or Why does engagement in activities tailored to cog-
more sessions. Interventionists reported that 84.8% nitive capacity and interests of dementia patients
of caregivers indicated the intervention was very reduce behavioral symptoms? One explanation is
useful, with 15.2% finding it somewhat useful. Also, that activities fill a void, maintain roles, and enable
89.1% of caregivers indicated the intervention had a dementia patients to express themselves positively.
positive effect. Only 10.9% indicated that strategies This promotes continuity in identity and a sense of
had no effect or made matters worse. Interventionists connectedness and belonging, important to life qual-
also reported that 100% of caregivers demonstrated ity throughout the disease.40,41 By introducing sim-
understanding of strategies somewhat or very much. plified activities that capitalized on preserved capa-
Only 2.2% did not use recommended activities. bilities and lifelong social roles (e.g., preparing
simple meals for homemakers), frustration was min-
imized and positive engagement afforded. Self-actu-
alization was illustrated by some patients’ remem-
bering interventionists between treatment sessions
CONCLUSIONS
that occurred weeks apart, creating craft objects for
The results of this controlled pilot study suggest holiday gifts, and seeking to frame placemats made
positive benefits and large symptom reductions as in the assessment.
evidenced by effect sizes for patient and caregiver Another explanation is that the intervention re-
outcomes. For behaviors, the main outcome, treat- duces allostatic load, defined as overload of sensory
ment gains were found overall and for frequently and information processing capacity.42 Recent con-
occurring behaviors (shadowing, repetitive question- ceptualizations of behaviors as reflecting the inter-
ing). Fewer caregivers in intervention reported oc- play between neurologic, psychosocial, and environ-
currences of agitation and argumentation, behaviors mental factors suggest that external conditions may
known to trigger nursing home placement. Addi- overload patients’ abilities, which may have negative
tionally, life quality improvements were found with consequences.17,43 Simplifying task and environmen-
caregivers reporting enhanced ability to derive plea- tal contexts in which activities occur may reduce
sure and engage in activities for dementia patients. physiologic stress responses and agitated-type be-
TAP did not minimize patient depressed mood, al- haviors.
though change was in the expected direction war- Caregivers may benefit from TAP in several ways.
ranting further examination with larger samples. A significant concern and source of distress for families
As to caregivers, TAP significantly reduced objec- is occupying their relatives and supporting person-
tive burden as measured by time spent caregiving; hood.5 TAP offered engaging activities, and caregiv-
however, subjective appraisals of burden were not ers could observe immediate benefits. The assessments
affected, suggesting that to address caregiver upset, also provided an understanding of patient capacity.
236 Am J Geriatr Psychiatry 16:3, March 2008
Gitlin et al.
Finally, caregivers found the tailored activities easy dence that tailoring activities to match residual abil-
and not time consuming to implement. ities, previous roles and interests, improves life qual-
Important clinical implications can be derived ity for dementia patients living at home. TAP offers
from this study. The TAP assessment combined neu- an assessment approach for identifying capabilities
ropsychological and performance-based testing to from which activities can be developed, reduces be-
identify capacities and deficits. Families often under- havioral symptoms, and benefits caregivers. As such,
or overestimate patient abilities and may benefit TAP provides a systematic nonpharmacologic man-
from the assessment itself. One recommendation agement approach for minimizing difficult behaviors
may be for referral to an occupational therapist that warrants further large-scale testing, validation
trained in TAP to augment neuropsychological test- with diverse dyads, and investigation into the un-
ing, to more adequately inform families of patient derlying physiologic mechanisms accounting for
capacities. Because TAP preserves functionality by symptom reductions.
reducing behavioral disturbances, it may be reim-
bursable under Medicare guidelines and thus is a
feasible disease management approach.
Several study limitations warrant caution in inter- APPENDIX: SAMPLE ACTIVITY
preting findings. First, the lack of an attention control PRESCRIPTION—THE TAILORED
group makes it impossible to exclude the possibility
ACTIVITY PROGRAM
that demonstrated benefits are due to the time and
attention bestowed by interventionists. Second, pilot Today’s date: ———————
studies may yield large effect sizes and overestimate
treatment benefits.44 Although our results are prom- Your Husband’s Abilities
ising, further testing of TAP is necessary with larger
• Good hand skills–Able to grasp, release, and
samples and randomized designs controlling for the
throw objects.
attention factor.
Handles/manipulates objects to gather addi-
Another potential limitation is reliance on care-
tional information thru his sense of “touch”
giver self-report of behavioral occurrences, which
• Follows simple 1 step directions with additional
may be affected by caregiver mood and perceived
cueing (“pointing” and short verbal cues work
study demands. Even so, we used two psychometri-
best)
cally sound measures commonly employed in be-
• Good attention and tolerance (up to 30 minutes)
havioral and pharmacologic research and clinical
with activities of interest
contexts that rely on collateral informants. Addition-
• Able to distinguish between size, shape, and
ally, research suggests caregiver depressed mood ac-
feel of objects
counts for only about 33% of variance in behavioral
• Sustains repetitive actions; needs some assis-
ratings.45 Moreover, obtaining objective behavioral
tance to progress to the next step
ratings in homes from independent raters may not be
feasible. Behavioral events occur day or night, mak-
ing objective sampling difficult. Having an indepen- Recommended Activity: Wood Craft
dent rater in the home imposes additional environ-
mental demand characteristics that may have a Activity Goal: Your husband will paint/stain
reactive effect, particularly for easily agitated or wood boxes with familiar paintbrush for 30 minutes,
paranoid patients. Asking caregivers to chart behav- one time per week.
iors can improve accuracy, but may be too burden-
some resulting in noncompliance, missing data, and Simplify the Setting for the Activity
inaccurate recordings. Thus, reliance on proxy or
caregiver report of dementia-related behaviors re- 1. Set up the area to enhance your husband’s orien-
mains the preferred methodology that is widely tation and success in completing the activity.
used. 2. Remove all objects from dining room table except
In summary, this study provides preliminary evi- a protective covering and craft objects.
Am J Geriatr Psychiatry 16:3, March 2008 237
Tailored Activity Program for Persons With Dementia
3. Place one wood box on the table in your hus- 4. You may need to help your husband initiate and
band’s field of vision (within 24 inches) sequence the activity. Use a guiding touch and a
4. Make sure overhead light is on. simple command to redirect if needed.
5. Choose time of day when your husband is at his
Simplify the Activity best—Alert and energized.
1. Allow sufficient time to complete the “task of the
Communicate Effectively
day.” Your husband may only paint or stain wood
box for 10 –15 minutes. That is okay. He may 1. As you do naturally, continue to use encouraging
return to the task after a short break. remarks as he participates in the activity.
2. Provide your husband with one box at a time. 2. Use short, clear and precise instructions.
3. Relax standard of performance (there is no right 3. If your husband looses focus, use a calm voice and
or wrong way). touch his arm to guide him back to the task. Use
praise and encouragement to continue.
Enhance Participation
Strategies for You
1. Draw on your husband’s ability to engage in re-
petitive activities. 1. Try to relax; take a few deep breaths before intro-
2. Draw on your husband’s ability to work well with ducing the activity as we practiced.
his hands and painting history. 2. Remember, there is no right or wrong way for
3. Your husband has great “activity tolerance” and your husband to do the activity.
sticks with a meaningful activity until his is tired. 3. Feel good about yourself—you are doing a great
Monitor level of frustration. job.
References
1. Alzheimer’s Association: Alzheimer’s Association Facts and Figures 2007 10. Schneider LS, Tariot PN, Dagerman KS, et al: Effectiveness of
[Alzheimer’s Association Web site]. 2007. Available at: http://www.alz. atypical antipsychotic drugs in patients with Alzheimer’s disease.
org/national/documents/Report 2007FactsAndFigures.pdf. Accessed N Engl J Med 2006; 35:1525–1538
April 11, 2007 11. Sink KM, Holden KF, Yaffee K: Pharmacological treatment of
2. Lebowitz BD: Behavioral and psychological symptoms of demen- neuropsychiatric symptoms of Dementia: a review of evidence.
tia (BPSD): a clinical and research update. Int Psychogeriatr 2000; J Am Med Assoc 2005; 293:596 – 608
12(S1): 19 –21 12. Gitlin LN, Corcoran MA, Winter L, et al: A randomized, controlled
3. Lyketsos CG, Sheppard JME, Steinberg M, et al: Neuropsychiatric trial of a home environmental intervention: effect on efficacy and
disturbance in Alzheimer’s disease clusters into three groups: the upset in caregivers and on daily function of persons with demen-
Cache County study. Int J Geriatr Psychiatry 2001; 16:1043–1053 tia. Gerontologist 2001; 41:15–30
4. Landes AM, Sperry SD, Strauss ME: Prevalence of apathy, dyspho- 13. Gitlin LN, Winter L, Corcoran MA, et al: Effects of the home
ria, and depression in relation to dementia severity in Alzheimer’s environmental skill-building program on the caregiver– care re-
disease J Neuropsychiatry Clin Neurosci 2005; 17:342–349 cipient dyad: 6-month outcomes from the Philadelphia REACH
5. Ballard C, Lowery K, Powell I, et al: Impact of behavioral and initiative. Gerontologist 2003; 43:532–546
psychological symptoms of dementia on caregivers. Int Psychoge- 14. Belle SH, Burgio L, Burns R, et al: Enhancing the quality of life of
riatr 2000; 12:93–105 dementia caregivers from different ethnic or racial groups: a
6. Fauth EB, Zarit SH, Femia EE, et al: Behavioral and psychological randomized, controlled trial. Ann Intern Med 2006; 145:727–738
symptoms of dementia and caregivers’ stress appraisals: intra- 15. Gallagher-Thompson D, Gray JI, Tang PCY, et al: Impact of
individual stability and change over short-term observations. Ag- In-home behavioral management versus telephone support to
ing Ment Health 2006; 10:563–573 reduce depressive symptoms and perceived stress in Chinese
7. Gilley DW, Bienias JL, Wilson RS, et al: Influence of behavioral caregivers: results of a pilot study. Am J Geriatr Psychiatry 2007;
symptoms on rates on institutionalization for person’s with Alz- 15:425– 434
heimer’s disease. Psychol Med 2004; 34:1129 –1135 16. Mittelman MS, Roth DL, Haley, et al: Effects of a caregiver inter-
8. Magai C, Hartung R, Cohen CI: Caregiver distress and behavioral vention on negative caregiver appraisals of behavior problems in
symptoms, in Behavioral complications in Alzheimer’s disease. patients with Alzheimer’s disease: results of a randomized trial.
Edited by Lawlor BA. Washington, DC, American Psychiatric J Gerontol B Psychol Sci 2004; 59B:P27–P34
Press, 1995; pp 223–243 17. Lyketsos CG, Colenda CC, Beck C, et al: Position statement of the
9. Schneider LS, Dagerman KS, Insel P: Risk of death with atypical American Association for Geriatric Psychiatry regarding princi-
antipsychotic drug treatment for Dementia. J Am Med Assoc ples of care for patients with dementia resulting from Alzheimer
2005; 294:1934 –1943 disease. Am J Geriatr Psychiatry 2006; 14:561–573
238 Am J Geriatr Psychiatry 16:3, March 2008
Gitlin et al.
18. Covinsky KE, Johnson CB: Envisioning better approaches for 32. Alexopoulos GS, Abrams RC, Young RC, et al: Cornell Scale for
dementia care. Ann Intern Med 2006; 145:780 –781 depression in dementia. Biol Psychiatry 1998; 23:271–284
19. Marshall MJ, Hutchinson SA: A critique of research on the use of 33. Logsdon RG, Gibbons Le, McCurry SM, et al: Assessing quality of
activities with person with Alzheimer’s disease: a systematic life in older adults with cognitive impairment. Psychosom Med
literature review. J Adv Nurs 2001; 35:488 – 496 2002; 64:510 –519
20. Cohen-Mansfield J: Nonpharmacologic interventions for inappro- 34. Lawton MP, Kleban MH, Moss M, et al: Measuring caregiving
priate behaviors in dementia: a review, summary, and critique. appraisal. J Gerontol 1989; 3:61–71
Am J Geriatr Psychiatry 2001; 9:361–381 35. Roth DL, Burgio LD, Gitlin LN, et al: Psychometric analysis of the
21. Garland K, Beer E, Eppingstall B, et al: A comparison of two Revised Memory and Behavior Problems Checklist: factor struc-
treatments of agitated behavior in nursing home residents with ture of occurrence and reaction ratings. Psychol Aging 2003;
dementia: simulated family presence and preferred music. Am J 18:906 –915
Geriatr Psychiatry 2007; 15:514 –521 36. Bedard M, Molloy DW, Squire L, et al: The Zarit Burden Interview:
22. Folstein MF, Folstein SE, McHugh PR: “Mini-mental state.” A a new short version and screening version. Gerontologist 2001;
practical method for grading the cognitive state of patients for 41:652– 657
the clinician. J Psychiatr Res 1975; 12:189 –198 37. Mahoney DF, Jones RN, Coon D, et al: The Caregiver Vigilance
23. Hall GR, Buckwalter KC: Progressively lowered stress threshold: Scale: application and validation in the Resources for Enhancing
a conceptual model for care of adults with Alzheimer’s disease. Alzheimer’s Caregiver (REACH) project. Am J Alzheimers Dis
Arch Psychiatr Nurs 1987; 1:399 – 406 Other Demen 2003; 18:39 – 48
24. Lawton MP, Nahemow LE: Ecology and the aging process, in The 38. Radloff LS: The CES-D scale: a self-report depression scale for
Psychology of Adult Development and Aging. Edited by Eisdorfer research in the general population. Appl Psychol Meas 1977;
C, Lawton MP. Washington, DC, American Psychological Associ- 1:385– 401
ation, 1973, pp 619 – 674 39. Gitlin LN, Winter L, Dennis M, et al: Strategies used by families to
25. Teri L, Logsdon RG: Identifying pleasant activities for Alzheimer’s simplify tasks for individuals with Alzheimer’s disease and related
disease patients: the pleasant events schedule-AD. Gerontologist disorders: psychometric analysis of the task management strategy
1991; 31:124 –127 index (TMSI). Gerontologist 2002; 42:61– 69
26. Jurica PJ, Leittenn CL, Mattis S: Dementia Rating Scale-2: Pro- 40. Cohen-Mansfield J, Parpura-Gill A, Golander H, et al: Utilization of
fessional Manual. Lutz, FL, Psychological Assessment Re- Self-Identity Roles for Designating Interventions for Persons with
sources, 2001 Dementia. J Gerontol B Psychol Sci Soc Sci 2006; 4:202–212
27. Allen CK, Blue T: Cognitive disabilities model: how to make 41. Phinney A, Chaudhury H, O’Connor DL: Doing as much as I can
clinical judgments, in Cognition Occupation in Rehabilitation: do: the meaning of activity for people with dementia. Aging Ment
cognitive models for intervention and occupational therapy. Ed- Health 2007; 11:384 –393
ited by Katz N. Bethesda, Md. The American Occupational Ther- 42. Gallagher-Thompson D, Shurgot GR, Rider K, et al: Ethnicity,
apy Association, 1998, pp 225–279 stress, and cortisol function in Hispanic and non-Hispanic white
28. Blue T, Allen CK: Allen Diagnostic Module Sensory Motor Stimu- women: a preliminary study of family dementia caregivers and
lation Kit II. Colchester, CT, S&S Worldwide, 1993 noncaregivers. Am J Geriatr Psychiatry 2006; 14:334 –342
29. Earhart CA, Pollard D, Allen CK, et al: Large Allen Cognitive Level 43. Richards KC, Beck CK: Progressively lowered stress threshold
Screen (LACLS) 2000 Test Manual. Colchester, CT, S&S World- model: understanding behavioral symptoms of dementia. J Am
wide, 2003 Geriatr Soc 2004; 52:1774 –1775
30. Logsdon RG, Teri L, Weiner MF, et al: Assessment of agitation in 44. Kraemer HC, Mintz J, Noda A, et al: Caution regarding the use of
Alzheimer’s disease: the agitated behavior in dementia scale. J Am pilot studies to guide power calculations for study proposals.
Geriatr Soc 1999; 47:1354 –1358 Arch Gen Psychiatry 2006; 63:484 – 489
31. Teri L, Truax P, Logsdon R, et al: Assessment of behavioral 45. Rosenberg PB, Mielke MM, Lyketsos CG: Caregiver assessment of
problems in dementia: the Revised Memory and Behavior Prob- patients’ depression in Alzheimer disease: longitudinal analysis in a
lems Checklist (RMBPC). Psychol Aging 1992; 7:622– 631 drug treatment study. Am J Geriatr Psychiatry 2005; 13:822– 826
Am J Geriatr Psychiatry 16:3, March 2008 239
View publication stats
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5813)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Answer 1-CHCHCSOO1 Heavendee (Sekhon D4255Document3 pagesAnswer 1-CHCHCSOO1 Heavendee (Sekhon D4255shweta0% (1)
- QMHC Annualreport 2016-17 WebDocument108 pagesQMHC Annualreport 2016-17 WebpaulartistdingleNo ratings yet
- Dementia GuidelineDocument2 pagesDementia Guideline-Timothy Osho-No ratings yet
- Stem Consent FormDocument3 pagesStem Consent Formapi-351900524No ratings yet
- Preventing and Managing COVID-19 Across Long-Term Care ServicesDocument8 pagesPreventing and Managing COVID-19 Across Long-Term Care ServicesMark Anthony MadridanoNo ratings yet
- Outlinethe Role of HCA in The Day To Day Provision of Care or The Older PersonDocument8 pagesOutlinethe Role of HCA in The Day To Day Provision of Care or The Older Person1chirciu1976floNo ratings yet
- National Clinical Guidelines For Stroke Fourth Edition 2012Document232 pagesNational Clinical Guidelines For Stroke Fourth Edition 2012h@d1putr@No ratings yet
- TF - CBT Brochure Final 12 16Document2 pagesTF - CBT Brochure Final 12 16Hashem Al AttasNo ratings yet
- Family Centred Hiv AidsDocument21 pagesFamily Centred Hiv AidsAyu KrismaNo ratings yet
- Case Study of Teenage PregnancyDocument16 pagesCase Study of Teenage PregnancyJanine LimjucoNo ratings yet
- Modified Interview For Deterioration in Daily Living Activities in Dementia (IDDD)Document5 pagesModified Interview For Deterioration in Daily Living Activities in Dementia (IDDD)CristiNo ratings yet
- OBRA and State Line ServicesDocument4 pagesOBRA and State Line ServicesIndiana Family to FamilyNo ratings yet
- Guidelines Protocols and FAQs As Per Covid Care CommitteeDocument28 pagesGuidelines Protocols and FAQs As Per Covid Care CommitteeMadhusmita NayakNo ratings yet
- WEEK 2: 12A, 12B, 12G Ôn Tập Khảo Sát Pronunciation ClosestDocument6 pagesWEEK 2: 12A, 12B, 12G Ôn Tập Khảo Sát Pronunciation ClosestHàNhậtNguyễnNo ratings yet
- DAVmagazineDocument40 pagesDAVmagazineMichael BonnieNo ratings yet
- Dementia Competency FrameworkDocument22 pagesDementia Competency FrameworkrowanpurdyNo ratings yet
- Full Ebook of Implementation Science The Key Concepts 1St Edition Frances Rapport Robyn Clay Williams Jeffrey Braithwaite Online PDF All ChapterDocument70 pagesFull Ebook of Implementation Science The Key Concepts 1St Edition Frances Rapport Robyn Clay Williams Jeffrey Braithwaite Online PDF All Chapterdanielklein170297100% (4)
- OT in Productive Aging Top 10 ThingsDocument33 pagesOT in Productive Aging Top 10 ThingsRobertAlexandraSculschiNo ratings yet
- Psychosocial Support: APRIL 15, 2016Document2 pagesPsychosocial Support: APRIL 15, 2016Batanai Djbornagain KaysNo ratings yet
- Case ScenarioDocument10 pagesCase Scenariodavlin1724No ratings yet
- YCDSB Procedure Policy 212 Concussions FINAL Revised Sept 2019Document17 pagesYCDSB Procedure Policy 212 Concussions FINAL Revised Sept 2019gsen75No ratings yet
- Acceptance of Tele-Rehabilitation by Stroke Patients: Perceived Barriers and FacilitatorsDocument8 pagesAcceptance of Tele-Rehabilitation by Stroke Patients: Perceived Barriers and Facilitatorsana irianiNo ratings yet
- Evaluation of Feeding, Eating, and Swallowing For Children With Cerebral PalsyDocument9 pagesEvaluation of Feeding, Eating, and Swallowing For Children With Cerebral Palsyanner.socialsNo ratings yet
- Oet 2 PDFDocument96 pagesOet 2 PDFSharika SayedNo ratings yet
- Research Agenda On Ageing For The 21st CenturyDocument8 pagesResearch Agenda On Ageing For The 21st CenturynbotevNo ratings yet
- The Best Way To Teach Self Care SkillsDocument26 pagesThe Best Way To Teach Self Care SkillsKarla TolentinoNo ratings yet
- WV Child Protection Assessment ReportDocument75 pagesWV Child Protection Assessment ReportCecilia2002No ratings yet
- An Introductory Guide To Schema-Focused Therapy - Adapted For Use With The YSQ-RDocument19 pagesAn Introductory Guide To Schema-Focused Therapy - Adapted For Use With The YSQ-RCeline Tan100% (1)
- Learn The Child Case StudiesDocument18 pagesLearn The Child Case StudiesNoo BoddieNo ratings yet
- Guideline For Alzheimer'S Disease Management: Final Report 2008Document122 pagesGuideline For Alzheimer'S Disease Management: Final Report 2008Chaddia MoresNo ratings yet