You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5814)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- 2020-21 Valley Winter Sports ProfileDocument24 pages2020-21 Valley Winter Sports ProfileAaron YoungNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- 2019 Fall Expo Contact List PDFDocument10 pages2019 Fall Expo Contact List PDFSoji AdimulaNo ratings yet
- 3 Takaful Emarat & Orient - Rn2 March2022.Document186 pages3 Takaful Emarat & Orient - Rn2 March2022.nafilkhanNo ratings yet
- Technological Advances in Nontraditional Orthodontics PDFDocument14 pagesTechnological Advances in Nontraditional Orthodontics PDFcatherineNo ratings yet
- Skeletal and Skin TractionDocument38 pagesSkeletal and Skin TractionCORROS JASMIN MARIE100% (1)
- Nonsurgical Rhinoplasty With Polydioxanone Threads and FillersDocument8 pagesNonsurgical Rhinoplasty With Polydioxanone Threads and FillersRaphaela TravassosNo ratings yet
- University Physics Volume 2 Derived Copy For Ysc1213 1.75Document441 pagesUniversity Physics Volume 2 Derived Copy For Ysc1213 1.75Soji AdimulaNo ratings yet
- Excessive Gingival Display Etiology Diagnosis and Treatment Modalities NIR SILBERBERGDocument10 pagesExcessive Gingival Display Etiology Diagnosis and Treatment Modalities NIR SILBERBERGValentina100% (4)
- Stanford Clinical Anesthesia TextbookDocument103 pagesStanford Clinical Anesthesia TextbookRishi Sharma100% (2)
- Perioperative CareDocument39 pagesPerioperative CareSolomon100% (1)
- Gauss Law ReviewDocument61 pagesGauss Law ReviewSoji AdimulaNo ratings yet
- Son of South Korean Immigrants, Bucks County's Andrew Heo Carries Family's Olympic Dream To BeijingDocument8 pagesSon of South Korean Immigrants, Bucks County's Andrew Heo Carries Family's Olympic Dream To BeijingSoji AdimulaNo ratings yet
- Chapter 11Document12 pagesChapter 11Soji AdimulaNo ratings yet
- Tree Care Industry MagazineDocument44 pagesTree Care Industry MagazineSoji AdimulaNo ratings yet
- DiagramsDocument62 pagesDiagramsSoji AdimulaNo ratings yet
- Sun Hasn't Set On Sunrise Packaging - Minneapolis - St. Paul Business JournalDocument4 pagesSun Hasn't Set On Sunrise Packaging - Minneapolis - St. Paul Business JournalSoji AdimulaNo ratings yet
- Molecular Orbitals and Curved ArrowsDocument51 pagesMolecular Orbitals and Curved ArrowsSoji AdimulaNo ratings yet
- Bio-Med 350: Normal Heart Function and Congestive Heart FailureDocument59 pagesBio-Med 350: Normal Heart Function and Congestive Heart FailureSoji AdimulaNo ratings yet
- Chem 14CL - Lecture 1 - Amino - AcidDocument17 pagesChem 14CL - Lecture 1 - Amino - AcidSoji AdimulaNo ratings yet
- RC Circuits: Instructor: Kazumi TolichDocument11 pagesRC Circuits: Instructor: Kazumi TolichSoji AdimulaNo ratings yet
- Faculty Version With Model Answers: Body FluidsDocument10 pagesFaculty Version With Model Answers: Body FluidsSoji AdimulaNo ratings yet
- What Is An Argument?: ConclusionDocument25 pagesWhat Is An Argument?: ConclusionSoji AdimulaNo ratings yet
- Periodic Properties of The Elements: Theodore L. Brown H. Eugene Lemay, Jr. and Bruce E. BurstenDocument82 pagesPeriodic Properties of The Elements: Theodore L. Brown H. Eugene Lemay, Jr. and Bruce E. BurstenSoji AdimulaNo ratings yet
- Inflammation and Repair: Definition of Inflammation Acute Inflammation Vascular Events in InflammationDocument35 pagesInflammation and Repair: Definition of Inflammation Acute Inflammation Vascular Events in InflammationSoji AdimulaNo ratings yet
- Happy Labor Day: Tuesday, September 8, 2020Document1 pageHappy Labor Day: Tuesday, September 8, 2020Soji AdimulaNo ratings yet
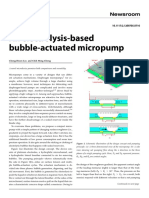
- An Electrolysis-Based Bubble-Actuated Micropump: Cheng-Hsien Liu and Chih Ming ChengDocument3 pagesAn Electrolysis-Based Bubble-Actuated Micropump: Cheng-Hsien Liu and Chih Ming ChengSoji AdimulaNo ratings yet
- Non-Operating Room Anesthesia (NORA) : A Beginner's GuideDocument26 pagesNon-Operating Room Anesthesia (NORA) : A Beginner's GuidepaulaNo ratings yet
- Jump Gait in Spastic Diplegia: An Expert Panel Case ReviewDocument6 pagesJump Gait in Spastic Diplegia: An Expert Panel Case ReviewHiram CastroNo ratings yet
- GraduateOutcomesSET ProgramUrologyDocument2 pagesGraduateOutcomesSET ProgramUrologyKirk KNo ratings yet
- 1.04 Large Intestine, Colon, and RectumDocument15 pages1.04 Large Intestine, Colon, and RectumZazaNo ratings yet
- Modul 6 BHS Ing Kep 1 Medical EquipmentsDocument6 pagesModul 6 BHS Ing Kep 1 Medical EquipmentsZikri RizaldiNo ratings yet
- Sri Wulandari N., M.Kep., Ns - Sp.Kep - AnDocument11 pagesSri Wulandari N., M.Kep., Ns - Sp.Kep - Anefi afriantiNo ratings yet
- 5 IV InsertionDocument16 pages5 IV InsertionEfreignz Mangay-at KinomesNo ratings yet
- Maggot Manual 2021Document16 pagesMaggot Manual 2021JCNo ratings yet
- Bbraun - Urimed-Bag-BrochureDocument6 pagesBbraun - Urimed-Bag-BrochureCampaign MediaNo ratings yet
- Hartofilakidis Classification Developmental Dysplasia of The HipDocument3 pagesHartofilakidis Classification Developmental Dysplasia of The HiphaminatrafNo ratings yet
- Tessier CleftDocument37 pagesTessier CleftJeel MohtaNo ratings yet
- MRN000410 BnCWy5eDocument11 pagesMRN000410 BnCWy5eAn JNo ratings yet
- Dr. Ahlam Al-Kharabsheh: Assistant Professor, OBS & GYN Department Mu'tah UniversityDocument36 pagesDr. Ahlam Al-Kharabsheh: Assistant Professor, OBS & GYN Department Mu'tah Universityraed faisalNo ratings yet
- Advocate Aurora Antitrust LawsuitDocument76 pagesAdvocate Aurora Antitrust LawsuitAnonymous 6f8RIS6No ratings yet
- Morbidity & Mortality (July, 2019)Document28 pagesMorbidity & Mortality (July, 2019)Wai GyiNo ratings yet
- Branstool Zachary Mental Health Case StudyDocument9 pagesBranstool Zachary Mental Health Case StudyZac BranstoolNo ratings yet
- OBM752 HM Unit-IV NotesDocument34 pagesOBM752 HM Unit-IV NotesRajanNo ratings yet
- 001 Organizational Plan For Patient CareDocument8 pages001 Organizational Plan For Patient CareMohamed NaeemNo ratings yet
- Medico Legal Report - ThamaeDocument13 pagesMedico Legal Report - ThamaencetaniNo ratings yet
- The Anatomy of Dorsal Ramus Nerves and Its Implica PDFDocument10 pagesThe Anatomy of Dorsal Ramus Nerves and Its Implica PDFPoramin BoonyawetchewinNo ratings yet
- SOP Irigasi TelingaDocument10 pagesSOP Irigasi Telingasasikirana sasikirNo ratings yet
- Reboa 02Document5 pagesReboa 02Maria AngelescuNo ratings yet