You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5813)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Ampere Generator IFU ENGDocument66 pagesAmpere Generator IFU ENGJonathan HernándezNo ratings yet
- AHA-PALS 2010: Pediatric Chain of SurvivalDocument10 pagesAHA-PALS 2010: Pediatric Chain of SurvivalIsabel CastilloNo ratings yet
- Basic Life Support: Participant's ManualDocument122 pagesBasic Life Support: Participant's ManualMarc Andreo Malala0% (1)
- Health and Wellness 2 Roll No 5Document16 pagesHealth and Wellness 2 Roll No 5Ansa MalikNo ratings yet
- CT of The Heart: U. Joseph Schoepf EditorDocument903 pagesCT of The Heart: U. Joseph Schoepf Editorruth_labella3653No ratings yet
- Supraventricular Tachycardia NotesDocument59 pagesSupraventricular Tachycardia NotesShadi TabbarahNo ratings yet
- PEDIA - Cardio (Esguerra) PDFDocument9 pagesPEDIA - Cardio (Esguerra) PDFMedisina101No ratings yet
- Nayor Et Al-2017-European Journal of Heart FailureDocument9 pagesNayor Et Al-2017-European Journal of Heart FailurelacatisNo ratings yet
- Assisting Arterial Blood Gas: Lesson PlanDocument2 pagesAssisting Arterial Blood Gas: Lesson PlanSwapnil MahapureNo ratings yet
- Pressure Injectors For Radiologists A Review and WDocument10 pagesPressure Injectors For Radiologists A Review and WL. K. DasNo ratings yet
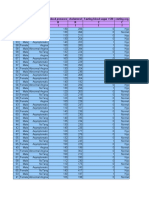
- Age Sex Chest Pain Type Blood Pressure Cholesterol Fasting Blood Sugar 120 Resting Ecg R C C R R C C I I I I I I IDocument14 pagesAge Sex Chest Pain Type Blood Pressure Cholesterol Fasting Blood Sugar 120 Resting Ecg R C C R R C C I I I I I I Isantu4_1111No ratings yet
- Enoxaparin - Prescribing, Administration and MonitoringDocument6 pagesEnoxaparin - Prescribing, Administration and MonitoringFaheem AlsabriaNo ratings yet
- Long-Term Outcome in Congenitally Corrected Transposition of The Great ArteriesDocument7 pagesLong-Term Outcome in Congenitally Corrected Transposition of The Great Arteriespaul00040No ratings yet
- Pharmacology Assignment No.02: Submitted By: Submitted To: Nandraj Ma'am Areeba Shafiq Roll No. 1817007Document23 pagesPharmacology Assignment No.02: Submitted By: Submitted To: Nandraj Ma'am Areeba Shafiq Roll No. 1817007Nandraj123100% (1)
- 2014 Article 85Document7 pages2014 Article 85taufikolingNo ratings yet
- Praktikum EBM Hipertensi Kel 2Document15 pagesPraktikum EBM Hipertensi Kel 2Intan PermatasariNo ratings yet
- Radhakrishnan2013 PREVALENCE OF HYPERTENSION AND DIABETES IN GERIATRIC PATIENTSDocument9 pagesRadhakrishnan2013 PREVALENCE OF HYPERTENSION AND DIABETES IN GERIATRIC PATIENTSConfidence UzomaNo ratings yet
- FRE 20101201 Dec 2010Document250 pagesFRE 20101201 Dec 2010Esteban Cabrera100% (1)
- Kewenangan Klinis SP - JPDocument3 pagesKewenangan Klinis SP - JPVania Lystia TantraNo ratings yet
- ACLSDocument46 pagesACLSYeoh Hong Shin100% (3)
- Assessing Heart and Neck VesselsDocument7 pagesAssessing Heart and Neck VesselsJae TyNo ratings yet
- Inpatient Quality Indicators™ V2020 Benchmark Data TablesDocument19 pagesInpatient Quality Indicators™ V2020 Benchmark Data TablesHanayuki VizureiNo ratings yet
- Recurrent Stroke in Minor Ischemic Stroke or Transient IschemicDocument12 pagesRecurrent Stroke in Minor Ischemic Stroke or Transient IschemicdickyNo ratings yet
- Factores para FNRDocument10 pagesFactores para FNRPOMYNo ratings yet
- UntitledDocument37 pagesUntitledclaudiaNo ratings yet
- Scandinavian Med Sci Sports - 2023 - Moore - Exploring The Direct and Indirect Effects of Cardiovascular Disease RiskDocument7 pagesScandinavian Med Sci Sports - 2023 - Moore - Exploring The Direct and Indirect Effects of Cardiovascular Disease RiskGabriel CostaNo ratings yet
- Discharge Planning PaperDocument5 pagesDischarge Planning Paperapi-398485408No ratings yet
- Study Guide 1 Case Studies 1 and 2 Gutierrez, W.Document3 pagesStudy Guide 1 Case Studies 1 and 2 Gutierrez, W.Winell Gutierrez100% (1)
- Concept Map For Anterior Myocardial Infarction: I. Introduction and ObjectivesDocument6 pagesConcept Map For Anterior Myocardial Infarction: I. Introduction and ObjectivesLouise GudmalinNo ratings yet
- HFAI 2021 Programme FinalDocument40 pagesHFAI 2021 Programme FinaljayjayshrigokuleshNo ratings yet