Professional Documents
Culture Documents
Chromosomally Integrated Human Herpesvirus 6 in Heart Failure: Prevalence and Treatment
Uploaded by
anandaacpOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Chromosomally Integrated Human Herpesvirus 6 in Heart Failure: Prevalence and Treatment
Uploaded by
anandaacpCopyright:
Available Formats
European Journal of Heart Failure (2015) 17, 9–19
doi:10.1002/ejhf.194
Chromosomally integrated human herpesvirus
6 in heart failure: prevalence and treatment
Uwe Kühl1*†, Dirk Lassner2,†, Nina Wallaschek3, Ulrich M. Gross2, Gerhard R.F.
Krueger4, Bettina Seeberg1, Benedikt B. Kaufer3, Felicitas Escher1, Wolfgang
Poller1, and Heinz-Peter Schultheiss1
1 Department of Cardiology & Pneumology, Campus Benjamin Franklin, Charité-Universitätsmedizin Berlin, Berlin, Germany; 2 Institut Kardiale Diagnostik und Therapie (IKDT),
Berlin, Germany; 3 Institut für Virologie, Freie Universität Berlin, Berlin, Germany; and 4 Department of Pathology& Laboratory Medicine, The University of Texas-Houston
Medical School, Houston, TX, USA
Received 27 May 2014; revised 25 August 2014; accepted 28 August 2014 ; online publish-ahead-of-print 11 November 2014
Aims Human herpesvirus 6 (HHV-6) A and B are two betaherpesviruses that are associated with many conditions including
roseola, drug-induced hypersensitivity syndrome, limbic encephalitis, and myocarditis. HHV-6 is integrated in the
germline [chromosomically integrated HHV-6 (ciHHV-6)] in ∼0.8% of the human population. To date, the prevalence,
species distribution, and treatment responses of ciHHV-6 are unknown for cardiac patients.
.....................................................................................................................................................................
Methods We determined the prevalence of HHV-6 and ciHHV-6 genotypes in 1656 endomyocardial biopsies of patients with
and results persisting unexplained symptoms of heart failure. Infection of cardiac tissue was identified by nested PCR, electron
microscopy, and immunohistochemistry. Virus load and mRNA levels were followed in ciHHV-6 patients treated
with ganciclovir. HHV-6 was detected in 273 of 1656 cardiac tissues (16.5%; HHV-6B, 98.2%, HHV-6A, 1.8%) by
PCR. Nineteen of the 1656 patients (1.1%) presented with persistently high HHV-6 copy numbers indicative of
ciHHV-6. Sequencing confirmed ciHHV-6A in seven patients (36.8%) which was considerably higher than detected in
non-ciHHV-6 patients. Inheritance was demonstrated in three selected families, confirming ciHHV-6 chromosomal
integration by PCR and fluorescence in situ hybridization. HHV-6 reactivation and chromosomal integration were
confirmed in peripheral blood mononuclear cells and heart tissue. Virus particles were identified in degenerating
myocytes and interstitial cells. Antiviral treatment abolished viral mRNA and ameliorated cardiac symptoms.
.....................................................................................................................................................................
Conclusion Virus replication in cardiac tissue of ciHHV-6 heart failure patients suggests that ciHHV-6 reactivation causes
persistence of unexplained heart failure symptoms. We demonstrated that antiviral treatment, effective in decreasing
viral transcripts and clinical complaints of cardiomyopathies, is a new therapeutic option for ciHHV-6-associated
..........................................................................................................
diseases.
Keywords Chromosomally integrated human herpesvirus 6 • Myocarditis • Cardiomyopathy • Treatment
Introduction HHV-6B is commonly acquired during the first 2 years of life,
.......................
whereas HHV-6A is acquired later in childhood with unknown
Human herpesvirus 6 (HHV-6) has recently been classified as prevalence.1
two distinct species, HHV-6A and HHV-6B, with significant Human herpesvirus-6A and HHV-6B are lymphotropic viruses
differences in their biological, immunological, and molecular that also infect a broad number of cell types including the vascular
properties. Both betaherpesviruses are closely related to the endothelium.2,3 HHV-6B is the causative agent of exanthema
human cytomegalovirus, and establish a lifelong latency upon subitum (sixth disease), causes one-third of febrile status epilep-
primary infection, with a seroprevalence of >90% in adults. ticus, is an important cause of limbic encephalitis in transplant
*Corresponding author. Department of Cardiology and Pneumology, Campus Benjamin Franklin, Charité-University Medicine Berlin, Hindenburgdamm 30, D-12200 Berlin,
Germany. Tel: +49 30 8445 4219, Fax +49 30 8445 4219, Email: uwe.kuehl@charite.de
† These two authors contributed equally to this work.
© 2014 The Authors
European Journal of Heart Failure © 2014 European Society of Cardiology
10 U. Kühl et al.
patients, and may play a role in a subset of mesial temporal lobe 2010. All patients presented with unexplained clinical symptoms of
..................................................................................................................................................................................
epilepsy. HHV-6A has been associated with Hashimoto’s thyroidi- heart failure including fatigue, weakness, chest pain at rest or on
tis and multiple sclerosis. Both viruses reactivate in drug-induced exertion, dyspnoea on exertion, palpitations and reduced physical
hypersensitivity disorder (DIHS), hepatitis, pneumonitis, and capacity, and clinically suspected myocarditis (n = 1192) or idiopathic
DCM (n = 464). Patients with other severe concomitant diseases were
lymphadenitis. HHV-6 reactivation results in subacute clinical
excluded from this analysis. All patients gave written informed con-
presentations, especially in acquired or drug-induced immune
sent for biopsy-based and genetic analyses to determine the underlying
deficiencies (e.g. transplant recipients) or in patients with autoim- cause of the disease. The protocol was approved by the local med-
mune disorders.1,4 It has been suggested that HHV-6 enhances ical ethics committee from the Charitè University Hospital (Berlin),
the pathogenicity of other viruses and is not always the causative Germany. They underwent EMB and right heart catheterization in
agent.5 It can infect various organs, even though infectious virus is a standardized manner as previously described.8 The clinical pre-
difficult to isolate from the peripheral blood and the virus genome sentation and baseline characteristics of patients with HHV-6 and
remains below the detection limit in many patients.6 Similarly, ciHHV-6 infection are given in the Supplementary material online,
HHV-6 can persist in brain tissue, myocarditis, and hepatitis, with Table S1.
little or no trace in the peripheral blood, discoverable only by
biopsy or at autopsy.6,7 Recently, HHV-6 has been detected in the
myocardium of patients with myocarditis and clinically suspected Molecular biological analysis
dilated cardiomyopathy (DCM) by PCR. Short-term follow-ups and sequencing of viral genomes
revealed an association with the clinical course of the disease.8 Polymerase chain reaction (PCR)/reverse transcription–PCR
There has been speculation about regional differences in rates of (RT–PCR) were performed to detect a panel of viruses as pub-
HHV-6 and parvovirus B19 (PVB19) infection in Germany and lished previously.8 HHV-6 genomes were amplified by nested PCR
other countries. However, there is no evidence to support regional (nPCR) using the primer pairs indicated in the Supplement material
differences. These two viruses were never tested in the earlier online, Table S2. Virus isolates were classified into HHV-6A and
biopsy studies done in the USA, and the practice of routine biop- HHV-6B by direct sequencing as described previously.17 Further
sies in myocarditis was ended in the mid 1980s, so these newer details on PCR analyses are given in the Supplementary material
tests were only done in Europe where biopsies are still performed online.
routinely.
Intriguingly, HHV-6 is able to integrate its genomes into telom-
eres of human chromosomes, which allows transmission of HHV-6 Histology and iimmunohistology
via the germline. Chromosomally integrated HHV-6 (ciHHV-6) is Histological specimens were examined according to the Dallas
present in ∼0.2% of the Japanese and 0.85% of the UK and US Classification.18 Immunohistochemistry (IHC) was performed as
populations, respectively, and increases up to 3.3% in hospitalized published previously.19,20 IHC staining of HHV-6 proteins was carried
patients.9,10 HHV-6A represents one-third of ciHHV-6 cases com- out using HHV-6-specific monoclonal antibodies specific for the
pared with only 1–3% of reactivation cases in transplant reacti- virion protein p101 (HHV-6B) and glycoprotein 60/110 (HHV-6A/B)
(Chemicon).2,21
vations or HHV-6-positive patients.9,11 – 14 The effects of ciHHV-6
on the health and development of the patients remain unknown.
Recently it was determined that the integrated virus can activate
in severely immunocompromised patients as well as in pregnant
Electron microscopy
women with ciHHV6.15,16 Since ciHHV-6 integration affects every To determine the topical distribution of HHV-6 in cardiac tis-
nucleated cell, and mRNA is detectable in the peripheral blood sues prior to treatment, formalin-fixed tissues of three untreated
of our ciHHV-6 patients, we investigated the prevalence, germline ciHHV-6 patients were analysed by electron microscopy as described
previously.2 Briefly, tissues were deparafinized and refixed for 90 min
transmission, and reactivation in ciHHV-6 patients with persisting
in Millonig’s buffer containing 3% glutaraldehyde and subsequent
unexplained symptoms of heart failure. Finally we demonstrated
post-fixation for 1 h in 2% osmium tetroxide. After staining with uranyl
that antiviral therapy can diminish HHV-6 replication as well as acetate, dehydration, and propylene oxide treatment, samples were
cardiac symptoms of these patients. We did not study HHV-6 reac- embedded in epoxy resins. 60–100 nm sections were stained with
tivation in the blood of non-ciHHV-6 patients with HHV-6-positive uranyl acetate and lead citrate. All sections were analysed using a JEOL
biopsy tissues because during the persistent phase of this highly 1200EX microscope.
cell-associated virus, HHV-6 DNA is not found in the peripheral
blood in sufficient quantities.
Fluorescence in situ hybridization
To visualize the HHV-6 genome in peripheral blood mononuclear cells
Methods (PBMCs), we performed fluorescence in situ hybridization (FISH) anal-
ysis as described previously.22 Samples were stained with digoxigenin
Patients (DIG)-labelled probes for HHV-6A or 6B and fluorescein isothio-
We prospectively studied 1656 consecutive patients who, after angio- cyanate (FITC)-conjugated anti-DIG antibodies (Sigma). Uninfected and
graphic exclusion of coronary artery disease, underwent a first infected JJhan cells served as controls. FISH preparations were analysed
endomyocardial biopsy (EMB) at our institution between 2003 and using an AxioImager M1 and Axiovision software (Zeiss).
© 2014 The Authors
European Journal of Heart Failure © 2014 European Society of Cardiology
Prevalence and reactivation of ciHHV-6 11
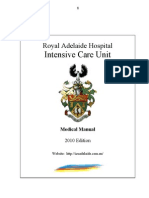
Figure 1 Analysis of family members of treated index patients for chromosomally integrated human herpesvirus 6 (ciHHV-6). Pedigrees of
three ciHHV-6 index patients with ciHHV-6B (P1 and P3) and ciHHV-6A (P2). The presence of ciHHV-6 is indicated by black circles and boxes
for females/males, respectively. The five symptomatic family members are indicated by dotted cycles.
Antiviral treatment and follow-up of 273 (28.2%) patients. Co-infections of HHV-6 with enterovirus
.................................................................................................................
(EV; n = 11), adenovirus (ADV; n = 3), Epstein–Barr virus (EBV;
Six highly symptomatic ciHHV-6 heart failure patients positive for
HHV-6 transcripts suggesting virus reactivation received ganciclovir in
n = 4), or PVB19 (n = 178) (65.2%) were detected in the remain-
addition to heart failure medication. After a 10-day course with 5 mg ing 196 EMBs. Next, we determined the HHV-6 species and
of ganciclovir administered i.v. every 12 h, medication was changed to virus load of 221 (81.0%) patients. HHV-6A was detected in 11
900 mg of valganciclovir p.o. for 6 months. After termination of the patients (5.0%) and HHV-6B in 210 patients (95.0%). In 202 tis-
antiviral treatment, patients underwent a control EMB to determine sue specimens (92%), copy numbers were <5 × 103 copies/μg of
HHV-6 replication and the inflammatory state of the myocardium. isolated myocardial DNA. The remaining 19 patients (8.6%) were
Blood samples were drawn daily for the first 2 weeks of treatment, with presumed to be ciHHV-6. Six were HHV-6 single infections and
extended intervals during follow-up to determine HHV-6 DNA levels. 13 had low-copy PB19V co-infection (<300 copies/μg of isolated
Due to recurrence of cardiac complaints shortly after termination DNA). The HHV-6 copy numbers were ∼105 copies/μg of iso-
of the antiviral treatment, p.o. administration of valganciclovir was
lated DNA (Figure 2A) in both cardiac tissue and PBMCs (median
continued in three ciHHV-6 patients. Two of them needed higher
158 184, range 74 454–401 995) and the viral load did not
dosages (1800 mg/day) to avoid recurrence of symptoms.
Changes of LVEF before and after treatment were determined decrease in follow-up studies over years, as would be expected for
by echocardiogaphy. Angina was scored as being present or not ciHHV-6 patients. Sequencing confirmed that 7 patients (36.8%)
present. Clinical improvement was defined as presence or absence of had ciHHV-6A and 12 (63.2%) had ciHHV-6B. Of the 19 ciHHV-6
pre-existing fatigue, angina, dyspnoea, a ≥10% improvement of LVEF, patients, 14 had mRNA transcripts, and 12 had viral transcripts
or a change by at least one NYHA class. >105 RNA copies/μg of RNA. In five patients, pre-treatment
mRNA levels were not analysed (P1 and P2) or respective RNA
materials were lacking (P17–P19).
Statistical analysis
Student’s t-test, one-way analysis of variance, 𝜒 2 , and Fisher’s exact test
were used as appropriate. All P-values were two-tailed; P-values <0.05 Clinical presentation of patients
were considered as statistically significant. All statistical analyses were
performed using the JMP software version 7.0 (SAS Institute Inc., Cary,
with chromosomally integrated human
NC, USA). herpesvirus 6
At the first onset of symptomatic heart disease, 18 out of the 19
adult ciHHV-6 patients (94.7%) clinically presented as myocarditis.
Results Five patients (26%, three with ciHHV-6A) complained about
sudden onset of angina pectoris with ST segment elevations and
Prevalence of human herpesvirus 6A positive cardiac enzymes mimicking acute myocardial infarction.
and B in cardiac patients Seven patients (37%, two with ciHHV-6A) suffered from acute
To determine if viruses are involved in the cardiac symptoms of the cardiac failure, with non-sustained ventricular tachycardia in one
patients, we screened the cardiac biopsies for a panel of viruses. patient. Five patients (26%, two with ciHHV-6A) complained of
Intriguingly, we identified 273/1656 patients (16.5%) positive for recent onset of fatigue, dyspnoea on exertion, and angina pectoris.
HHV-6 infection by nPCR. A total of 478 patients (28.8%) were Two patients presented with ventricular tachycardia or rapid-onset
virus negative while in 905 patients other viruses were detected DCM (both ciHHV-6B), respectively. At biopsy, angina and fatigue
(Supplementary Figure S1). HHV-6 single infection was found in 77 were slightly more frequent in ciHHV-6 than in HHV-6 patients
© 2014 The Authors
European Journal of Heart Failure © 2014 European Society of Cardiology
12 U. Kühl et al.
Figure 2 Detection and localization of chromosomally integrated human herpesvirus 6 (ciHHV-6) A and B in myocardial tissue. In baseline
endomyocardial biopsy (EMB) tissues of untreated ciHHV-6 patients, variable amounts of ciHHV-6 mRNA copy numbers (A) and viral
proteins (B, C) were detected by nested polymerase chain reaction (PCR)/quantitative PCR and immunohistochemical staining, respectively.
Virus particles were localized in tissue compartments by electron microscopy (D–J). Immunohistochemical staining with specific monoclonal
antibodies (mAbs) directed against envelope glycoprotein 60/110 of HHV-6A and B identified HHV-6A in cardiomyocytes (B) whereas HHV-6B
was detected in interstitial cells of myocardial tissue by mAbs directed against p101 of HHV-6B (C). Ultrastructural examination localized
HHV-6B virus particles in the vascular endothelium (D–E) while HHV-6A was also detected in degenerating cardiomyocytes (F–H). Herpesvirus
particles with nucleocapsid, tegument, and viral envelope are indicated by arrows (I).
(Supplementary material online, Table S1). All other clinical param- Screening of family members of patients
...................
eters were not different either between the HHV-6 species or
for chromosomally integrated human
in the ciHHV-6 genotypes. Systolic function remained unaffected
or only moderately decreased in most patients, suggesting that
herpesvirus and clinical symptoms
HHV-6 reactivation, similar to erythrovirus reactivation, is more Inheritance of ciHHV-6 would mean that other family members
frequently associated with symptoms of heart failure than with also harbour ciHHV-6 virus. We analysed blood samples of
structural changes and systolic LV dysfunction.23 first-degree relatives of three index patients (P1, P2, and P3;
© 2014 The Authors
European Journal of Heart Failure © 2014 European Society of Cardiology
Prevalence and reactivation of ciHHV-6 13
Figure 2 Continued
Table 1). Persisting HHV-6 copy numbers >105 DNA copies/μg of myocardial tissues of ciHHV-6A and -B patients. CiHHV-6
..........................................................................
indicative of ciHHV-6 were detected in several family members virions (P1–P3) were detected in vascular endothelial cells (ECs)
as depicted in the pedigrees of the three families (Figure 1). Five (Figure 2D and E). As seen in immunohistochemistry, HHV-6A virus
ciHHV-6 patient family members with unexplained heart failure particles were also present in the cytoplasm of cardiac myocytes
were reported; 11 were asymptomatic with respect to cardiac (Figure 2 F–I). Several cytoplasmic virions in cardiac myocytes
complaints. In one family, sudden cardiac death of the maternal contained a thick tegumental layer, suggesting that HHV-6 virions
grandmother at young age was reported (P1). From some asymp- successfully mature in these cells (Figure 2 F). Our data demonstrate
tomatic first-degree family members. blood samples were not that HHV-6 mRNA, structural proteins, and virions are present in
available. myocardial tissue of ciHHV-6 patients, due to ciHHV-6 reactivation
of the integrated strain (P1–P3).
Detection of viral mRNA, antigens,
and virions in myocardial tissue Suppression of DNA replication and viral
To determine if ciHHV-6 reactivates in the cardiac tissue, we RNA synthesis by antiviral therapy
analysed HHV-6 transcript levels, viral protein expression, and the To confirm that ciHHV-6 reactivation is indeed involved in cardiac
presence of virions in EMB samples. Viral mRNA transcripts were symptoms, six highly symptomatic patients for whom the treatment
detected in the myocardium of 14 ciHHV-6 patients (Figure 2A). costs were covered by their health insurance were treated with
Next, we analysed the biopsy specimen for the presence of ganciclovir. If HHV-6 is involved in the clinical symptoms, an
viral proteins.2 Immunohistochemical staining revealed HHV-6A/B improvement should occur under antiviral treatment of ciHHV-6
envelope glycoprotein 60/110 in some cardiomyocytes (Figure 2B) patients. Response to therapy was determined by EMB diagnostics
and the HHV-6B structural protein p101 in interstitial cells of the before and after 6 months treatment (Table 1). HHV-6 DNA
myocardium (Figure 2C). The presence of viral structural proteins and RNA levels of PBMCs were measured for permanent and
in the cardiac tissue suggests that virus replication indeed occurs in ongoing therapy monitoring (Figures 3 and 4). Six patients with
ciHHV-6 patients.2 To determine if infectious virions are formed, severe persisting symptoms of heart failure were treated with
we performed transmission electron microscopic (EM) analyses 900 mg/day of valganciclovir; a herpesvirus-specific inhibitor of
© 2014 The Authors
European Journal of Heart Failure © 2014 European Society of Cardiology
14 U. Kühl et al.
Table 1 Changes of clinical parameters during valganciclovir treatment of chromosomally integrated human
herpesvirus 6-positive patients
Patient P1 P2 P3 P4 P5 P6
...........................................................................................................................................
Baseline biopsy
LVEF (%) 55 70 61 51 67 18
NYHA 3 3 2 3 2 4
Angina + + + + + +
Dyspnoea + – + + – +
Fatigue + + + + + +
Diuretics + – – + – +
Spironolactone – – – – – +
Beta-blocker + + – + – +
ACE inhibitor + ARB + – + + + +
End of 6 months treatment
LVEF (%) 65 70 68 71 64 66
NYHA 2 2 2 2 2 2
Angina – – – – – –
Dyspnoea – – – – – +
Fatigue – – – + + +
Diuretics + – – + – +
Spironolactone – – – – – +
Beta-blocker + + – + – +
ACE inhibitor + ARB + – + + + +
Clinical improvement Yes Yes Yes Yes Yes Yes
Haemodynamic improvement Yes No No Yes No Yes
Persisting improvement (months) 0.5 0.5 1 12 12 15
Continous treatment with valganciclovir (mg/day) 1800 1800 900 No No No
Persisting improvement 12 months post-treatment Yes Yes Yes Yes Yes Yes
Follow-up (months) 30 24 74 92 92 72
Persisting improvement Yes Yes Yes No No No
LVEF (%) 62 72 61 50 42 55
NYHA 2 2 2 2 2 3
Angina – – – – – +
Dyspnoea – – – – + +
Fatigue – – – + + +
Diuretics – – – + + +
Spironolactone – – – – + +
Beta-blocker + – – + + +
ACE inhibitor + ARB – – + + + +
virus replication, for 6 months. Three of these patients (P1, P4, proton inhibitor taken by patient 3 in order to treat heartburn,
...............................................
and P6) had a minor co-infection with parvovirus, with copy resulted in higher levels of ciHHV-6 DNA and RNA copies/μg
numbers <300 copies/μg of RNA. After 2 weeks of treatment, all (Figure 4B and C) despite other medications remaining unchanged.
six reported a rapid improvement of symptoms and were free of HHV-6 reactivates preferentially in severe drug hypersensitivity
angina, dyspnoea, or fatigue, with a significant improvement of their reactions and ciHHV-6 patients may be more susceptible to HHV-6
physical capacity in daily life after 3 months of treatment. reactivation associated with adverse drug reactions.1 Pantoprazole
Measurements of HHV-6 mRNA levels (Figure 3A) in PBMCs triggers hypersensitivity reactions and it is possible that it might
revealed that DNA replication and RNA synthesis were eliminated trigger activation of the integrated HHV-6. No HHV-6 mRNA was
after antiviral therapy (Table 2). The absence of DNA replication detected in follow-up biopsies of all six patients after 6 months
was confirmed by FISH, which detected only the integrated HHV-6 of treatment (Table 1). Intriguingly, myocardial inflammation had
genome in interphase nuclei of the treated patients (Figure 3B and resolved in the ciHHV-6B patients but persisted in both ciHHV-6A
C). Although antiviral treatment coincided with a reduction of patients (Table 2).
the severity, frequency, and duration, these symptoms re-appeared During the following 12 months, clinical symptoms remained
for 2–3 days at 4- to 6-week intervals and were accompanied nearly absent in three patients (P4, P5, and P6). The other three
by elevated HHV-6 RNA levels (Figures 3A and 4A). Of interest, patients had a recurrence of fatigue, dyspnoea, and angina within
acute infections (Figure 3A) or co-medication with pantoprazole, a 4 weeks. Upon continuous ganciclovir treatment with an elevated
© 2014 The Authors
European Journal of Heart Failure © 2014 European Society of Cardiology
Prevalence and reactivation of ciHHV-6 15
Figure 3 Suppression of viral RNA and lytic infection by antiviral treatment. Ganciclovir treatment of a chromosomally integrated human
herpesvirus 6B (ciHHV-6B)-positive female patient (P3) with persisting high cardiac and systemic virus loads and cardiac involvement (A). HHV-6
RNA levels are shown as viral copy numbers per 1 μg of RNA. A symptomatic increase of mRNA (S) was noted between days 13 to 21 when
i.v. ganciclovir was changed to oral administration. During short symptomatic phases (S) at day 41 and 75, again mild increases of mRNA were
detected. Fluorescent in situ hybridization (FISH) analysis detecting the HHV-6 genome (anti-digoxigenin fluorescein isothiocyanate, green) in
interphase nuclei (4’,6-diamidino-2-phenylindole stain, blue) of lymphocytes from two patients with ciHHV-6A (B) and ciHHV-6B (C) treated
with valganciclovir. In contrast to uninfected (F) JJhan cells (E, F), HHV-6A- (D) and HHV-6B JJhan-infected cells (G) exhibit strong fluorescent
signals. Representative images are shown for each patient and the viral genome(s) are highlighted by arrows.
dosage of 1800 mg/day, clinical symptoms and myocardial function needed constant treatment to maintain this condition. Despite
..................................
improved or disappeared completely (P1–P3) (Table 1). Of note, unchanged heart failure medication, discontinuation of antiviral
symptoms reappeared within 2–4 days in P1, P2, and P3 whenever treatment was associated with the reappearance of both cardiac
medication was discontinued and vanished within 5–7 days when symptoms and viral mRNA, indicating a direct involvement of
treatment was restarted. HHV-6 in these symptoms.
Long-term follow-up of the three patients without prolonged
treatment (P4–P6) revealed that symptoms of heart failure with
impairment of myocardial function that had improved after the
6-month treatment course reappeared again ∼1 year later. Alter-
Discussion
nating elevated blood mRNA levels were detected in these patients We detected a high prevalence of HHV-6 infection in the myocar-
(Table 2). Symptoms thus improved upon beta-herpesvirus-specific dial tissue of patients who presented with symptoms of heart failure
antiviral treatment in 6/6 of treated patients but three of them in a clinically suspected setting of myocarditis (17.4%) or DCM
© 2014 The Authors
European Journal of Heart Failure © 2014 European Society of Cardiology
16 U. Kühl et al.
Figure 4 Sporadic recurrence of clinical complaints and viral replication during antiviral treatment. (A) Occurrence of clinical symptoms
under antiviral treatment is accompanied by an elevation of RNA copies of a representative patient (P4). Clinical symptoms (S) are indicated by
arrows and antiviral treatments are shown for the indicated period of times (black bars). A similar periodicity was reported by all six treated
patients. Sporadic (days 1444–1600) and constant (days 1600–30) Pantozol© uptake (40 mg per day p.o.), which was the only distinctive feature
reported by the patient during antiviral treatment, was paralleled by viral reactivation as indicated by a simultaneous increase of both human
herpesvirus 6 RNA (B) and DNA (C) genome copy numbers in P3.
© 2014 The Authors
European Journal of Heart Failure © 2014 European Society of Cardiology
Prevalence and reactivation of ciHHV-6 17
Table 2 Changes of myocardial parameters during treatment of chromosomally integrated human herpesvirus
6-positive patients with high and low doses of valganciclovir
Patient P1 P2 P3 P4 P5 P6
...........................................................................................................................................
Gender M M F F F F
Age (years) 34 41 51 59 64 65
HHV-6 genotype B A B A A B
Valganciclovir (mg/day) 1800 1800 900 900 900 900
Baseline biopsy
EMB (copies/μg DNA) Positive* 5.1 × 104 5.1 × 104 5.9 × 104 3.7 × 104 11.8 × 104
RNA/EMB copies/μg RNA ND* ND* 1.6 × 104 2.3 × 104 33.0 × 104 1.4 × 104
PBMC (copies/μg DNA) 16.5 × 104 14.2 × 104 6.5× 104 13.1 × 104 10.7 × 104 24.5 × 104
PBMC (copies/μg RNA) ND* ND* 1.0 × 104 1.2 × 104 6.1 × 101 6.3 × 102
CD3 (cells/mm2 ) >10* >10* 11.3 14.3 13.5 1.5
Intramyocardial inflammation Yes Yes Yes Yes Yes No
End of 6-month treatment
DNA/EMB copies/μg DNA ND* 17.7 × 104 23.2 × 104 9.0 × 104 10.6 × 104 16.1 × 104
RNA/EMB copies/μg RNA ND* Negative Negative Negative Negative Negative
PBMC (copies/μg DNA) 29.2× 104 15.0 × 104 13.4 × 104 10.8 × 104 15.0 × 104 10.8 × 104
PBMC (copies/μg RNA) Negative Negative Negative Negative Negative Negative
CD3 (cells/mm2 ) ND* ND* 3.6 12.5 17.5 9.6
Intramyocardial inflammation ND* ND* No Yes Yes No
Continous treatment with valganciclovir (mg/day) 1800 1800 900 No No No
PBMC (copies/μg DNA) 24.9 × 104 23.4 × 104 15.0 × 104 11.6 × 104 26.4 × 104 13.5 × 104
PBMC (copies/μg RNA) 0.36 × 103 Negative 0.60 × 103 1 × 101 1.2 × 103 1.8 × 104
EMB, endomyocardial biopsy; F, female; HHV-6, human herpesvirus 6; M, male; ND, not done; PBMC, peripheral blood mononuclear cell.
* No data analysis done in the external centre.
(14.0%). Most of these patients were infected with HHV-6B (95%). tissue specimens from heart biopsies and respective blood sam-
.................................................................................
In addition to HHV-6, 1.1% of the patients harboured ciHHV-6, ples for the presence of HHV-6 mRNA, viral proteins, and virions.
which is in accordance with data reported from other popula- HHV-6-specific mRNA was detected in both solid tissue and iso-
tions (0.4–0.8%).9,13,24 A high proportion of these patients har- lated PBMCs of the same patients, suggesting ciHHV-6 reactivation.
boured ciHHV-6A (37%), which is consistent with previous studies In addition, we detected HHV-6 envelope glycoprotein 60/110 in
indicating an increased prevalence of HHV-6-A for chromosomal cardiac myocytes and interstitial cells of the myocardium. Further-
integration.13 more, we could identify mature cytoplasmic virions with a thick
Primary HHV-6 infection causes febrile seizures or exanthema tegument layer by electron microscopy. Despite the limited num-
subitum (roseola infantum) in ∼5% of children, but remains subclini- ber of patients, our study provides the evidence that ciHHV-6 can
cal in most. Reactivation in older children and in adults is associated replicate in degenerating cardiomyocytes and other cells and that
with more serious diseases.9,13,25 CiHHV-6 appears to be associ- this reactivation could result in cardiac symptoms.
ated with an increased risk of myocarditis. At the first onset of This antiviral treatment abolished viral transcripts indicative of
symptomatic heart disease, 18 out of 19 of our adult patients active HHV-6 replication and coincided with a rapid improve-
(94.7%) presented with clinical signs suggesting myocarditis, includ- ment of the clinical symptoms. In addition, no DNA replication
ing acute angina and dyspnoea, elevated cardiac enzymes, or ECG was detectable under treatment and only the integrated virus
changes mimicking myocardial infarction. This is considerably more genome was detectable by FISH. The association of recurrent
frequent than generally observed in non-chromosomally integrated cardiac complaints together with elevated ciHHV-6 mRNA lev-
HHV-6 infection (9.8%) or virus-negative patients (10.9%). The els and the amelioration of symptoms with decreased transcript
patients with a low copy number did not harbour ciHHV-6 in the levels upon ganciclovir treatment with constant co-medication indi-
germline. Therefore, it is possible that the low number of genome cate that HHV-6 reactivation in heart and other tissues is possible
copies could correspond to latently infected cells or reactivation and is involved in the symptoms of these ciHHV-6 patients. Dam-
of HHV-6 from latency. age of ECs caused by HHV-6 reactivation in ciHHV-6 patients
Several recent studies have suggested that ciHHV-6 can reacti- may explain complaints of angina of our patients as a sequela
vate from its integrated state in vitro and in vivo.16,26 – 28 In addition, of myocyte and vascular endothelial dysfunction, as shown for
ciHHV-6 individuals may be unable to defend themselves against PVB19.30 Persistence of myocardial inflammation after treatment
community-acquired strains.29 To demonstrate that ciHHV-6 can was only detectable in patients with the HHV-6 genotype A.
indeed reactivate from latency in differentiated cells, we analysed Whether this relates to a virus-triggered autoimmune response or
© 2014 The Authors
European Journal of Heart Failure © 2014 European Society of Cardiology
18 U. Kühl et al.
reflects a virus subtype-specific pathophysiology remains unknown. for an extended treatment study with a larger cohort of ciHHV-6
........................................................................................................................................................................................................................
A new mouse model of HHV-6A infection suggests that HHV-6A patients with cardiac disease in a randomized manner and including
can persist and cause inflammation in the absence of replication a placebo control. In addition, analysis of the genomes of ciHHV-6
via the up-regulation of chemokines CCL5, CCL2, CXCL10, and patients with cardiac disease might reveal genetic predispositions,
CCL1.31 HHV-6A encodes a distant chemokine homologue U83A allowing a predictive genetic diagnosis.
that results in inflammation.32 Changes of the inflammatory state,
however, do not explain the rapid and reversible clinical changes in
association with initiation or interruption of the antiviral treatment. Conclusion
Valganciclovir is routinely used for HHV-6-induced limbic
In our study we could demonstrate that ciHHV-6 reactivates
encephalitis, and is used in most transplant centres for transplant
in blood and heart tissue and that antiviral treatment efficiently
complications where HHV-6 is suspected. Several case reports
decreased HHV-6 transcripts. HHV-6 transmitted via the germline
have demonstrated that ciHHV-6 patients with encephalitis and
affects every cell of the body and may not only reactivate in heart
chronic fatigue syndrome respond to antiviral therapy.33 – 36 In
or blood cells, but also in other cells of the body. This reactiva-
our study, we successfully treated six highly symptomatic patients
tion could cause unexplained symptomatic conditions in cardiac
with cardiac involvement for 6 months with ganciclovir. The
and non-cardiac diseases. Antiviral treatment abolishes viral tran-
symptoms of all patients improved, with a reduced frequency and
scriptional activity and was associated with a reduced severity of
shorter duration of angina, palpitations, dyspnoea, and fatigue,
clinical symptoms, suggesting that this herpesvirus-specific antiviral
and improved physical capacity in daily life that coincided with the
drug might be effective in some ciHHV-6 heart failure patients.
abrogation of HHV-6 mRNA transcripts. One ciHHV-6B and two
ciHHV-6A patients remained asymptomatic until 12 months after
treatment before symptoms reappeared. Acknowledgements
In three patients, angina, dyspnoea, fatigue, and physical disabil-
ity reappeared within days after termination of the therapy. These We thank Mrs K. Winter, S. Ochmann, C. Seifert, and G. Zingler,
patients needed a continuous and more intensive antiviral ther- Berlin, Germany for their excellent technical assistance.
apy to avoid recurrence of symptoms. In the patients without a
prolonged treatment, symptoms and myocardial function remained Supplementary Information
stable but, symptoms of heart failure and impairment of myocar-
dial function in association with alternating mRNA levels recurred Additional Supporting Information may be found in the online
during long-term follow-up. version of this article:
Our data indicate that antiviral treatment reduces HHV-6 tran- FigureS1. Identification of ciHHV-6 patients and selection of six
scriptional activity in the heart and PBMCs of ciHHV-6 patients. symptomatic patients for whom the treatment costs were covered
However, the recurrent symptomatic episodes indicate that cardiac by a health insurance.
complaints may rise above a certain threshold of HHV-6 transcrip- TableS1. Characteristics of ciHHV-6 and non-ciHHV-6 patients
tional activity in the heart. To test this hypothesis, long-term mon- TableS2. Primers used for sequencing
itoring of HHV-6 transcripts in a larger cohort will be necessary
and could reveal possible factors that influence HHV-6 reactivation
in ciHHV-6 patients.
Funding
This work was supported by grants of the German Research Founda-
tion (DFG), Transregional Collaborative Research Centre ‘Inflamma-
Limitations tory Cardiomyopathy–Molecular Pathogenesis and Therapy’ (SFB TR
In this study we used tissues from symptomatic cardiac patients as 19 04).
an example to describe general features of the ciHHV-6 infection, Conflict of interest: none declared.
a rarely recognized condition that may also be associated with
a number of non-cardiac diseases. Our clinical information in
References
this retrospective study is limited due to the fact that a biopsy
1. Pellett PE, Ablashi DV, Ambros PF, Agut H, Caserta MT, Descamps V, Flamand
is still infrequently used at the time of diagnosis to confirm L, Gautheret-Dejean A, Hall CB, Kamble RT, Kuehl U, Lassner D, Lautenschlager
a possible virus-associated inflammatory process as the cause IT, Loomis KS, Luppi M, Lusso P, Medveczky PG, Montoya JG, Mori Y, Ogata
of a cardiac disease. Because viral infections generally present M, Pritchett JC, Rogez S, Seto E, Ward KN, Yoshikawa T, Razonable RR.
Chromosomally integrated human herpesvirus 6: questions and answers. Rev Med
with uncharacteristic symptoms, the proof of ciHHV-6 was often Virol 2012;22:144–155.
delayed to a time point when specific parameters were no longer 2. Krueger GRF, Rojo J, Buja LM, Lassner D, Kuehl U. Human herpesvirus-6
detected. The number of treated patients is still limited by the (HHV-6) is a possible cardiac pathogen: an immunohistological and ultrastructural
study. Hosp Gen 2008;71:187–191.
number of patients that presented in our clinic with pronounced 3. Caruso A, Rotola A, Comar M, Favilli F, Galvan M, Tosetti M, Campello C, Caselli
cardiac symptoms, and the fact that the treatment costs were E, Alessandri G, Grassi M, Garrafa E, Cassai E, Di Luca D. HHV-6 infects human
not universally covered by their health insurance. Due to the low aortic and heart microvascular endothelial cells, increasing their ability to secrete
proinflammatory chemokines. J Med Virol 2002;67:528–533.
number of patients, it was not possible to include a control group 4. Lautenschlager I, Razonable RR. Human herpesvirus-6 infections in kidney, liver,
and to randomize the study. However, our study provides a basis lung, and heart transplantation: review. Transplant Int 2012;25:493–502.
© 2014 The Authors
European Journal of Heart Failure © 2014 European Society of Cardiology
Prevalence and reactivation of ciHHV-6 19
5. Ratnamohan VM, Chapman J, Howse H, Bovington K, Robertson P, Byth K, Allan 6 variant B strain Z29: identification and characterization of the gene and
..............................................................................................................................
R, Cunningham AJ. Cytomegalovirus and human herpesvirus 6 both cause viral mapping of a variant-specific monoclonal antibody reactive epitope. Virology
disease after renal transplantation. Transplantation 1998;66:877–882. 1993;195:521–531.
6. Fotheringham J, Akhyani N, Vortmeyer A, Donati D, Williams E, Oh U, Bishop M, 22. Kaufer BB. Detection of integrated herpesvirus genomes by fluorescence in situ
Barrett J, Gea-Banacloche J, Jacobson S. Detection of active human herpesvirus-6 hybridization (FISH). Methods Mol Biol 2013;1064:141–152.
infection in the brain: correlation with polymerase chain reaction detection in 23. Kühl U, Lassner D, Dorner A, Rohde BM, Escher F, Seeberg B, Hertel E, Tschope
cerebrospinal fluid. J Infect Dis 2007;195:450–454. C, Gross U, Poller W, Schultheiss HP. A distinct subgroup of cardiomyopathy
7. Hall CB, Caserta MT, Schnabel KC, Long C, Epstein LG, Insel RA, Dewhurst S. patients characterized by transcriptionally active cardiotropic erythrovirus and
Persistence of human herpesvirus 6 according to site and variant: possible greater altered cardiac gene expression. Basic Res Cardiol 2013;108:372–382.
neurotropism of variant A. Clin Infect Dis 1998;26:132–137. 24. Potenza L, Barozzi P, Masetti M, Pecorari M, Bresciani P, Gautheret-Dejean A,
8. Kühl U, Pauschinger M, Noutsias M, Seeberg B, Bock T, Lassner D, Poller Riva G, Vallerini D, Tagliazucchi S, Codeluppi M, Di Benedetto F, Gerunda GE,
W, Kandolf R, Schultheiss HP. High prevalence of viral genomes and multiple Narni F, Torelli G, Luppi M. Prevalence of human herpesvirus-6 chromosomal
viral infections in the myocardium of adults with ‘idiopathic’ left ventricular integration (CIHHV-6) in Italian solid organ and allogeneic stem cell transplant
dysfunction. Circulation 2005;111:887–893. patients. Am J Transplant 2009;9:1690–1697.
9. Leong HN, Tuke PW, Tedder RS, Khanom AB, Eglin RP, Atkinson CE, Ward 25. Morissette G, Flamand L. Herpesviruses and chromosomal integration. J Virol
KN, Griffiths PD, Clark DA. The prevalence of chromosomally integrated 2010;84:12100–12109.
human herpesvirus 6 genomes in the blood of UK blood donors. J Med Virol 26. Hall CB, Caserta MT, Schnabel KC, Shelley LM, Carnahan JA, Marino AS, Yoo C,
2007;79:45–51. Lofthus GK. Transplacental congenital human herpesvirus 6 infection caused by
10. Ward KN, Thiruchelvam AD, Couto-Parada X. Unexpected occasional persis- maternal chromosomally integrated virus. J Infect Dis 2010;201:505–507.
tence of high levels of HHV-6 DNA in sera: detection of variants A and B. J Med 27. Huang Y, Hidalgo-Bravo A, Zhang E, Cotton VE, Mendez-Bermudez A, Wig G,
Virol 2005;79:563–570. Medina-Calzada Z, Neumann R, Jeffreys AJ, Winney B, Wilson JF, Clark DA,
11. Arbuckle JH, Medveczky MM, Luka J, Hadley SH, Luegmayr A, Ablashi D, Dyer MJ, Royle NJ. Human telomeres that carry an integrated copy of human
Lund TC, Tolar J, De Meirleir K, Montoya JG, Komaroff AL, Ambros PF, herpesvirus 6 are often short and unstable, facilitating release of the viral genome
Medveczky PG. The latent human herpesvirus-6A genome specifically integrates from the chromosome. Nucleic Acid Res 2013;42:315–327.
in telomeres of human chromosomes in vivo and in vitro. Proc Natl Acad Sci USA 28. Prusty BK, Krone G, Rudel T. Reactivation of chromosomally integrated human
2010;107:5563–5568. herpesvirus-6 by telomeric circle formation. PLOS Genet 2013;9:e1004033.
12. Arbuckle JH, Pantry SN, Medveczky MM, Prichett J, Loomis KS, Ablashi D, 29. Pantry SN, Medveczky MM, Arbucle JH, Luka J, Montoya JG, Hu J, Renne
Medveczky PG. Mapping thetelomere integrated genome of human herpesvirus R, Peterson D, Pritchett JC, Ablashi DV, Medveczky PG. Persistent human
6A and 6B. Virology 2013;442:3–11. herpesvirus-6 infection in patients with an inherited form of the virus. J Med
13. Hall CB, Caserta MT, Schnabel K, Shelley LM, Marino AS, Carnahan JA, Yoo C, Virol 2013;85:1940–1949.
Lofthus GK, McDermott MP. Chromosomal integration of human herpesvirus 30. Schmidt-Lucke C, Spillmann F, Bock T, Van Linthout S, Kühl U, Schultheiss
6 is the major mode of congenital human herpesvirus 6 infection. Pediatrics HP, Tschoepe C. Interferon-beta modulates endothelial damage in patients
2008;122:513–520. with cardiac persistence of parvovirus B19V. J Infectious Dis 2010;201:
14. Flammand LL, Krueger GRF, Ablashi DV, eds. Human Herpesviruses HHV-6A, 936–945.
HHV-6B, and HHV-7: Diagnosis and Clinical Management. Amsterdam: Elsevier; 31. Reynaud JM, Jegou JF, Welsch JC, Horvat B. Human herpesvirus 6A infection in
2014. CD46 transgenic mice: viral persistence in the brain and increased production of
15. Endo A, Watanabe K, Ohye T, Suzuki K, Matsubara T, Shimizu N, Kurahashi proinflammatory chemokines via Toll-like receptor 9. J Virol 2014;88:5421–5436.
H, Yoshikawa T, Katano H, Inuoue N, Imai K, Takagi M, Morio T, Mizutani 32. Dewin DR, Catusse J, Gompels U. Identification and caracterization of U83A
S. Molecular and virological evidence of viral activation from chromosomally viral chemokine, a broad and potent beta-chemokine agonist for human
integreted human herpesvirus 6A in a patient with x-linked severe combined CCRs with unique selectivity and inhibition by spliced isoforms. Immunology
immunodeficiency. Clin Infect Dis 2014;59:545–548. 2006;176:544–556.
16. Gravel A, Hall CB, Flammand L. Sequence analysis of transplacentally acquired 33. Montoya JG, Neely MN, Gupta S, Lunn MR, Loomis KS, Pritchett JC, Polsky B,
human herpesvirus 6 DNA is consistent with transmission of a chromosomally Medveczky PG. Antiviral therapy of two patients with chromosomally-integrated
integrated reactivated virus. J Infect Dis 2013;207:1585–1589. human herpesvirus-6A presenting with cognitive dysfunction. J Clin Virol
17. Kühl U, Lassner D, Pauschinger M, Gross UM, Seeberg B, Noutsias M, Poller 2012;55:40–45.
W, Schultheiss HP. Prevalence of erythrovirus genotypes in the myocardium of 34. Watt T, Oberfoell S, Balise R, Lunn MR, Kar AK, Merrihew L, Bhangoo MS,
patients with dilated cardiomyopathy. J Med Virol 2008;80:1243–1251. Montoya JG. Response to valganciclovir in chronic fatigue syndrome patients
18. Aretz HT. Myocarditis: the Dallas criteria. Hum Pathol 1987;18:619–624. with human herpesvirus 6 and Epstein–Barr virus IgG antibody titers. J Med Virol
19. Kühl U, Noutsias M, Seeberg B, Schultheiss HP. Immunohistological evidence for 2012;84:1967–1974.
a chronic intramyocardial inflammatory process in dilated cardiomyopathy. Heart 35. Troy SB, Blackburn BG, Yeom K, Caufield AKF, Bhangoo MS, Montoya JG.
1996;75:295–300. Immunocompetent adult with chromosomally integrated human herpesvirus 6
20. Noutsias M, Seeberg B, Schultheiss HP, Kuhl U. Expression of cell adhesion and clinical response to treatment with foscanet plus ganciclivir. Clin Inf Dis
molecules in dilated cardiomyopathy: evidence for endothelial activation in 2008;47:e93–e96.
inflammatory cardiomyopathy. Circulation 1999;99:2124–2131. 36. Wittekind B, Berger A, Porto L, Grüttner HP, Becker M, Lehrnbecher T. Human
21. Pellett PE, Sanchez-Martinez D, Dominguez G, Black JB, Anton E, Greenamoyer herpes virus-6 DNA in cerebrospinal fluid of children undergoing therapy for
C, Dambaugh TR. A strongly immunoreactive virion protein of human herpesvirus acute leukemis. Br J Haematol 2009;145:533–550.
© 2014 The Authors
European Journal of Heart Failure © 2014 European Society of Cardiology
You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Star Wars - Medical Sourcebook PDFDocument140 pagesStar Wars - Medical Sourcebook PDFevilnerf100% (5)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Orthopedic NursingDocument46 pagesOrthopedic Nursingposh0038No ratings yet
- Manual IcuDocument217 pagesManual IcuEmil Zatopek100% (3)
- Adult Health Final Study GuideDocument5 pagesAdult Health Final Study GuideNurseNancy93100% (1)
- Basic Nursing PharmacologyDocument78 pagesBasic Nursing PharmacologyLloyd Rafael EstabilloNo ratings yet
- Post-ACLS Megacode Flashcards - QuizletDocument9 pagesPost-ACLS Megacode Flashcards - QuizletMaya LaPradeNo ratings yet
- Laporan Pelayanan PKPP / Ukp Dokter Internship Rs Muhammadiyah BandungDocument8 pagesLaporan Pelayanan PKPP / Ukp Dokter Internship Rs Muhammadiyah BandungVirissa Calista HarbaindoNo ratings yet
- Logo NegaraDocument448 pagesLogo NegaraIndah PurnamasariNo ratings yet
- Polymyxin B: Similarities To and Differences From Colistin (Polymyxin E)Document12 pagesPolymyxin B: Similarities To and Differences From Colistin (Polymyxin E)Anggun NurhidayahNo ratings yet
- Questions and AnswerDocument5 pagesQuestions and AnswerPatricia Camille Ponce JonghunNo ratings yet
- Gengigel For GingivitisDocument7 pagesGengigel For GingivitisIka Dewi RahmawatiNo ratings yet
- COVID-19 Outbreak, Its Impact On Global EconomyDocument110 pagesCOVID-19 Outbreak, Its Impact On Global EconomyramaramoinNo ratings yet
- Drug Abuse: Short-Term EffectsDocument2 pagesDrug Abuse: Short-Term EffectsYeonjin ChoiNo ratings yet
- Conscious SedationDocument65 pagesConscious SedationAjay Kumar YadavNo ratings yet
- Brajac - ProtocolDocument13 pagesBrajac - Protocolthanh ngôNo ratings yet
- 2021 Small For Gestational Age - StatPearls - NCBI BookshelfDocument12 pages2021 Small For Gestational Age - StatPearls - NCBI BookshelfIlda IldaNo ratings yet
- Etiology of Stroke PDFDocument2 pagesEtiology of Stroke PDFMichelle0% (1)
- Aminoglycosides and SulfonamidesDocument35 pagesAminoglycosides and SulfonamidesPhoenixNo ratings yet
- Chapter 22, PharmacologyDocument25 pagesChapter 22, PharmacologyDurgaNadellaNo ratings yet
- Hospital Impact Emergency DepartmentDocument20 pagesHospital Impact Emergency DepartmentydtrgnNo ratings yet
- Neisseria Spp.Document22 pagesNeisseria Spp.sajad abasNo ratings yet
- 46 135 1 PB PDFDocument6 pages46 135 1 PB PDFpriscilla harmanyNo ratings yet
- Pulmonary Aneurysms Arteriovenous and FistulasDocument9 pagesPulmonary Aneurysms Arteriovenous and FistulasAlvaro OlateNo ratings yet
- Newspaper Report Sample 1Document2 pagesNewspaper Report Sample 1Susmita NathNo ratings yet
- Letter To Parents From PHMC MH 11-3-20Document1 pageLetter To Parents From PHMC MH 11-3-20WZZM NewsNo ratings yet
- Operating Instructions: EpilatorDocument7 pagesOperating Instructions: EpilatorMohamed HassanNo ratings yet
- IridocyclitisDocument4 pagesIridocyclitisadjcdaughtNo ratings yet
- Congress Program September 2022 Anglisht 1 1Document17 pagesCongress Program September 2022 Anglisht 1 1ediNo ratings yet
- Dental Hospital in VijayawadaDocument9 pagesDental Hospital in Vijayawadakrishna dentalNo ratings yet
- Risk Assesment For StudioDocument5 pagesRisk Assesment For StudioaishahkhanNo ratings yet