You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Fanuc NCGuide PMC Simulation FunctionDocument121 pagesFanuc NCGuide PMC Simulation FunctionkenNo ratings yet
- Forces and MotionDocument22 pagesForces and MotiongamahimeNo ratings yet
- Strategy Implementation, Evaluation and ControlDocument6 pagesStrategy Implementation, Evaluation and Controlbonny MishNo ratings yet
- PESTEL Analysis of MoroccoDocument2 pagesPESTEL Analysis of Moroccoethernalx67% (15)
- MARY, Woman of Faith, Hope, Love (Lyrics & Chords)Document2 pagesMARY, Woman of Faith, Hope, Love (Lyrics & Chords)Jessa Marie Maquiling88% (8)
- Virgin Galactic Profile & Performance Business ReportDocument10 pagesVirgin Galactic Profile & Performance Business ReportLoic PitoisNo ratings yet
- University of Tennessee Religious ExemptionDocument3 pagesUniversity of Tennessee Religious ExemptionDonnaNo ratings yet
- PDF Laporan Pendahuluan Maternitas Mastitis DDDocument17 pagesPDF Laporan Pendahuluan Maternitas Mastitis DDAlifia Nurdani DarmawanNo ratings yet
- Keywords: Congenital Deafness, Family Support, Early DetectionDocument8 pagesKeywords: Congenital Deafness, Family Support, Early DetectionAlifia Nurdani DarmawanNo ratings yet
- Diagnosis and Management of Congenital Sensorineural Hearing LossDocument10 pagesDiagnosis and Management of Congenital Sensorineural Hearing LossAlifia Nurdani DarmawanNo ratings yet
- Tenosynovitis SupuratifDocument9 pagesTenosynovitis SupuratifAlifia Nurdani DarmawanNo ratings yet
- EBOOK6131f1fd1229c Unit 3 Ledger Posting and Trial Balance PDFDocument44 pagesEBOOK6131f1fd1229c Unit 3 Ledger Posting and Trial Balance PDFYaw Antwi-AddaeNo ratings yet
- Article Role of Zinc Post-Injury Wound Healing: Special inDocument3 pagesArticle Role of Zinc Post-Injury Wound Healing: Special inVinicio Rodriguez MirandaNo ratings yet
- Drug-Induced Sleep Endoscopy (DISE)Document4 pagesDrug-Induced Sleep Endoscopy (DISE)Luis De jesus SolanoNo ratings yet
- SHPL Product Order Form 2021Document4 pagesSHPL Product Order Form 2021anuradha100% (3)
- Literature Review of Centella AsiaticaDocument6 pagesLiterature Review of Centella Asiaticaea3vk50y100% (1)
- Bihar-Board-Intermediate-Mathematics-Protect KeyDocument37 pagesBihar-Board-Intermediate-Mathematics-Protect Keyapi-335786032No ratings yet
- HW 2Document12 pagesHW 2Munish RanaNo ratings yet
- Ol7 SecurityDocument84 pagesOl7 Securityneaman_ahmedNo ratings yet
- SDS - Molykote 1000Document8 pagesSDS - Molykote 1000Zarni KyawNo ratings yet
- The Young Muslim Muharram 1429 January 2008Document12 pagesThe Young Muslim Muharram 1429 January 2008Amthullah Binte YousufNo ratings yet
- Jess's Heart Is Racing at 100 Miles Per Hour.Document3 pagesJess's Heart Is Racing at 100 Miles Per Hour.vexagon wallowNo ratings yet
- James Rachels - What Is MoralityDocument26 pagesJames Rachels - What Is MoralityKiara Lagrisola100% (1)
- 24 - Mubangizi-WHOPQP GMP Inspections UpdatesDocument17 pages24 - Mubangizi-WHOPQP GMP Inspections UpdatessamxuNo ratings yet
- 22661-RET Notes-UNIT 02Document25 pages22661-RET Notes-UNIT 02jayeshdeore398No ratings yet
- Geologic Report Arches NationalDocument9 pagesGeologic Report Arches NationalJacob AndersonNo ratings yet
- Management of Developing DentitionDocument51 pagesManagement of Developing Dentitionahmed alshaariNo ratings yet
- Assignment 3: Course Title: ECO101Document4 pagesAssignment 3: Course Title: ECO101Rashik AhmedNo ratings yet
- (267.) SWOT - Cruise Industry & CarnivalDocument2 pages(267.) SWOT - Cruise Industry & CarnivalBilly Julius Gestiada100% (1)
- QP English Viii 201920Document14 pagesQP English Viii 201920Srijan ChaudharyNo ratings yet
- User Manual: Series 7Document44 pagesUser Manual: Series 7Roniel ManjaresNo ratings yet
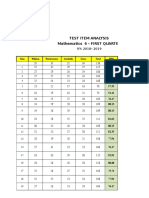
- Test Item Analysis Mathematics 6 - FIRST QUARTER: Item Wisdom Perseverance Gratitude Grace Total MPSDocument6 pagesTest Item Analysis Mathematics 6 - FIRST QUARTER: Item Wisdom Perseverance Gratitude Grace Total MPSQUISA O. LAONo ratings yet
- Fender Re-Issue 62 Jazzmaster Wiring DiagramDocument1 pageFender Re-Issue 62 Jazzmaster Wiring DiagrambenitoNo ratings yet
- Laboratory Activity No 3Document11 pagesLaboratory Activity No 3MAE MALALUANNo ratings yet