You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5807)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (843)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (346)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Functional Exposure ReportDocument48 pagesFunctional Exposure Reportdeepak kumarNo ratings yet
- 4x4 - Hummer - UK Manual - PCDocument24 pages4x4 - Hummer - UK Manual - PCHan SoloNo ratings yet
- Climaveneta Installation Manuals Generale - enDocument20 pagesClimaveneta Installation Manuals Generale - enNhật Phong NguyễnNo ratings yet
- Cambridge Assessment International Education: Economics 0455/12 March 2018Document2 pagesCambridge Assessment International Education: Economics 0455/12 March 2018farahNo ratings yet
- Case Study MilitaryDocument1 pageCase Study Militaryrazvan6b49No ratings yet
- Public Administration FinalDocument18 pagesPublic Administration FinalDon Jeffrey100% (1)
- BasixDocument4 pagesBasixcinderella6No ratings yet
- ICAODocument55 pagesICAOben folds100% (1)
- Personal StatementDocument2 pagesPersonal Statementapi-660808389No ratings yet
- CHANCROIDDocument13 pagesCHANCROIDPradeep YarasaniNo ratings yet
- 4 The Manufacture of Spun Concrete Poles PDFDocument85 pages4 The Manufacture of Spun Concrete Poles PDFSuyenthan Sathish100% (1)
- Taylor and Scientific Management - Administrative ThinkersDocument5 pagesTaylor and Scientific Management - Administrative ThinkersAshish SharmaNo ratings yet
- Presonus Hp2 Manual en de Es FRDocument8 pagesPresonus Hp2 Manual en de Es FRrobochetNo ratings yet
- Blaze Master Mysterium of The UniverseDocument117 pagesBlaze Master Mysterium of The UniverseStanisław Giers100% (1)
- Preverbal Stages of DevelopmentDocument17 pagesPreverbal Stages of DevelopmentKhristina Anne AmaNo ratings yet
- © 2015 F1F9 LTD: (Standard) (F1F9 Utility)Document2 pages© 2015 F1F9 LTD: (Standard) (F1F9 Utility)mahmoud.alnouri2099No ratings yet
- Chapter 15 - 3rd Ed. (Chap. 15 - 4, 5 Ed. Chap. 16, 6 Ed.)Document18 pagesChapter 15 - 3rd Ed. (Chap. 15 - 4, 5 Ed. Chap. 16, 6 Ed.)Anonymous cuWS3Q2No ratings yet
- Your CatDocument76 pagesYour CatAkk PhotgrNo ratings yet
- Crim 4 ModuleDocument55 pagesCrim 4 Moduleaya brea antalanNo ratings yet
- Math JIngleDocument2 pagesMath JIngleLouilaine OgalescoNo ratings yet
- Benefits of Column FlotationDocument5 pagesBenefits of Column FlotationMohamed DraaNo ratings yet
- Managing Data ConcurrencyDocument17 pagesManaging Data ConcurrencyJerry OlbinsonNo ratings yet
- Module 4 - The Consumer Decision ProcessDocument17 pagesModule 4 - The Consumer Decision ProcessSha ShaNo ratings yet
- Simple Queen RearingDocument8 pagesSimple Queen RearingAyvz Martija LambioNo ratings yet
- Pepsi Miniproject8Document68 pagesPepsi Miniproject8sudhakar5472No ratings yet
- Boric Acid, Powder NF: Safety Data SheetDocument6 pagesBoric Acid, Powder NF: Safety Data SheetMikkha EsguerraNo ratings yet
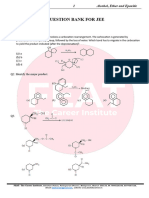
- Question Bank For Jee: Objective QuestionsDocument44 pagesQuestion Bank For Jee: Objective QuestionsYash KapoorNo ratings yet
- Chapter 3Document49 pagesChapter 3Trang ĐoànNo ratings yet
- Gambar CWS SulungDocument10 pagesGambar CWS Sulunghendrik rustendiNo ratings yet
- Describing People WorksheetDocument2 pagesDescribing People WorksheetFco Javier Gomez GarciaNo ratings yet