Frozen shoulder
Overview of Frozen Shoulder
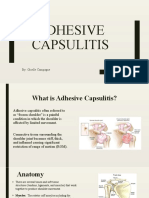
Frozen shoulder, or adhesive capsulitis, is a thickening of the shoulder capsule
around the glenohumoral shoulder joint. It is usually a result of the
inflammation, scarring, tightening of the connective tissue surrounding the
shoulder joint capsule. It can be classified as a loss of both passive and active
range of motion in the shoulder with associated pain and stiffness.
Causes
• Identifying the actual cause can be very unclear
• Injury, trauma, surgery or prolonged periods on immobility can be a
contributing factor.
• Age can be a factor 40 – 60 yr old category
• More common in females (70%)
• Diabetes, Thyroid conditions, Parkinson’s , Cardiovascular disease
can predispose.
• Poor biomechanics and posture
Symptoms or Problems
Symptoms begin as a gradual onset and progress through the following
3 stages.
1. Painful ( Freezing ) stage
• Stiffness in the shoulder joint
• Pain with any shoulder movement (worse at night)
• Limited ROM
• Little to no response to anti-inflammatory medication
2. Frozen ( Adhesion ) stage
• Pain begins to subside
• ROM is significantly limited
• Pain is present with end ROM ie elevation , external rotation
3. Thawing ( Resolution ) stage
• ROM begins to improve
• Spontaneous restoration of freedom in the joint capsule
Note: Recovery from frozen shoulder can take up to 18 to 42 months. It can
often affect the other shoulder. Associated symptoms can refer to the upper
arm, upper back and neck region, resulting in stiffness in any of these areas.
Treatment
Treatment is difficult and requires an considered approach and patient
compliance to improve outcomes. The range of treatment options include:
• Early treatment would benefit from rest , ice, compression and
elevation ( RICE ) and when inflammation is present
• Distention injections into the effected shoulder capsule (eg: sterile
water, iced saline or corticosteroid injections )
• Surgery ( open arthroscopic capsular release to remove scar tissue
ect )
• Conservative exercise to maintain a comfortable ROM
• Manipulation ( under general anaesthetic )
Exercise Considerations
All movement should be within a pain free range. Avoid aggravating symptoms
by pushing end ROM such as overhead arms , side lying or weight bearing
• Maintain a comfortable range of motion with gentle exercise
• Focus on maintaining strength and mobility
• Address associated / surrounding areas
• Last stages ( resolution ) should involve a focus on a return to
functional ADL’s
• Increase muscle tone to any atrophy that may have occurred
References and further reading.
Funk, Leonard. Frozen Shoulder, 2007. www.shoulderdoc.co.uk
Nash, P. Shoulder Pain. Current Therapy 1999 Apr, 40 (4)
Jing-Ian Yang, Chein-wei Chang, et al, Mobilization Techniques in Subjects with
Frozen Shoulder Syndrome: Randomised Multiple Treatment Trial. Vol. 87
Number 10 Physical Therapy, October 2007.
Ruiz, Jose Orlando, Positional Stretching of the Coracohumeral Ligament on a
Patient with Adhesive Capsulate: A Case Report. Journal of Manual &
Manipulative Therapy Vol.17 No.1
www.PhysioAdvisor.com Frozen Shoulder (Adhesive capsulitis)
http://www.frozenshoulder.com/your_diagnosis.php
You might also like
- 8 Sample Care Plans For ACDFDocument11 pages8 Sample Care Plans For ACDFacasulla98No ratings yet
- Frozen Shoulder - Adhesive Capsulitis - OrthoInfo - AAOSDocument6 pagesFrozen Shoulder - Adhesive Capsulitis - OrthoInfo - AAOSpempekplgNo ratings yet
- Herniated Nucleus PulposusDocument41 pagesHerniated Nucleus PulposusMichael John F. Natividad100% (2)
- 8 Harris Hip ScoreDocument1 page8 Harris Hip Scorestevebravo81100% (1)
- Frozen ShoulderDocument11 pagesFrozen Shoulderjean catherine singoa toyaNo ratings yet
- Frozen...Document24 pagesFrozen...Tutut RachmawatiNo ratings yet
- Frozen ShoulderDocument18 pagesFrozen ShoulderChitra ChauhanNo ratings yet
- Evaluation and Treatment of Common Musculoskeletal Disorder of The ShoulderDocument42 pagesEvaluation and Treatment of Common Musculoskeletal Disorder of The ShoulderhdthhhhNo ratings yet
- ياسمين العودةDocument3 pagesياسمين العودةSondos AshourNo ratings yet
- Presentation 3Document12 pagesPresentation 3api-547492718No ratings yet
- Presentation 26Document10 pagesPresentation 26yousufNo ratings yet
- Frozen Shoulder (Adhesive Capsulitis)Document7 pagesFrozen Shoulder (Adhesive Capsulitis)Rully Riyan DikaNo ratings yet
- Adhesive Capsulitis or Frozen SholderDocument24 pagesAdhesive Capsulitis or Frozen Sholdersanalcrazy100% (1)
- CME Shoulder Rehab Doc TalkDocument43 pagesCME Shoulder Rehab Doc TalkElliya RosyidaNo ratings yet
- Intervertebral Disc ProlapseDocument46 pagesIntervertebral Disc Prolapsehellosir8273No ratings yet
- The Shoulder and Shoulder GirdleDocument43 pagesThe Shoulder and Shoulder GirdleMuhammad UsmanNo ratings yet
- Cervical Herniated Disc or Ruptured DiscDocument4 pagesCervical Herniated Disc or Ruptured DiscUwais AlNo ratings yet
- Shoulder PainDocument5 pagesShoulder Paindrraj07No ratings yet
- Lumbar Degenerative Disc DiseaseDocument13 pagesLumbar Degenerative Disc DiseasesanalcrazyNo ratings yet
- Frozen Shoulder 20 FebruaryDocument29 pagesFrozen Shoulder 20 Februaryangga nugrahaNo ratings yet
- Frozen Shoulder: By: Denise Dela CruzDocument44 pagesFrozen Shoulder: By: Denise Dela CruzDenise De la Cruz100% (1)
- Herniated Nucleus PulposusDocument17 pagesHerniated Nucleus PulposusCharmaine Joyce Fajardo RosquetaNo ratings yet
- Shoulder Assessment: Ayesha RazzaqDocument47 pagesShoulder Assessment: Ayesha Razzaqayesha100% (1)
- Physical Therapy Protocols For Conditions of Shoulder RegionDocument111 pagesPhysical Therapy Protocols For Conditions of Shoulder RegionPieng Napa100% (1)
- Physical Therapy For Sports Injuries (2012-2013)Document66 pagesPhysical Therapy For Sports Injuries (2012-2013)Mohammad EsmatNo ratings yet
- Frozen Shoulder (Revision)Document6 pagesFrozen Shoulder (Revision)Atet KurniadiNo ratings yet
- Frozen ShoulderDocument6 pagesFrozen ShoulderanumolNo ratings yet
- Shoulder PainDocument35 pagesShoulder PainAjayi FolamiNo ratings yet
- Physical Therapy in The Management of Frozen Shoulder: RticleDocument5 pagesPhysical Therapy in The Management of Frozen Shoulder: RticleYulianaNo ratings yet
- Sri Venkateshwara College of Pharmacy: Presented byDocument31 pagesSri Venkateshwara College of Pharmacy: Presented bySumavarsha Akavaram100% (1)
- Lumbar Herniated DiscDocument5 pagesLumbar Herniated DiscRinda AndreanditaNo ratings yet
- Sport Injuries: ShoulderDocument67 pagesSport Injuries: ShoulderNabiha AjmalNo ratings yet
- Herniated Nucleus PulposusDocument13 pagesHerniated Nucleus PulposusLorebell100% (4)
- Off-Campus Placement ProjectDocument4 pagesOff-Campus Placement Projectapi-488042467No ratings yet
- 4 Shoulder JointDocument50 pages4 Shoulder Jointq77gkyhzs4No ratings yet
- 43-44 - Muscuskeletal DisordersDocument39 pages43-44 - Muscuskeletal DisordersTaif SalimNo ratings yet
- 4 Common Musculoskeletal ProblemDocument54 pages4 Common Musculoskeletal ProblemMaria Lynne ParambitaNo ratings yet
- Pat Guide Frozen ShoulderDocument7 pagesPat Guide Frozen ShoulderMohammad TarmidziNo ratings yet
- Frozen Shoulder - Adhesive CapsulitisDocument8 pagesFrozen Shoulder - Adhesive CapsulitisfriskaNo ratings yet
- TendinitisDocument7 pagesTendinitisIceLeg SamUelNo ratings yet
- Lecture 5 Shoulder and Elbow Orthopedics-1Document52 pagesLecture 5 Shoulder and Elbow Orthopedics-1mukhtar abddi100% (1)
- Low Back Pain: Amir ShuhairiDocument69 pagesLow Back Pain: Amir ShuhairiHikaru99 otakuNo ratings yet
- Frozen ShoulderDocument110 pagesFrozen ShoulderAchmad ZulfikarNo ratings yet
- WEEK Orthopedics DR JohnDocument16 pagesWEEK Orthopedics DR JohnnoorgianilestariNo ratings yet
- Sprains and StrainsDocument23 pagesSprains and StrainsokaciaNo ratings yet
- PT Concept For Frozen ShoulderDocument27 pagesPT Concept For Frozen ShoulderBambang Ulan AeiyuNo ratings yet
- The Shoulder: M.K. SastryDocument37 pagesThe Shoulder: M.K. SastryGugus EkaNo ratings yet
- Physiotherapy Management of Secondary Impairments in Patients With StrokeDocument18 pagesPhysiotherapy Management of Secondary Impairments in Patients With StrokeBryan ChiamNo ratings yet
- Evaluare UmarDocument39 pagesEvaluare Umarcristian darabanNo ratings yet
- Frozen Shoulder: By: Kanchan SharmaDocument21 pagesFrozen Shoulder: By: Kanchan SharmaKanchan SharmaNo ratings yet
- Wry NeckDocument3 pagesWry NeckHasan RahmanNo ratings yet
- Frozen Shoulder ExercisesDocument7 pagesFrozen Shoulder ExercisesSumon PhysioNo ratings yet
- Lower Back SpondylosisDocument4 pagesLower Back SpondylosisDiduNo ratings yet
- Adhesive Capsulitis (Frozen Shoulder)Document5 pagesAdhesive Capsulitis (Frozen Shoulder)erikaNo ratings yet
- ICD-9-CM Codes: ICF Codes:: d4452 Reaching (Using The Hands and Arms To ExtendDocument13 pagesICD-9-CM Codes: ICF Codes:: d4452 Reaching (Using The Hands and Arms To ExtendAbdul Wahid ShaikhNo ratings yet
- Physiotheray Management of Shoulder DislocationDocument8 pagesPhysiotheray Management of Shoulder DislocationMonica StephenieNo ratings yet
- Rotator Cuff InjuryDocument29 pagesRotator Cuff InjuryArko duttaNo ratings yet
- HEINKING CounterstrainInAcuteInjuries ACOFPDocument60 pagesHEINKING CounterstrainInAcuteInjuries ACOFPRukaphuongNo ratings yet
- The Mindful Spine: A Holistic Approach to Healing Back PainFrom EverandThe Mindful Spine: A Holistic Approach to Healing Back PainNo ratings yet
- Rheumatoid ArthritisDocument4 pagesRheumatoid ArthritisFreeNursingNotes100% (1)
- Case 2Document19 pagesCase 2jagdish030798No ratings yet
- Space Infections PDFDocument98 pagesSpace Infections PDFRamya ReddyNo ratings yet
- Facial Fractures ClassificationDocument72 pagesFacial Fractures ClassificationAmar Mahesh KalluNo ratings yet
- Biziverse Template For LeadsDocument64 pagesBiziverse Template For LeadsKamal JindalNo ratings yet
- MSASDocument2 pagesMSASIvo_NichtNo ratings yet
- HIp & Knee Extremity Notes Sorgenfrey Gindl 7.16.10Document116 pagesHIp & Knee Extremity Notes Sorgenfrey Gindl 7.16.10joe joeNo ratings yet
- The Repertory Order of Synthesis-20211121Document11 pagesThe Repertory Order of Synthesis-20211121parents021No ratings yet
- 11-1. OsteoartritisDocument31 pages11-1. OsteoartritisZilhulaifaNo ratings yet
- Musculoskeletal Ultrasonography in Physical and ReDocument10 pagesMusculoskeletal Ultrasonography in Physical and ReHoussem BejaouiNo ratings yet
- Dental Equilibration and OsteopathyDocument9 pagesDental Equilibration and OsteopathyshivnairNo ratings yet
- Humerus Bone - Google Search PDFDocument1 pageHumerus Bone - Google Search PDFAngieBreidenbachNo ratings yet
- Anatomymnemonics PDFDocument28 pagesAnatomymnemonics PDFSenthilkumar ThiyagarajanNo ratings yet
- Bola Baling PrintDocument9 pagesBola Baling PrintLlna HnNo ratings yet
- Sanjeevini Combination Sheet For SSC 4 Back ProblemsDocument1 pageSanjeevini Combination Sheet For SSC 4 Back ProblemsEduardoNo ratings yet
- Handstand A Four Stage Training ModelDocument8 pagesHandstand A Four Stage Training ModelAllen ValseNo ratings yet
- Powerpoint - Normal Vs Abnormal Kinetic Chain AssessmentDocument29 pagesPowerpoint - Normal Vs Abnormal Kinetic Chain AssessmentmassagekevinNo ratings yet
- Full Download Principles of Athletic Training A Competency Based Approach Prentice 15th Edition Test Bank PDF Full ChapterDocument36 pagesFull Download Principles of Athletic Training A Competency Based Approach Prentice 15th Edition Test Bank PDF Full Chapterhalicore.icedlcbvp100% (20)
- T Bringing Classical and Contemporary Homoeopathy Ogether: ISSN: 9070-6038Document118 pagesT Bringing Classical and Contemporary Homoeopathy Ogether: ISSN: 9070-6038VarshaNo ratings yet
- 173 Anatomy SkeletalDocument23 pages173 Anatomy SkeletalSuryaNo ratings yet
- Therapy Therapy: Passive Movement Passive MovementDocument7 pagesTherapy Therapy: Passive Movement Passive MovementSIYAVUYA GCEBA100% (1)
- Postoperative Management and Rehabilitation inDocument3 pagesPostoperative Management and Rehabilitation invidyasagar pagilla100% (1)
- Chin Up KinesiologyDocument6 pagesChin Up KinesiologyMoffOmbasa100% (2)
- Artrodesis Revista EspañolaDocument9 pagesArtrodesis Revista EspañolaAlessandro MedinaNo ratings yet
- Practical Exam WorkDocument6 pagesPractical Exam WorkshinobieNo ratings yet
- Rehabilitation of Muscle Dysfunction in HemophiliaDocument14 pagesRehabilitation of Muscle Dysfunction in HemophiliadavidcorzoNo ratings yet
- CGMWDocument2 pagesCGMWpixol9339No ratings yet
- KCR Abstract Book - MusculoskeletalDocument19 pagesKCR Abstract Book - MusculoskeletalJANBADE PURVESH ATUL (PGP 2016-18)No ratings yet
- 01 Head and Neck JMDocument16 pages01 Head and Neck JMJowi SalNo ratings yet