Professional Documents
Culture Documents
Artigo 44 Mohamed2017 - Neuro
Artigo 44 Mohamed2017 - Neuro
Uploaded by
Lucas OliveiraCopyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Artigo 44 Mohamed2017 - Neuro
Artigo 44 Mohamed2017 - Neuro
Uploaded by
Lucas OliveiraCopyright:
Available Formats
MISS WARDA RAMADAN ABOUZEID MOHAMED (Orcid ID : 0000-0002-0117-3566)
Article type : Original Article
Accepted Article
The effectiveness of clinical pathway directed care on
hospitalisation-related outcomes in patients with severe
traumatic brain injury: a quasi-experimental study
Warda Ramadan Abouzeid Mohamed*, BN(Hons), MSN,
Visiting International Research (PhD) Student, University of South Australia, Australia;
Assistant Lecturer of Critical Care and Emergency Nursing, South Valley University, Egypt
E-mail: wardarr1199@gmail.com, ramwy002@mymail.unisa.edu.au, Phone: +201067027775
Matthew J Leach, RN, BN(Hons), ND, DipClinNutr, PhD
Senior Research Fellow, Department of Rural Health, University of South Australia, Australia
Email: Matthew.Leach@unisa.edu.au, Phone: +61 8 8302 2846
Nagwa Ahmad Reda, BN, MSN, PhD
Professor of Critical Care and Emergency Nursing, Alexandria University, Egypt
Email: nagwacc@hotmail.com Phone: +2 01001697687
Mohammad Mohamed Abd-Ellatif, BN, MSN, PhD
Professor of Anesthesia, Assiut University, Egypt
Email: Latif_mohamed@hotmail.com Phone: +2 01001745301
Mona Aly Mohammed, BN, MSN, PhD
Assist. Professor of Critical Care and Emergency Nursing, Assiut University, Egypt
Email: mona.ali77@yahoo.com Phone: +2 01226164645
Mervat Anwar Abdel Aziz, BN, MSN, PhD
Assist. Professor of Critical Care and Emergency Nursing, Assiut University, Egypt
Email: anwerabdelziz@yahoo.com Phone: +2 01062384501
*Corresponding author
Funding
The study was not supported by funding from any agency.
This article has been accepted for publication and undergone full peer review but has not
been through the copyediting, typesetting, pagination and proofreading process, which may
lead to differences between this version and the Version of Record. Please cite this article as
doi: 10.1111/jocn.14194
This article is protected by copyright. All rights reserved.
ABSTRACT
Accepted Article
Background: Severe traumatic brain injury (STBI) is a major cause of disability and
mortality in young adults. Clinical pathways endeavour to bring evidence and clinical
practice closer together to foster the delivery of best practice and to improve patient
outcomes.
Objective: To compare the effectiveness of clinical pathway directed care to usual care on
hospitalisation-related outcomes in patients with STBI.
Design: Quasi-experimental study.
Methods: The study was conducted in a trauma Intensive Care Unit of a large teaching
hospital in Egypt. Patients aged 18–60 years with a diagnosis of STBI, a Glasgow Coma
Scale score between 3 and 8 and a non-penetrating head injury, were consecutively assigned
to 15 days of care. The outcomes assessed were complications related to hospitalization,
clinical variances, length of ICU stay, ICU readmission rate, and patient/family satisfaction.
Results: Sixty participants completed the study (30 in each arm). Apart from age, there were
no significant differences between groups in baseline characteristics. The clinical pathway
group demonstrated statistically significantly fewer cases of hospitalisation-related
complications at day 15, and a significantly shorter length of ICU stay, lower ICU
readmission rate, and a high level of patient/family satisfaction when compared with the
usual care group. The effect of the intervention on fever, pressure ulceration, hyperglycaemia
and re-admission to the ICU was no longer statistically significant after controlling for age.
This article is protected by copyright. All rights reserved.
Conclusions: The findings of the current study suggest that the implementation of a clinical
pathway for patients with severe TBI may be helpful in improving the patient experience as
Accepted Article
well as some hospitalisation-related outcomes.
Relevance to clinical practice: The provision of clinical pathway directed care in a trauma
ICU may offer benefits to the patient, family and institution beyond that provided by usual
care
Key words: Care Pathways, Clinical Effectiveness, Evidence-Based Practice, Outcomes,
Patient Satisfaction, Severe traumatic brain Injury
What does this paper contribute to the wider global clinical community?
The study findings suggest that the provision of clinical pathway directed
care may improve hospitalisation-related outcomes in patients with severe
traumatic brain injury.
Clinical pathway directed care may also enhance the patient experience
through improvements in care processes, structures and outcomes.
INTRODUCTION
Traumatic brain injury (TBI) is defined as a physiological disruption of brain function and/or
structures caused by a strong impact or a bump to the head (Zasler et al. 2013). It is a leading
cause of morbidity, mortality and disability in young adults throughout the world (Benson,
2016). The management of STBI is complex and usually directed at reducing secondary
complications and maintaining adequate cerebral blood flow (Benson, 2016). Prevention of
these complications is critical to reducing the burden of head injury, although current practice
This article is protected by copyright. All rights reserved.
may not necessary reflect best practice (Kreipke & Rafols 2015). Clinical pathways provide
the means to connect the best available evidence with clinical practice; the intention of which
Accepted Article
is to foster the delivery of high quality care and to improve patient outcomes (Haddadsm
2010). Notwithstanding, there is little evidence to date to support this assumption. The study
described herein examines whether evidence-based, clinical pathway directed care is
effective in improving hospitalisation-related outcomes in persons with severe TBI when
compared with usual care.
BACKGROUND
The incidence of traumatic brain injury (TBI) is increasing worldwide; this increase is most
evident in developing countries where there is a significant rise in transport-related head
injuries (Frieden et al. 2015). In Africa, the majority of head and spinal injuries are related to
road traffic accidents. In Egypt in 2010, moderate and severe traumatic brain injury
accounted for 17.2% of all TBI presentations and males represented 79% of all patients
(Montaser & Hassan 2013). In Assiut University Hospital, approximately160 patients are
admitted to the trauma ICU with traumatic brain injury every year. Globally, the Centre for
Disease Control and Prevention estimate 2.5 million hospitalizations and deaths, annually,
are attributed to TBIs, either as an isolated condition or in combination with other injuries
(Frieden et al, 2015).
The World Health Organization (WHO) indicate that traffic accidents will represent the third
greatest cause of disease and injury burden in the world by the year 2020 (Maas et al. 2008)
and TBI will exceed chronic disease in terms of mortality and disability (Benson, 2016).
Adding to the burden of illness/injury is the relatively young age of persons affected by TBI,
This article is protected by copyright. All rights reserved.
with most cases likely to occur in children aged less than five years of age and adults aged
between 15–30 years (Roozenbeek et al. 2013)
Accepted Article
The consequences of TBI can be considerable, resulting in loss of consciousness, prolonged
immobilisation, hydrocephalus, skull fracture, cerebral spinal fluid leakage, and infections.
The residual effects of TBI are also significant, including seizures, cognitive impairment (e.g.
thinking, memory, and reasoning), mental heath or behavioural problems (e.g. aggression,
depression, personality changes, anxiety), and neurodegenerative disorders (e.g. dementia of
the Alzheimer's type and Parkinsonism) (Stocchetti & Zanier 2016).
The prolonged period of hospitalisation and immobilisation following the onset of TBI
contributes an additional risk of harm to the patient by promoting the development of
hospitalisation-related complications such as pressure ulceration, systemic or local infections,
hyperthermia, hyperglycaemia, hyper or hypotension and respiratory complications, in
addition to the complications related to head injury. Systemic complications post-traumatic
brain injury may be neurogenic in nature (e.g. the product of an intensecatecholamine, and
neuro-inflammatory response to injury), or an adverse effect of treatment (Rahul et al. 2008).
The presence of hospitalisation-related complications and TBI-related complications can
impact the prognosis of TBI, as can patient age, pertinent medical conditions, and prolonged
secondary brain insult (Zasler et al. 2013). Another factor contributing to the prognosis of
TBI is the severity of the condition. TBI can be classified as mild, moderate or severe; which
is determined by Glasgow Coma Scale (GCS) scoring. Approximately 10% of all head
trauma patients that are still alive on arrival at the emergency department have severe TBI
(Zasler et al. 2013). The presence of severe TBI has important implications in terms of
management and prognosis. For instance, it is predicted that 25% of all patients who have
severe TBI have neurological lesions that require neuro-surgical intervention (Rahul et al.
This article is protected by copyright. All rights reserved.
2008). Further, the mortality rate of adult patients with severe head injury is high, around
60%, and most survivors of severe TBI will suffer from severe disability. The effective
Accepted Article
management of TBI and the prevention of hospitalisation-related complications are therefore
critical to improving the prognosis of TBI.
The management of severe TBI is complex, challenging, and often necessitates a multimodal,
standardised approach. This approach generally includes circumspective hemodynamic
monitoring and support, fluid and electrolyte management, respiratory therapy, and other
aspects of care that focus on preventing secondary brain injury, improving cerebral
oxygenation and maintaining adequate cerebral perfusion pressure. The management of
severe TBI also requires collaboration across multiple disciplines, including the involvement
of critical care nurses, neuro-intensivists, neuro-surgeons, respiratory therapists, and other
medical specialties. Although the management of this condition can be challenging, involving
many different disciplines can lead to omissions in care, and duplicated services; this can
create inefficiencies in care and potentially increase the risk of harm to the patient
(Haddadsm 2010). The provision of high-quality, evidence-based care can be effective in
reducing variations in practice and improving patient outcomes (Howell, 2014). Clinical
pathways provide a means by which to synchronise the best available evidence with clinical
practice in order to facilitate the delivery of high quality care (Rotter et al. 2010).
Clinical pathways are multidisciplinary tools that provide explicit, best practice guidance on
the management of patients with particular diagnoses, or for particular procedures. Current
evidence indicates that the provision of clinical pathway directed care can contribute to
significant improvements in health outcomes, with a Canadian study demonstrating
significant improvement in hospitalization days, morbidity and mortality rate in nursing
home residents with pneumonia (Loeb et al. 2006). However, the evidence of the
effectiveness of clinical pathway directed care for the management of severe TBI is lacking,
This article is protected by copyright. All rights reserved.
and in terms of effectiveness in Middle Eastern populations and for hospitalisation-related
outcomes, the evidence is absent. In light of this, there is a need to determine whether clinical
Accepted Article
pathways are effective in improving the clinical outcomes of patients with severe TBI. The
current study aims to address this knowledge gap by comparing the effectiveness of clinical
pathway directed care to usual care in improving hospitalisation-related outcomes in adults
with STBI.
METHODOLOGY
Research design: The study adopted a quasi-experimental design; specifically, a
prospective, non-randomised, open-label, controlled trial design. The study comprised three
distinct phases, including: (1) development of a clinical pathway for severe TBI; (2) pilot
testing of the clinical pathway and study protocol; and (3) examination of the effectiveness of
a severe TBI clinical pathway versus usual care.
Aims and hypotheses: The study investigated whether the implementation of a clinical
pathway for patients with severe traumatic brain injury improves hospitalisation-related
outcomes when compared with usual care. To address this aim, the following hypotheses
were tested:
Primary hypotheses
Patients with STBI receiving clinical pathway directed care will:
1. Exhibit significantly fewer complications related to hospitalisation (e.g. hyperthermia,
pressure ulceration, infection, procedural pain and hyperglycaemia) than those receiving
usual care
2. Demonstrate less than 20% of clinical variances related to the prevention of
hospitalisation-related complications (e.g. DVT prophylaxis, pressure ulcer prevention).
This article is protected by copyright. All rights reserved.
Secondary hypotheses
Patients with STBI receiving clinical pathway directed care will:
Accepted Article
1. Exhibit a significantly shorter ICU length of stay than those receiving usual care
2. Demonstrate significantly fewer re-admissions to the ICU than those receiving usual
care
3. Demonstrate a significantly higher level of satisfaction with the care process, care
structure and care outcome than those receiving usual care.
Sample and setting: The pilot and main study were conducted at the Trauma Intensive Care
Unit (ICU) of the Main Assiut University Hospital, the largest teaching hospital in Assiut
City, Egypt. Participant inclusion criteria included: aged 18-60 years (this age group was
selected because it represented an adult population that is likely to require a similar approach
to TBI management), and Glasgow Coma Scale(GCS) score between 3 and 8 (a GCS within
this range is indicative of severe traumatic brain injury).
The sample size for the current study was based on an expected difference in primary
outcomes (i.e. complications and the clinical variances) of 40% between the intervention and
control group; this was based on data derived from the phase II pilot study. A sample size of
60 adult patients (i.e. 30 patients in each study arm) was expected to have 80% power to
detect a statistically significant difference in the primary and secondary outcomes (i.e.
complications, clinical variances, duration of MV, ICU stay and readmission) with a beta
level of 0.8 and a two-tailed alpha level set at 0.05.
Methods: Phase I of the study (i.e. the development of the STBI clinical pathway) began
with a critical review of the relevant literature. A comprehensive search of MEDLINE,
This article is protected by copyright. All rights reserved.
ProQuest, ScienceDirect, CINAHL and Google Scholar were undertaken to identify articles
that reported the evidence-based assessment, diagnosis and management of patients with
Accepted Article
severe traumatic brain injury. The search was restricted to articles published in the last ten
years (2004 to 2014) to ensure recency of evidence for phases II and III of the study. The
relevant literature was reviewed, along with theoretical frameworks describing the structure
and design of clinical pathways, as well as other pertinent clinical pathways (e.g. cardiac
pathways, wound care pathways), to develop a preliminary clinical pathway for severe TBI.
Five experts in the field of critical care and anaesthesiology examined and confirmed the face
and content validity of the clinical pathway.
The clinical pathway was a 15-page, double-sided, A4, paper-based document, which
comprised two instruments: the traumatic brain injury assessment checklist (containing four
parts) and the patient progress variances checklist (containing three parts). The traumatic
brain injury assessment checklist, which was designed to assess patients in both study groups,
gathered the following information: socio-demographic and health history, Glasgow Coma
Scale, injury severity scale, and clinical data. The patient progress variances checklist was
designed only for patients in the intervention group and provided guidance on daily
actions/tasks that could be performed to address each clinical objective. The variance
checklist, also recorded variations in care, that is, care that deviated from the clinical
pathway.
Pilot testing of the clinical pathway (phase II) was carried out between September 2014 and
October 2014. Six, consecutively selected, critically ill patients with severe TBI (assigned to
the intervention group only) were recruited (i.e. 10% of the total sample size required for the
phase III study). The purpose of phase II was to determine the feasibility of the study
protocol, clinical pathway and data collection instruments. The pilot study was similar in
every way to the main study, including the study setting, participant selection criteria,
This article is protected by copyright. All rights reserved.
duration of intervention (i.e. 15 days), and outcome measures used. Necessary revisions to
the clinical pathway and study protocol were made prior to commencing phase III (e.g. the
Accepted Article
main tools were originally designed to assess/manage patients over a seven-day period, but it
was the opinion of the experts to assess/manage patients over a fifteen-day period; experts
also recommended adding several additional actions/tasks to the pathway and omitting one
other).
Phase III of the study commenced in October 2014 and was completed by April 2015. All
persons presenting to emergency who met the study selection criteria were invited to
participate. Consenting participants were consecutively assigned by the researcher to usual
care or clinical pathway directed care between October and December 2014, and January and
April 2015, respectively. Participants assigned to usual care received 15 days of routine
nursing, medical and ancillary care in the trauma ICU of the hospital. Participants assigned to
the clinical pathway group received 15 days of care directed by a multidisciplinary clinical
pathway for severe TBI (noting that even though data collection ceased at 15 days, patients
continued to receive pathway-directed care after the trial to ensure continued access to best
practice care). The pathway required nursing, medical and ancillary staff to observe and
manage the patient across three phases; the admission phase (i.e. the first 24 hours), the acute
care phase (i.e. days two to eight) and mobility and weaning phase (i.e. days nine to fifteen).
The pathway was reviewed by staff on each shift (i.e. three shifts a day), and any variances to
the pathway or complications were reported. The researcher also provided health education
for the family members of participants in the intervention group on the second day of patient
admission; the education included a description of the care to be provided to the patient each
day, and information about the injury, complications, prognosis and care after discharge.
This article is protected by copyright. All rights reserved.
Outcomes: The main outcomes of the study are defined and operationalised below:
Accepted Article
- Complications related to hospitalisation, or adverse events, are an unintended harm
attributed to medical management or lack thereof. Complications were monitored and
recorded daily throughout the patients’ hospitalization period using the patient progress
variance checklist; this was documented by the researcher.
- Clinical care variances refer to the delivery of different levels of care amongst patients
with comparable demographic characteristics, diagnoses, and prognoses, despite the
presence of established and clearly documented evidence of best practice. Clinical
variances were measured across the following areas: assessment, diagnostic studies,
medications, intravenous solution, diet, activity, nursing care, consultation, health teaching
and discharge planning. These variances were measured by the researcher at each shift over
the fifteen-day of study period, using the patient progress variance checklist.
- Length of stay in ICU refers to the period of time the patient was situated within the ICU
(i.e. from the time the patient was admitted to the ICU, until their discharge from the unit).
The length of stay in the ICU was measured by the researcher at the end of the 15-day
study period by counting the number of the days information was recorded in the TBI
assessment checklist.
- Re-admission to ICU is defined as a second admission to the ICU within the same
hospitalization episode, for a diagnosis or problem similar or identical to the initial ICU
admission. Re-admission to the ICU was monitored by the researcher and recorded at the
end of the 15-day study period using the TBI assessment checklist.
- Patient/family satisfaction refers to the patient's/family's perceptions of the quality of the
health care service. Patients (if oriented) and/or family members in each study group were
interviewed by the researcher using the patient/family satisfaction tool before the end of the
study (day fourteen). Each interview lasted between 15 and 20 minutes.
This article is protected by copyright. All rights reserved.
Statistical analysis: All data cleaning and analyses were completed using IBM SPSS
Accepted Article
(version 20.0) software. Categorical variables were described using numbers and percentages.
Chi-square (χ2) tests were used to measure associations between categorical variables.
Continuous variables were described using means and standard deviations, with comparisons
made between continuous variables using either t-tests or Mann Whitney U tests. Continuous
variables were also tested for normal distribution using the Kolmogorov-Smirnov test and Q-
Q Plots. Where differences in demographic characteristics between groups were reported at
baseline, ANCOVA was used to test the statistical significance of the relationship between
the independent and dependent variables after controlling for the effects of the covariate(s).
The level of statistical significance for all tests was set at p<0.05.
Ethics: Written approval to conduct the current study was attained from the Assiut University
Hospital administrative authority. The study was also conducted in accordance with the
Assiut University Hospital Ethics Committees policy and the Declaration of Helsinki.
RESULTS
Demographic characteristics of the sample
Table 1 presents the demographic characteristics of the patients assigned to the intervention
and control groups. Participants in both groups were predominantly male and educated.
Participants in the intervention group were on average 10.7 years younger than those in the
control group, with the difference in mean age between groups found to be statistically
significant (p=0.001). There were also between-group differences in the marital status of
participants, with more patients in the intervention group being single (53.3%), and a greater
This article is protected by copyright. All rights reserved.
proportion of patients in the control group being married (63.3%); however, the difference
between groups was not statistically significant.
Accepted Article
Clinical characteristics of the sample
The event most likely to lead to TBI in both groups was a motor car accident, which
represented 49.9% of cases in the intervention group and 56.3% of cases in the control group.
Other events leading to TBI were motor bicycle accident (20% in the intervention group and
10% in the control group), falling from a height (20% and 6.7%), assault from another (6.6%
and 20%), firearm injury (3.3% and 0.0%) and a fall to the ground (0.0% and 6.7%). In terms
of past medical history, most patients (86.7% in the intervention group and 83.3% in the
control group) had no co-morbidities. By contrast, most patients (93.3% in the intervention
group and 86.6% in the control group) had poly-trauma on admission. The mean differences
of total injury severity score in intervention group were 19.3 while in control group were
18.5. Differences between groups in past medical history, presence of poly-trauma, type of
event leading to TBI and Injury Severity Score were not statistically significant
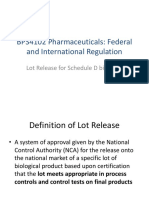
Frequency of complications related to hospitalisation
The frequency of complications related to hospitalisation reduced in both study groups over
time (Figure 1). Differences between groups in the occurrence of fever, pressure ulcers,
procedural pain (i.e. did not require lidocaine) and hyperglycaemia were statistically
significant (p=0.004, p=0.062, p=0.002 and p=0.022, respectively), with relatively fewer
cases of these complications reported in the intervention group. After controlling for age, the
intervention still had a significant effect on procedural pain (F [1,57] = 9.027, p = 0.004), but
not fever (F [1,57] = 2.717, p = 0.105), pressure ulcers (F [1,57] = 1.284, p = 0.262)
or hyperglycaemia (F [1,57] = 1.276, p = 0.263).There were no statistically significant
differences between groups in the occurrence of infection with fungi, gram-negative bacilli or
This article is protected by copyright. All rights reserved.
gram-negative cocci, deep venous thrombosis, vascular injuries or multiple organ system
failure.
Accepted Article
Overall variance
Variances to the clinical pathway that relate to the prevention of hospitalisation-related
complications are reported in Table 2 (for the intervention group only). Variances occurred
most frequently in areas relating to nursing care (i.e. use of circulating air-cooling blankets
[100%], air matrices [16.7%] and graduated stockings [13.3%], and meeting the 4-day
tracheostomy target [3.3%]) and professional consultations (i.e. rehabilitation consultation
[100%] and social worker consultation [100%]). No variances to the clinical pathway were
reported for patient/family health teaching. The most common reasons for the variations to
the clinical pathway were non-availability of services/equipment and action not applicable or
indicated.
Invasive devices duration
Table 3 outlines the differences in the frequency and duration of use of invasive devices
between study groups. The frequency of use of invasive devices was not significantly
different between groups for any device. Most invasive devices were in-situ for a relatively
shorter period of time in the intervention group than the control group; however, the only
statistically significant difference between groups was in the duration of central venous
catheter use (p=0.028).
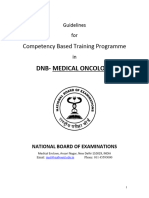
Length of ICU stay and re-admission to ICU
Length of stay in the intensive care unit (ICU) and number of re-admissions to the ICU are
illustrated in Figure 2. Differences between groups in mean length of ICU stay and mean
number of re-admissions to the ICU were statistically significant (p=0.007 & p=0.001,
respectively), with relatively smaller means reported in the intervention group. After
This article is protected by copyright. All rights reserved.
controlling for age, the intervention still had a significant effect on length of ICU stay
(F [1,55] = 7.341, p = 0.009), but not rate of re-admission to the ICU (F [1,57] = 0.213, p =
Accepted Article
0.646)."
Patient/family Satisfaction
In relation to the level of patient/family satisfaction with the care structure (Table 4), there
was a statistically significant difference between groups in areas relating to the hospital
environment (p=0.001), privacy (p=0.001), safety (p=0.004) and diet (p=0.001), with
relatively higher satisfaction scores reported in the intervention group across all four areas.
Patient/family satisfaction scores relating to care processes (i.e. respecting patient dignity,
maintaining social life, caring approach by nursing/medical/auxiliary teams and hospital
administration, and family education) and care outcomes (i.e. hospitalisation outcomes), are
presented in Table 5. There were no statistically significant differences between the
intervention and control groups in relation to the level of patient/family satisfaction with the
hospital administration processes. Differences between groups across all other process and
outcome areas were statistically significant (p=0.001), with relatively higher satisfaction
scores reported in the intervention group.
Table 6 illustrates the overall level of patient/family satisfaction with care (i.e. Care structure,
process and outcome) in the control and intervention groups. Chi-square analysis revealed a
statistically significant association between overall patient/family satisfaction and study
group (X2= 60.0, p< 0.001), with higher levels of satisfaction reported in the intervention
group.
This article is protected by copyright. All rights reserved.
DISCUSSION
Accepted Article
The utilisation of multidisciplinary clinical pathways for the management of various clinical
presentations has been associated with improvements in patient outcomes, adverse events and
health care costs (Santamaria et al. 2003). Notwithstanding, there has been very little research
to date examining the effectiveness of clinical pathways for patients with severe traumatic
brain injury (Harris et al. 2012). This is the first known study to examine the effectiveness of
clinical pathway directed care on hospitalisation-related outcomes in adults with STBI. The
study findings indicate that clinical pathways may offer patients and institutions some benefit
in terms of hospitalisation-related complications, length of ICU stay, ICU readmission rates,
and satisfaction with care, relative to usual care. The extent to which these findings might be
applicable to other patients with STBI requires a closer look at the study sample.
The sample
The study sample overall was predominantly young, male, married and educated. The higher
ratio of married and educated participants within this study could not be explained. The
higher ratio of males to females, and the young age of participants, is understandable
however, as this is typical of the general TBI population. This can be explained by the fact
that males are more prone to trauma during driving (the most common cause of head injury)
than females (Frieden et al. 2015); further, according to data from the Centers for Disease
Control and Prevention (Sahler & Greenwald 2012), head injury is most likely to occur in
males aged between 14 and 24 years.
The study sample was also reasonably homogenous in terms of clinical presentation, with
most participants presenting with a non-penetrating head injury secondary to a motorcar
accident, as well as poly-trauma, a GCS between 6 and 8, and the absence of any co-
This article is protected by copyright. All rights reserved.
morbidities. These characteristics are similar to the general head injury population in Egypt.
For instance, data from Farghaly et al (2007) indicate that 60% of patients admitted to Assiut
Accepted Article
hospital (Egypt) with head injury had sustained their injury from a road traffic accident, with
the highest incidence occurring in the age group of 20 to 29 years. Similarly, evidence from
the trauma audit and research network (TARN) showed that around 16% of trauma registry
patients (26,514 patients) between 1989–2007 had signs of poly-trauma; that is, significant
injuries to more than one body region (Pape et al. 2010). Unfortunately, there are insufficient
published data on typical GCS scores and the presence of pre-injury co-morbidities in
patients with severe traumatic brain injury. Notwithstanding, the sample of the current study
appeared to be generally representative of the head injury population in Egypt.
The only statistically significant difference observed between groups at baseline was the age
of participants. Participants in the intervention group were on average 10.7 years younger
than those in the control group. Whilst there is no obvious explanation for the difference in
age between groups, the difference is of clinical importance as older age has been shown to
have a negative impact on patient outcomes post-TBI (e.g. complications and mortality) (Røe
et al. 2013). The differences in the age of participants between groups could provide a
plausible alternate explanation for the improvements observed among participants in the
clinical pathway group for some, but not all, study outcomes, as discussed below.
Complications related to hospitalisation
The aim of this study was to determine whether the implementation of a clinical pathway
could improve the complications of hospitalisation among adults with STBI. The outcomes of
primary interest were hyperthermia, pressure ulceration, presence of procedural pain,
hyperglycaemia, infection, clinical variances related to the prevention of hospitalisation-
This article is protected by copyright. All rights reserved.
related complications, and ICU length of stay and re-admission rate. A discussion of the
findings relating to each of these outcomes now follows.
Accepted Article
Hyperthermia
There is a clear rationale for why body temperature must be controlled and pyrexia
aggressively managed in patients with severe TBI, with evidence suggesting that moderate
systemic hypothermia or normothermia can reduce cerebral metabolism, lower intracranial
pressure and raise cerebral perfusion pressure (Haddad & Arabi 2012). The current study
found statistically significantly fewer cases of fever in the intervention group than the control
group. This suggests that the implementation of the clinical pathway may have improved the
management of hyperthermia, possibly because the strategies outlined in the clinical pathway
were informed by the best available evidence. The use of antipyretic medication, cooling
blankets, ice packs, and cooled intravascular fluids as recommended in the pathway parallel
national and regional trends in fever and hyperthermia management as well as neuroscience
nurse decision-making, both nationally and regionally (Young & Saxena 2014).
Of course, many factors can impact body temperature, including environmental temperature.
For instance, during periods of persistent high ambient temperature, hyperthermia can arise in
critically ill infected patients and to a minor extent, in non-infected patients. In the current
study, the control group was conducted between summer and autumn, and the intervention
group conducted between winter and spring, thus exposing participants in the control group
to higher ambient temperature and potentially to an increased risk of elevated body
temperature. Whilst such an explanation is plausible, given the presence of air-conditioning
in the intensive care unit, it is unlikely that the timing of the study groups and subsequent
seasonal variations would have contributed much to the differences in this outcome between
study groups.
This article is protected by copyright. All rights reserved.
Pressure ulcers
Pressure ulcers are serious complications that commonly develop in individuals with severe
Accepted Article
traumatic brain injury (Dhandapani et al. 2014). Preventing pressure ulceration in
hospitalised patients is a clinical priority as the development of these wounds is associated
with a long list of negative patient and economic outcomes, including delayed enteral
feeding, fall in haemoglobin level, increased hospital length of stay (LOS), greater mortality
and health-care expenditure and decreased patient and family satisfaction with care
(Dickinson & Tschannen 2012). Findings from the current study revealed statistically
significant differences between groups in the occurrence of pressure ulcers, with no cases of
pressure ulceration reported in the intervention group compared to five reported cases in the
control group. It is probable that the application of the evidence-based pressure ulcer
prevention methods outlined in the STBI clinical pathway (e.g. changing patient position
every two hours, maintaining good body alignment, use of air mattresses, applying range of
motion exercises, massaging the lower limbs and back and sitting the patient out of bed)
contributed to these differences between groups, as the control group only received routine
hospital care (e.g. changing patient position every two hours and applying range of motion
exercises). It is also probable that the maintenance of adequate nutrition in the clinical
pathway group contributed to differences in the occurrence of pressure ulceration between
groups. This is because nutrition plays a central role in supporting tissue viability and the
preservation of skin integrity, both of which are critical to the prevention of pressure
ulceration and healing of existing ulcers (Kennerly et al. 2015).
Despite the aforementioned findings, the higher mean age of participants in the control group
could have played a part in the greater occurrence of pressure ulcers in this group, with
empirical evidence strongly supporting the relationship between advancing age and the
development of pressure ulcers in critical care patients. The results of ANVOVA certainly
This article is protected by copyright. All rights reserved.
suggest that the effect of the intervention on pressure ulcer occurrence was clearly modified
by age. Notwithstanding, the degree to which age contributed to the difference in pressure
Accepted Article
ulcer occurrence between groups is questionable as the control group was still relatively
young (i.e. 39 years), with studies indicating that pressure ulcers typically develop in much
older patients (i.e. 73 years) (Cox, 2011).
Use of lidocaine and presence of pain
Critically ill adult patients often experience considerable pain during hospitalisation, with
more than 30% of ICU patients reporting substantial pain at rest, and over 50% experiencing
marked pain during usual care, including endotracheal suctioning, repositioning, and wound
management (Puntillo et al. 2014). Lidocaineis widely used to reduce procedural pain, such
as endotracheal or nasogastric tube insertion. Evidence from a prospective study of nineteen
patients in a medical ICU in Taipei, Taiwan (Lee et al. 2012) lends some support to this
practice, concluding that lidocaine spray is effective in reducing pain caused by endotracheal
tube insertion.
The findings of the current study concur with the results of the aforementioned study (Lee et
al. 2012), revealing significantly fewer cases of procedural pain in the intervention group
than the control group. This may be because the clinical pathway encouraged nursing and
medical staff to deliver best practice care around minimising the occurrence of procedural
pain. However, given that the intervention and control group were administered at different
points in time, other factors influencing the occurrence of pain cannot be dismissed, such as
the variability in techniques provided by different nursing and medical personnel. It was
certainly the case in the current study that the nursing and medical staff present during the
control phase and intervention phase were different; this is mainly due to the level of staff
turnover (including medical staff rotations) observed over the seven-month study period. A
This article is protected by copyright. All rights reserved.
retrospective study of critically ill intubated patients has shown that such variations in
staffing can lead to differences in the level of pain experienced during procedures (Gélinas et
Accepted Article
al. 2004).
Hyperglycaemia
The acute sympathoadrenomedullary response following trauma is characterised by elevated
catecholamine levels, which predisposes patients with severe traumatic brain injury to
hyperglycaemia. Hyperglycaemia is also positively correlated with infection, the need for
intensive care, hospital length of stay, and mortality (Salim et al. 2009). As such, the
effective management of hyperglycaemia should not be overlooked in the overall
management of severe TBI in the ICU.
In the current study, participants receiving care guided by the TBI clinical pathway
demonstrated significantly fewer cases of hyperglycaemia than participants receiving usual
care. This may be because the strategies outlined in the clinical pathway were informed by
the best available evidence (e.g. administration of intensive insulin therapy for serum glucose
levels exceeding than 120 mg/dl) (Salim et al.2009). This is supported by findings from a
prospective observational study of 100 patients hospitalized in an Eastern European medical
intensive care unit. The study found protocol-directed intensive monitoring and insulin
therapy to be effective in the treatment of hyperglycaemia in critically ill patients (Godinjak
et al. 2015). It is also possible that the improvement in blood glucose levels in the
intervention group may have been mediated by age (as shown by ANCOVA), with evidence
from cross-sectional studies indicating that plasma glucose levels rise with increasing age in
non-diabetic adults (Ko et al. 2006).
This article is protected by copyright. All rights reserved.
Infection
Patients with severe traumatic brain injury are particularly prone to developing infections and
Accepted Article
sepsis because clinical symptoms and conventional markers are not always reliable indicators
of infection in this patient group. Adding to this, patients with Glasgow Coma Scale scores
less than nine (as is the case in severe TBI) have relatively higher rates of upper airway
microbial colonisation (Feasal et al. 2015), possible attributed to the aspiration of high
inoculum oropharyngeal secretions immediately following brain injury, during resuscitation,
and as a result of intubation. The presence of long-term invasive devices such as urinary
catheters or intravenous cannulae compounds this risk (McClelland & Moxon, 2014)
The findings of the current study revealed no significant differences between study groups in
terms of the occurrence of infection with fungi, gram-negative bacilli or gram-negative cocci;
however, there were fifty-five percent fewer cases of infection reported in the clinical
pathway group. The lower infection rate in the intervention group may be related to the
relatively fewer risk factors for infection observed in this group, such as reduced number of
days with invasive devices in-situ, decreased incidence of pressure ulceration and greater
adherence infection control practices. This is supported by findings from a meta-analysis of
twenty-two studies examining the effectiveness of clinical pathway directed care for hip and
knee joint replacement. The analysis revealed significantly fewer reports of postoperative
complications, including superficial and deep infections, among patients receiving clinical
pathway care when compared with standard care (Barbieri et al. 2009).
Overall variances
Reports from Australia and overseas suggest that deviations in clinical practice are not
atypical even where approved clinical practice guidelines are available. Unnecessary
variations that are unable to be attributed to disease severity or patient factors are common,
This article is protected by copyright. All rights reserved.
and clinical practice is often idiosyncratic and unscientific (Kennedy et al 2010). Clinical
pathways aim to reduce such inconsistencies in clinical practice and to facilitate the delivery
Accepted Article
of evidence-based practice.
The findings of the current study suggest that the clinical pathway for severe traumatic brain
injury may have fostered the uptake of best practice, with few variances to the evidence-
based clinical pathway reported. It is also possible that because of the nature of the study
design, and that variances were not (understandably) measured in the control group, that
nursing, medical and ancillary staff may have already been delivering best practice care. The
limitation of the current study highlights the need for future clinical pathway studies to more
closely monitor clinical practice in control groups to determine the extent to which clinical
pathways may impact the delivery of best practice care.
Variances occurred in the intervention group most frequently in areas relating to nursing care.
The most common reasons for the variations to the clinical pathway were non-availability of
services/equipment and actions not applicable or indicated. Most studies agree that
insufficient funds and decreased availability of equipment and resources can affect the
delivery of services to patients in hospitals, adversely affecting perceptions of health service
quality, patient satisfaction and patient loyalty (Wanjau et al. 2012). These findings suggest
that if sufficient resources and services were available to nurses, adherence to the clinical
pathway, and thus best practice, may have been greater. Notwithstanding, there are multiple
and diverse reasons for variations in clinical practice (Kennedy et al 2010), thus the provision
of necessary services/equipment may only partially address variations to a clinical pathway.
Understanding how other factors contribute to such variations in clinical pathways should be
the focus of future research.
This article is protected by copyright. All rights reserved.
Invasive devices duration
Invasive medical devices play an essential role in the monitoring and management of
Accepted Article
critically ill patients. However, the presence of an indwelling invasive device is a recognised
risk factor for healthcare-associated infection (HAIs), such as ventilator-associated
pneumonia, central venous catheter related bloodstream infections and catheter-associated
urinary tract infections (Loveday et al. 2014). Hence, the early removal of invasive medical
devices is an important strategy in reducing infection risk in hospitalised patients (Evik et al.
2013).
The current study found invasive devices to be in-situ for a relatively shorter period of time in
the intervention group than the control group. This suggests that there was greater adherence
to best practice in the intervention group, possibly translating to a lower risk of harm from
invasive device-associated hospital infection among participants in this group. The impact of
clinical pathways on infection rates also has been demonstrated by Walker et al. (2012), who
showed the introduction of a bronchiolitis clinical care pathway to be effective in reducing
the proportion of infants with infection as well as the use of prescribed salbutamol. In a
systematic review and meta-analysis of the effects of clinical pathways on patient outcomes,
hospital costs and length of stay, Rotter et al, (2008) revealed a significant reduction in the
duration of invasive devices. Both of these studies corroborate the findings of the current
study, thus supporting the value of clinical pathways in reducing healthcare associated
infection.
Length of stay and re-admission
Many clinical studies on traumatic brain injury have used length of stay (LOS) as a health
care performance indicator, with many using pre-defined LOS as an “economic” outcome
and a suitable surrogate for hospital expenditure (Lazaridis et al. 2015). The current study
This article is protected by copyright. All rights reserved.
indicates that clinical pathway directed care may influence the duration of hospitalization, but
possibly not ICU re-admission rate, with patients in the pathway group demonstrating
Accepted Article
significantly shorter lengths of stay in the ICU than patients in the control group. These
findings may be attributed to a number of factors, such as the shorter duration of mechanical
ventilation, meeting the 4-day tracheostomy target (Hosokawa et al. 2015), earlier
mobilization, earlier return of oral intake, and the education of hospital healthcare providers
in the intervention group. The findings of this study corroborate the results of other studies,
which have shown clinical pathways to be effective in reducing the number of hospitalisation
days, health care costs and mortality rates in persons with pneumonia, lower respiratory tract
infection and heart failure (Loeb et al. 2006). These findings highlight the potential economic
benefit of implementing clinical pathways in STBI; an important focus of further research in
this area would be to examine the cost-benefit of implementing clinical pathways in STBI.
Patients/Family Satisfaction
While patient satisfaction is regarded as one of the most desired outcomes of care, and is a
key domain of quality care, the assessment of patient satisfaction in the critical care
environment is somewhat complicated. Patients in the critical care setting are typically not
able to make decisions about their care because of the level of consciousness or severity of
illness (Stricker et al. 2007). Likewise, patients in this setting are often too ill to ascertain the
level of satisfaction with care or may not even recall the critical care experience;
consequently, patient satisfaction surveys may not be an adequate measure of satisfaction in
the critical care environment. Instead, family members are frequently the ones to establish a
patient’s satisfaction with care, as well as the patient’s overall critical care experience. In
other words, satisfaction may be measured by the family member's perception of care
delivered rather than the actual care received (Roberti & Fitzpatrick 2010).
This article is protected by copyright. All rights reserved.
In the current study, there was a statistically significant difference between groups in
perception of care structure, with relatively higher satisfaction levels reported in the clinical
Accepted Article
pathway group across areas relating to the hospital environment, privacy, safety and diet.
Differences between groups across care processes and care outcomes were statistically
significant, with relatively higher satisfaction scores reported in the intervention group.
However, there was no statistically significant difference found between the intervention and
control groups in regards to satisfaction with hospital administration.
The significant improvements in patient/family satisfaction across multiple aspects of care
correlates with the findings of other clinical pathway research (Neves et al 2009). In an
earlier review of 200 studies evaluating the effectiveness of clinical pathways (Van Herck et
al. 2004), 66% of the included studies reported a positive effect on clinical pathway
outcomes, with 62% reporting a positive effect on patient satisfaction. Similarly, Hassan et al.
(2014) had shown that the implementation of a diabetic ketoacidosis (DKA) clinical pathway
had empowered clinicians to deliver evidence-base practice, which in turn, resulted in the
provision of better patient care. These findings suggest that clinical pathways may foster a
positive patient experience not only by improving the safety and quality of patient care, but
by enhancing patient, family and clinician education and communication.
Limitations
There are several limitations to this study that may affect the interpretation and
generalizability of the findings. The most notable limitation of the current study was the
study design. The collection of data for each of the two groups occurred at different time
points, which may have increased the risk of chronology bias (Paradis, 2008). Further,
without participant/family and clinician blinding, we cannot exclude the possibility that
expectation bias impacted the results. It is also possible that the absence of randomization
This article is protected by copyright. All rights reserved.
may have increased the risk of selection bias. However, given that the two study groups were
similar across all clinical variables and demographic variables (except for age), the likelihood
Accepted Article
of selection bias is very small. Nevertheless, patients in the intervention group were on
average ten years younger than those in the control group; this difference is of clinical
importance as older age has been shown to have a negative impact on patient outcomes post-
TBI (Dhandapani et al. 2012).
CONCLUSIONS AND RECOMMENDATIONS
Severe traumatic brain injury can lead to considerable morbidity and disability, even death, if
not promptly diagnosed and treated. The findings of the present study suggest that the
implementation of clinical pathway directed care for adults with STBI may be useful in
improving procedural pain, the patient experience, and potentially, decreasing health care
expenditure (via reductions in ICU length of stay). Further research is needed to determine
whether these findings can be reproduced in persons of different age groups (i.e. older adults
and children), in different settings, and over longer periods of time. Such research should also
consider the economic impact of using clinical pathways for STBI.
ACKNOWLEDGMENTS
We would like to thank the Assiut University Hospital Trauma ICU, Egypt, for their support
with participate recruitment and data collection. We would also like to thank the study
participants for their involvement in the study.
FUNDING
The study was not supported by funding from any agency.
This article is protected by copyright. All rights reserved.
REFERENCES
Accepted Article
Barbieri A, Vanhaecht K, Herck P, Sermeus W, Faggiano F, Marchisio S, & Panella M
(2009) Effects of clinical pathways in the joint replacement: a meta-analysis.
BMC Medicine Journal, 7, 32. doi: DOI: 10.1186/1741-7015-7-32.
Benson K (2016) Traumatic Brain Injury in Kenya: A Preliminary Review of the
Literature. SAGE Open, 1–7.
Cox J (2011) Predictors of pressure ulcers in adult critical care patients. American
Association of Critical-Care Nurses 20 (5), 364-374.
Dhandapani M, Dhandapani S, Agarwal M & Mahapatra A (2014) Pressure ulcer in
patients with severe traumatic brain injury: significant factors and association
with neurological outcome . Journal of Clinical Nursing 23, 1114–1119.
Dhandapani S, Manju D & Mahapatra A (2012) Prognostic significance of age in
traumatic brain injury. Journal of Neuroscience in Rural Practice 3(2), 131-135.
doi: doi: 10.4103/0976-3147.98208.
Dickinson S & Tschannen D (2012) Can the Use of an Early Mobility Program Reduce the
Incidence of Pressure Ulcers in a Surgical Critical Care Unit?. Critical Care
Nursing Quarterly 36 (1), 127-140.
EvikS, Bosnak V, NamiduruM, Karaoglan İ & Ozlem M (2013) Invasive device-associated
hospital infection rates, etiological agents, and their antibiotic susceptibilities in
the medical intensive care unit of a university hospital in Turkey. Turkish Journal
of Medical Sciences, 43, 33-38.
Farghaly A, El-KhayatR, Awad W, & George S (2007) Head Injuries in Road Traffic
Accidents. Faculty of Medicine, Asyut University, Egypt.
Feasal A, El Azab A, Mashhour K & El Hadidy A (2015) Impact of body temperature and
serum procalcitonin on the outcomes of critically ill neurological patients. The
Egyptian Journal of Critical Care Medicine, 3, 18.
Finally A (2015) The link between diabetic and body temperature. New life outlook.
from http://dm2.newlifeoutlook.com/body-temperature-and-type-2-diabetes/
Frieden T, Houry D, & Baldwin G (2015) Traumatic brain injury in United States:
epidemiology and rehabilitation. United States: Centre for Disease Control and
Prevention (CDC).
Gélinas C, Fortier M, Viens C, FillionL & Puntillo K (2004) Pain assessment and
management in critically ill intubated patients: A retrospective study. American
Journal of Critical Care 13, 126-135.
Godinjak A, Iglica A, Burekovic A, Jusufovic S, Ajanovic A, Tancica I & Kukuljac A (2015)
Hyperglycemia in Critically Ill Patients: Management and Prognosis. Medical
Arhives Journal, 69 (3), 157-160.
Haddad S & Arabi Y (2012) Critical care management of severe traumatic brain injury in
adults. Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine,
20, 12.
Haddadsm M (2010) Clinical pathways: effects on professional practice, patient
outcomes, length of stay and hospital costs: RHL commentary. TheWorld Health
Organization Reproductive Health Library; Geneva: World Health Organization.
Harris T, Rhys T & Brohi K (2012) Early fluid resuscitation in severe trauma. Britich
Medical Journal, 345: e5752.
This article is protected by copyright. All rights reserved.
Hassan I, Al-Otaibi A, Al-Bugami M, Bin Salih S, Al Saleh Y, and Abdulaziz S. (2014). The
Impact of a Structured Clinical Pathway on the Application of Management Standards
in Patients with Diabetic Ketoacidosis and Its Acceptability by Medical Residents.
Journal of Diabetes Mellitus; 4, 264-272.
Accepted Article
Hosokawa K, Nishimura M, Egi M & Vincent JL. (2015) Timing of tracheotomy in ICU
patients: a systematic review of randomized controlled trials. BMC Crit Care. 19:
424.
Howell S. (2014). Advances in trauma care: a quiet revolution. British Journal of
Anaesthesia,113 (2): 202–6.
Kennedy P, Leathley C & Hughes C (2010) Clinical practice variation. Medical Journal of
Australia, 193(8), s97-s99.
Kennerly S, Batchelor-Murphy S & Yap T (2015) Clinical insights: Understanding the
link between nutrition and pressure ulcer prevention. Geriatric Nursing, 36, 477-
481.
Ko GTC, Wai HPS, Tang JSF. (2006) Effects of Age on Plasma Glucose Levels in Non-
diabetic Hong Kong Chinese. Croat Med J; 47(5): 709–713.
Kreipke C & Rafols J (2015)Cerebral Blood Flow, Metabolism and Head Trauma (pp. 1-
12).
Lazaridis C, YangM, DeSantis S, LuoS & RobertsonC (2015) Predictors of intensive care
unit length of stay and intracranial pressure in severe traumatic brain injury.
Journal of Critical Care, 30, 1258-1262.
LeeS, Wu C, Kuo L, Lai C, Hsu C, Hwung H, Chen Y, Ho Y, Hsu H , Sun F, et al. (2012) The
Effects of Xylocaine Spray for Pain Control Caused by Endotracheal Tube in
Critical Care. International Journal of Gerontology, 6, 11-15.
Loeb M, Carusone S, Goeree R, et al (2006) Effect of a clinical pathway to reduce
hospitalizations in nursing home residents with pneumonia: a randomized
controlled trial. Journal of the American Medical Association, 295 (21), 2503-
2510. DOI:10.1001/jama.295.21.2503
Loveday H, Wilson J, Pratt R, Golsorkhi M, Tingle A, et al (2014) National Evidence-
based Guidelines For Preventing Healthcare Associated Infections in NHS
hospitals in England.Department of Health EPIC 3. Journal of Hospital Infection.
86S1, s1-70.
Maas A, Stocchetti N & Bullock R (2008) Moderate and severe traumatic brain injury in
adults. Lancet Neurol, 7, 728–741
McClelland H & Moxon A (2014) Early identification and treatment of sepsis. Nursing
Times, 110 (4), 14-17.
Montaser T & Hassan s (2013) Epidemiology of moderate and severe traumatic brain
injury in Cairo University Hospital in 2010. Critical Care, 17(2).
Neves F, Dantas M, Bitencourt A, Vieira P, Magalhaes L, Teles J et al. (2009). Analysis of
family satisfaction in intensive care unit. Rev Bras Ter Intensiva. 21(1):32-37.
Pape H, Peitzman A, Schwab C & Giannoudis P (2010) Damage Control Management in
the Polytrauma Patient. DOI: 10.1007/978-0-387-895086.
ParadisC (2008) Bias in Surgical Research. Annals of Surgery, 248, 180-188. Pinkerman
C, Sander P, BreedingJ, Brink D, Curtis R, Hayes R, OjhaA, Pandita D, RaikarS,
Setterlund L, Sule O & Turner A (2013) Heart Failure in Adults. Institute for
Clinical Systems Improvement
https://http://www.icsi.org/_asset/50qb52/heartfailure.pdf
This article is protected by copyright. All rights reserved.
Puntillo K, Max A, Timsit J, Vignoud L, Chanques G & Robleda G (2014) Determinants of
Procedural Pain Intensity in the Intensive Care Unit TheEuropain (R) Study.
American Journal of Respiratory and Critical Care Medicine, 189(1), 39-47.
Rahul B, Korin H& Tina S. (2008). An Evidence-Based Approach to Severe Traumatic
Accepted Article
Brain Injury. Emergency Medicine Practice j. 10 (12):1-24
Roberti S & Fitzpatrick J (2010) Assessing family satisfaction with care of critically ill
patients: A pilot study. Critical Care Nurse, 30(6), 18-26.
Røe C, Skandsen T, Anke A, Ader T, VikA, Lund S, Manskow U, Sollid S et al (2013)
Severe traumatic brain injury in Norway: impact of age on outcome. Journal of
Rehabilitation Medicine, 45, 734–740.
Roozenbeek B, Maas A & Menon D (2013) Changing patterns in the epidemiology of
traumatic brain injury. Nature Reviews Neurology, 9, 231–236
doi:10.1038/nrneurol.2013.22
Rotter L, James EL, Machotta A, Gothe H, Willis J, Snow P & Kugler J (2010) Clinical
pathways: effects on professional practice, patient outcomes, length of stay and
hospital costs. The Cochrane library, 7, 1-166.
Rotter T, Kugler J, Koch R, Gothe H, Twork S, et al (2008) A systematic review and meta-
analysis of the effects of clinical pathways on length of stay, hospital costs and
patient outcomes. BMC Health Services Research, 8, 265.
Sahler C & Greenwald B (2012) Traumatic Brain Injury in Sports: A Review. .
Rehabilitation Research and Practice, 2012, 1-10.
Salim A, Hadjizacharia P, Dubose J, Brown C, Inaba K, Chan L & Margulies D(2009)
Persistent hyperglycemia in severe traumatic brain injury: an independent
predictor of outcome. American Surgeon 75, 25-29.
Santamaria N, Houghton L, Kimmel L & Graham A (2003) Clinical pathways for
fractured neck of femur: A cohort study of health related quality of life, patients
satisfaction and clinical outcome. Australian Journal of Advanced Nursing, 20 (3),
24-29.
Stocchetti N & Zanier E (2016) Chronic impact of traumatic brain injury on outcome and
quality of life: a narrative review. Critical Care, 20.
Stricker K, Niemann S, BugnonS, Wurz J, Rohrer O & Rothen H (2007) Family
satisfaction in the intensive care unit: cross-cultural adaptation of a
questionnaire. Journal of Critical Care, 22(3), 201-211.
Van Herck P, Vanhaecht K and Sermeus W (2004). Effects of Clinical Pathways: do they
work?. Journal of Integrated Care Pathways, 8, 95-105
WalkerC, Danby S & Turner S (2012) Impact of a bronchiolitis clinical care pathway on
treatment and hospital stay.European Journal of Pediatrics, 171(5), 827–832.
Wanjau K, Muiruri B & Ayodo E (2012) Factors Affecting Provision of Service Quality in
the Public Health Sector: A Case of Kenyatta National Hospital. International
Journal of Humanities and Social Science, 2(13), 114-125.
Young P & Saxena M (2014) Fever management in intensive care patients with
Infections. Critical Care, 18, 206.
Zasler D, Arciniegas B, Jaffee S & Vanderploeg D (2013) Management of Adults with
Traumatic Brain Injury. American Psychiatric Publishing, 6-8.
This article is protected by copyright. All rights reserved.
Tables and Figures
Table 1: Demographic characteristics of participants by study group
Accepted Article
Intervention Control P value
Age (year), mean + SD 29.0+10.2 39.7+13.7 0.001
Gender, n (%)
Male 28 (93.3) 26 (86.7)
0.389
Female 2 (6.7) 4(13.3)
Marital status, n (%)
Single 16 (53.3) 10 (33.3)
Married 14 (46.7) 19 (63.3) 0.208
Divorce 0(0.0) 1 (3.3)
Level of education, n (%)
Educated 28 (93.3) 26 (86.7)
0.389
Illiterate 2(6.7) 4(13.3)
27 **
24
21
18
15 * **
Number of patients
12
9 Intervention
*
6
3 0 Control
0
Complications related hospitalization
**significance at p< 0.005, * significance at p < 0.05
Figure 1: Frequency of complications related to hospitalisation by study group
This article is protected by copyright. All rights reserved.
Table 2: Occurrence of variances to the clinical pathway in the intervention group
Accepted Article
Intervention
Variance Reasons for variance
n (%)
Related to nursing care
Did not use of Cervical collar Not applicable 30 (100.0)
Did not use circulating air cooling Not available 30 (100.0)
blanket
Did not use air matrices Not available 5 (16.7)
Did not remove endotracheal tube Not required 1(3.3)
by day 4
Did not use graduated stocking Not available 4(13.3)
Related to activity
Did not move Patient on chair Condition of the patients not 5(16.7)
allowed
Related to medication
Did not use low molecular weight Not required 3 (10.0)
heparin
Did not give Midazolam Not required 6 (20)
Did not administer of vasopressor as Not required 5(16.7)
ordered
Related to diet / nutrition
Did not start oral feeding Condition of the patient not 4 (13.3)
allowed
Related to diagnostic studies
Did not monitor ECG Not required 4 (13.3)
Related to IV fluids
Did not use Blood product Not required 6 (20)
Related to consultation
Did not consult rehabilitation Not available 30 (100.0)
consultant
Did not consult social worker Not available 30 (100.0)
Related to health teaching and discharge planning
Did not deliver health teaching No variance 0.0(0.0)
Did not complete discharge planning Patients still in the ICU 4 (13.3)
This article is protected by copyright. All rights reserved.
Table 3: Frequency and duration of use of invasive devices by study group
Invasive devices Number of patient's Duration insitu (days)
Intervention, Control, Intervention, Control, Mean difference
Accepted Article
P value P value
n (%) n (%) mean + SD mean + SD (95% CI)
Endotracheal tube -0.8
30 (100) 29 (96.7) 0.313 3.9+1.4 4.7+2.4 0.096
(-1.87,0.16)
Tracheostomy -0.6
9 (30) 7 (23.3) 0.770 4.5+1.2 5.1+1.1 0.295
(-1.92,0.63)
Central venous -1.6
30 (100) 29 (96.7) 0.313 12.1+3 13.7+2.5 0.028
catheter (-3.1,-0.18
Chest tube -2.2
17(56.7) 22 (73.3) 0.176 5.2+5 7.4+4.7 0.093
(-4.64,0.37)
Peripheral catheter 0.2
30 (100) 29 (96.7) 0.313 14.1+1.2 13.9+2.9 0.648
(-0.90,1.43)
Urinary catheter -0.6
30 (100) 29 (96.7) 0.313 14.1+1.5 14.7+1.2 0.104
(-1.3,0.13)
Nasogastric tube -5.3
30 (100) 29 (96.7) 0.313 12.1+2.9 17.4+20.2 0.091
(-12.78,2.15)
18
16 **
14
12
10
Mean
**
8
Intervention
6
Control
4
2
0
LOS in ICU Readmission to ICU
LOS= length of stay, ICU= Intensive care unit, ** significance at p< 0.005
Figure 2: Length of ICU stay and readmission to ICU, by study group
This article is protected by copyright. All rights reserved.
Table 4: Patient / family satisfaction with the care structure, by study group
Mean
Satisfaction with Intervention Control difference T value
Accepted Article
Cohen’s d P value
care structure (95% CI)
Mean+ SD Mean+ SD
a 1.1
Environment 20 + 1.1 18.9 + 0.3 1.36 5.02 0.001
(0.69,1.52)
b 1.5
Safety 19.1 + 1.6 17.6 + 2.1 0.80 3.05 0.004
(0.5,2.4)
c 2.0
Diet 9.9 + 0.5 7.9 + 1.0 2.53 9.71 0.001
(1.59,2.4)
d 0.7
Privacy 6.9 + 0.9 6.2 + 0.4 1.01 3.70 0.001
(0.31,1.03)
a
Environment satisfaction: 7 questions; scoring: rarely (1), sometimes (2) & always (3); maximum score = 21
b
Safety satisfaction: 8 questions; scoring: rarely (1), sometimes (2) & always (3); maximum score = 24
c
Diet satisfaction: 4 questions; scoring: rarely (1), sometimes (2) & always (3); maximum score = 12
d
Privacy satisfaction: 4 questions; scoring: rarely (1), sometimes (2) & always (3); maximum score = 12
Table 5: Patient / family satisfaction with care process and outcome, by study group
Mean
Satisfaction with care Intervention Control Cohen’s
difference T value P value
process & outcome d
Mean+ SD Mean+ SD (95% CI)
a 6.2
Hospitalisation outcome 19.1+ 0.9 12.9+ 1.0 6.52 21.82 0.001
(6.16,6.89)
b 5.5
Respect dignity 18.3 + 0.9 12.8 + 1.0 5.78 21.80 0.001
(4.9,5.9)
c 3.7
Caring by auxiliary team 17.0 + 1.5 13.3 + 1.6 2.39 14.30 0.001
(3.12,4.01)
d -0.6
Hospital administration 14.1 + 1.5 14.7 + 1.2 0.44 14.33 0.104
(-1.9,0.63)
e 4.5
Education 9.6 + 1.4 5.1 + 0.3 4.45 6.87 0.001
(4.1,5.04)
f 2.6
Caring by nursing team 8.5 + 0.7 5.9 + 1.1 2.82 19.41 0.001
(1.58,2.42)
g 1.5
Caring by medical team 8.4 + 0.7 6.9 + 1.0 1.74 16.07 0.001
(0.91,1.88)
h 1.4
Maintain social life 7.5 + 1.3 6.1 + 0.3 1.48 5.76 0.001
(0.92,1.88)
a
Hospitalization outcome: 7 questions; scoring: rarely (1), sometimes (2) & always (3); maximum score =21.
b
Respect dignity: 7 questions; scoring: rarely (1), sometimes (2) & always (3); maximum score =21.
c
Caring by auxiliary team: 7 questions; scoring: weak (1), good (2) &excellent (3); maximum score =21.
d
Hospital administration: 3 questions; scoring: weak (1), good (2) &excellent (3); maximum score =9.
e
Education: 5 questions; scoring: rarely (1), sometimes (2) & always (3); maximum score =15.
f
Caring by nursing team: 3 questions; scoring: weak (1), good (2) &excellent (3); maximum score =9.
g
Caring by medical team: 3 questions; scoring: weak (1), good (2) &excellent (3); maximum score =9.
h
Maintain social life: 5 questions; scoring: rarely (1), sometimes (2) & always (3); maximum score =15.
This article is protected by copyright. All rights reserved.
Table 6: Overall level of patient/family satisfaction with care, by study group
Intervention Control Chi-square
Overall satisfaction level P value
(X2)
Accepted Article
N (%) N (%)
90-100% 0 (0.0) 0 (0.0)
80-89% 16 (53.3) 0 (0.0)
70-79% 14 (46.7) 0 (0.0) 60.0 0.001
60-69% 0 (0.0) 13 (43.3)
<60% 0 (0.0) 17 (56.7)
Total 30 (100.0) 30 (100.0)
This article is protected by copyright. All rights reserved.
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5814)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Adcs-Adl Mci v1 Annotated CRFDocument22 pagesAdcs-Adl Mci v1 Annotated CRFSara KingNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Science 37 (Site)Document28 pagesScience 37 (Site)Pro Business PlansNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- FDA Briefing Book - TOBIDocument135 pagesFDA Briefing Book - TOBISnigdha Santra SaxenaNo ratings yet
- BPS4102 Pharmaceuticals: Federal and International RegulationDocument41 pagesBPS4102 Pharmaceuticals: Federal and International RegulationFourat MuzielNo ratings yet
- Sex, Gender and Health BiotechnologyDocument7 pagesSex, Gender and Health BiotechnologymoonchildNo ratings yet
- Columbia Asia Referral HospitalDocument9 pagesColumbia Asia Referral HospitalNeerajNo ratings yet
- HaruyamaDocument10 pagesHaruyamabarros6No ratings yet
- Guided by DR Ravishankar DR Amit Tirth DR Vaibhav Tandon DR Smita Chandra Presented by Rituparna Bhowmick Bds Final YearDocument24 pagesGuided by DR Ravishankar DR Amit Tirth DR Vaibhav Tandon DR Smita Chandra Presented by Rituparna Bhowmick Bds Final YearAbhay TandonNo ratings yet
- Medicinal Mushrooms Their Therapeutic Properties and Current Medical Usage With Special Emphasis On Cancer Treatments 2002Document276 pagesMedicinal Mushrooms Their Therapeutic Properties and Current Medical Usage With Special Emphasis On Cancer Treatments 2002lordraffael100% (1)
- Mil STD 810cDocument274 pagesMil STD 810cAlphamanNo ratings yet
- McLean Hospital Annual Report 2011Document32 pagesMcLean Hospital Annual Report 2011mcleanhospitalNo ratings yet
- eXampleCG Strategy and Operations Excellence Consulting ServicesDocument44 pageseXampleCG Strategy and Operations Excellence Consulting ServicesexamplecgNo ratings yet
- Bioeq Rev-Oxcarbazepine TabsDocument55 pagesBioeq Rev-Oxcarbazepine TabsJagdish ChanderNo ratings yet
- Chapter 5Document4 pagesChapter 5Ian Dante ArcangelesNo ratings yet
- SOP On Handling of Out of Specification Results in Quality ControlDocument11 pagesSOP On Handling of Out of Specification Results in Quality ControlBejoy KarimNo ratings yet
- 8ED94d01 PDFDocument6 pages8ED94d01 PDFIlvita MayasariNo ratings yet
- Canadian GPC AnsiedadDocument83 pagesCanadian GPC AnsiedadFabiana FloresNo ratings yet
- CliniIndia: Clinical Data ManagementDocument5 pagesCliniIndia: Clinical Data ManagementAnuj TripathiNo ratings yet
- Are Current Clinical Studies On Artificial Intelligence-Based Medical DevicesDocument13 pagesAre Current Clinical Studies On Artificial Intelligence-Based Medical Devicesmgw backupdataNo ratings yet
- 508-Prowell-Final Slides5Document25 pages508-Prowell-Final Slides5dfsdjgflksjgnawNo ratings yet
- Maas 2007Document11 pagesMaas 2007Caroline FelicianoNo ratings yet
- Reishimax GLP Us PipDocument3 pagesReishimax GLP Us PipKeith KingNo ratings yet
- Pancreatic Cancer Therapeutics in Major Developed Markets To 2021Document7 pagesPancreatic Cancer Therapeutics in Major Developed Markets To 2021Kanchan JagtaniNo ratings yet
- Writing Guidelines FrywebDocument14 pagesWriting Guidelines FrywebH. DaasNo ratings yet
- Superiority, Equivalence, and Non-Inferiority TrialsDocument5 pagesSuperiority, Equivalence, and Non-Inferiority TrialscrystalmodelNo ratings yet
- 2 - Introduction To PharmacovigilanceDocument28 pages2 - Introduction To PharmacovigilanceHanan AhmedNo ratings yet
- The Truth About Hydrazine SulfateDocument4 pagesThe Truth About Hydrazine SulfateMichael FlynnNo ratings yet
- Khalitya (PPTminimizer)Document12 pagesKhalitya (PPTminimizer)Samhitha Ayurvedic ChennaiNo ratings yet
- GLP TrainerDocument268 pagesGLP TrainerAsep RNo ratings yet
- Medical OncologyDocument41 pagesMedical Oncologylavadey2No ratings yet